Surgical Management of Subungual Tumors & Exostoses

Key Takeaway
Subungual and periungual lesions, including fibromas, exostoses, and glomus tumors, present unique diagnostic and surgical challenges. Accurate diagnosis relies on clinical suspicion, advanced imaging, and recognizing systemic associations like tuberous sclerosis. Surgical management requires meticulous nail bed preservation, precise tumor excision, and strategic flap design to eradicate the pathology while minimizing postoperative nail dystrophy and ensuring optimal functional recovery.
Comprehensive Introduction and Patho-Epidemiology
The subungual space represents a highly specialized, anatomically constrained, and biomechanically unique microenvironment. The perionychium—comprising the nail plate, the sterile and germinal matrices, the proximal and lateral nail folds, and the hyponychium—serves critical physiologic functions. These include the facilitation of highly sensitive tactile discrimination, thermoregulation via complex microvascular networks, and the rigid mechanical protection of the terminal phalanx. Pathologic entities arising within this unyielding volumetric envelope, such as subungual fibromas, subungual exostoses, and glomus tumors, invariably present with disproportionate clinical symptomatology. The rigid dorsal boundary formed by the keratinized nail plate and the unyielding volar floor composed of the distal phalangeal cortex create a "closed compartment" effect, wherein even microscopic neoplastic proliferation generates intense pressure, ischemic pain, and subsequent nail dystrophy.
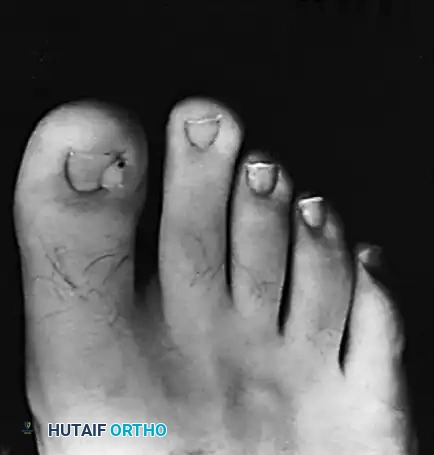
Diagnosing these lesions preoperatively remains an exceptionally challenging clinical endeavor, frequently resulting in delayed diagnosis and prolonged patient morbidity. Patients typically present with a protracted history of localized symptoms, having often consulted multiple primary care providers and specialists without definitive resolution or having been misdiagnosed with chronic paronychia or psychosomatic pain syndromes. The classical presentation of localized, exquisite tenderness beneath a specific, identifiable portion of the nail plate, accompanied by subtle chromatic alterations (erythematous or violaceous hues) and profound patient frustration, must immediately elevate the orthopedic surgeon's clinical index of suspicion for a subungual neoplasm.
Epidemiologically, the distribution of these tumors varies significantly based on the underlying histopathology. Glomus tumors, which are benign hamartomatous proliferations of the neuromyoarterial glomus apparatus, account for approximately 1% to 5% of all hand tumors but represent up to 75% of all subungual tumors. They exhibit a distinct predilection for females when occurring in the subungual space, typically presenting in the third to fifth decades of life. Conversely, subungual exostoses are benign, reactive osteocartilaginous outgrowths rather than true neoplasms. They predominantly afflict adolescents and young adults, with a striking predilection for the hallux, often precipitated by chronic microtrauma from restrictive footwear or prior acute traumatic events.
Subungual and periungual fibromas, while benign fibrous tissue tumors, carry profound systemic implications. Although isolated fibromas can occur spontaneously, their multifocal presence is highly pathognomonic for underlying systemic genetic disorders, most notably Tuberous Sclerosis Complex (TSC). Up to 80% of patients with TSC will develop ungual fibromas, clinically designated as Koenen tumors. These lesions typically manifest in post-pubertal cohorts and demonstrate a higher incidence in the pedal digits compared to the manual digits. The recognition of these lesions is not merely a localized orthopedic concern but a critical diagnostic gateway that necessitates comprehensive dermatologic, neurologic, and genetic screening to evaluate for associated systemic manifestations such as cortical tubers, subependymal giant cell astrocytomas, and renal angiomyolipomas.
Detailed Surgical Anatomy and Biomechanics
A profound, microscopic-level understanding of perionychial anatomy is the absolute prerequisite for the successful surgical management of subungual pathology. The nail complex, or perionychium, is divided into several distinct anatomical and functional zones. The germinal matrix, located proximally beneath the eponychium and extending distally to the lunula, is responsible for approximately 90% of nail plate generation. Any iatrogenic or neoplastic disruption of the germinal matrix will invariably result in permanent longitudinal ridging, splitting, or complete absence of the corresponding nail plate segment. The sterile matrix, extending from the distal margin of the lunula to the hyponychium, contributes to the adherence of the nail plate and adds a minimal amount of squamous material to the ventral surface of the nail, providing crucial structural integrity and thickness.
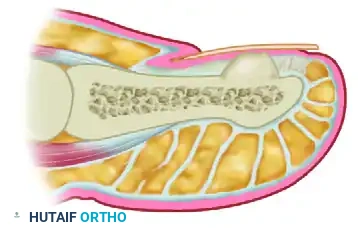
The osseous anatomy of the distal phalanx is intimately related to the overlying nail bed. The dorsal cortex of the distal phalanx is virtually devoid of intervening subcutaneous fat, meaning the periosteum is directly contiguous with the deep surface of the sterile matrix. This anatomical intimate relationship explains why expanding osseous lesions, such as subungual exostoses, rapidly distort the nail bed and elevate the nail plate. Biomechanically, the nail plate acts as a counter-force to the volar pulp during pinch and grip activities. When an exostosis expands dorsally, it creates a pathological pinch mechanism between the rigid shoe upper (or external environment) and the expanding bony mass, leading to pressure necrosis, ulceration of the sterile matrix, and secondary bacterial colonization.
The vascular anatomy of the subungual space is incredibly robust, supplied by the terminal arborizations of the proper palmar or plantar digital arteries. These vessels form a rich anastomotic arcade within the distal pulp and send perforating branches dorsally to supply the matrix. Within the reticular dermis of the nail bed lies a high concentration of glomus bodies (the Sucquet-Hoyer canals). These specialized neuromyoarterial structures function as highly efficient arteriovenous shunts, bypassing the capillary bed to regulate core body temperature through the dissipation or conservation of heat. A glomus tumor represents a localized, hyperplastic proliferation of the modified smooth muscle cells (glomus cells) surrounding these shunts.
Innervation of the perionychium is supplied by the terminal branches of the volar and dorsal digital nerves. The subungual space possesses one of the highest densities of nociceptors and thermoreceptors in the human body. This dense neural network, combined with the rigid boundaries of the nail plate and the distal phalanx, elucidates the pathophysiology of the excruciating, paroxysmal pain characteristic of subungual tumors. Even a microscopic glomus tumor, expanding by mere millimeters, will compress these highly sensitive nerve endings against the unyielding dorsal cortex of the phalanx or the ventral surface of the nail plate, triggering profound hyperalgesia and allodynia.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for subungual tumors and exostoses requires a meticulous risk-benefit analysis, balancing the necessity of tumor extirpation against the high risk of iatrogenic nail dystrophy. Absolute indications for surgical excision include intractable, paroxysmal pain that impairs activities of daily living (classic for glomus tumors), progressive nail deformity or matrix ulceration (frequently seen with subungual exostoses), recurrent secondary bacterial or fungal infections due to mechanical disruption of the hyponychial seal, and any lesion demonstrating rapid growth or suspicious characteristics warranting histopathological evaluation to rule out subungual melanoma or squamous cell carcinoma.
Relative indications encompass milder pain syndromes, cosmetic concerns related to nail plate elevation or discoloration, and the presence of asymptomatic periungual fibromas (Koenen tumors) that interfere with normal footwear or hygiene. In patients with Tuberous Sclerosis Complex, prophylactic excision of asymptomatic fibromas is generally discouraged due to the high rate of recurrence and the potential for creating painful postoperative scars; however, if the fibroma causes mechanical impingement or recurrent bleeding, marginal excision is justified.
Contraindications to definitive tumor extirpation are primarily related to the local physiological state of the digit and the patient's systemic health. Active, uncontrolled local infection (e.g., severe acute paronychia or deep space infection) is an absolute contraindication to definitive tumor excision; the infection must be eradicated with appropriate antimicrobial therapy and, if necessary, simple incision and drainage prior to definitive oncologic resection. Severe peripheral vascular disease (e.g., advanced diabetic microangiopathy or critical limb ischemia) represents a formidable relative contraindication, as the delicate flaps required for exposure may undergo ischemic necrosis, leading to catastrophic digital loss.
| Pathology | Primary Indications for Surgery | Relative/Absolute Contraindications | Biopsy / Pathology Requirement |
|---|---|---|---|
| Glomus Tumor | Intractable paroxysmal pain, cold hypersensitivity, positive Hildreth's/Love's tests. | Severe peripheral arterial disease; active untreated local digital infection. | Excisional biopsy is standard; definitive histopathology required to confirm hamartoma. |
| Subungual Exostosis | Painful nail elevation, ulceration of sterile matrix, inability to wear closed shoes. | Asymptomatic incidental finding on plain radiographs (Observation preferred). | Excisional biopsy required to differentiate from true osteochondroma or malignant sarcoma. |
| Subungual Fibroma | Mechanical impingement, recurrent bleeding, severe nail plate distortion. | Asymptomatic lesions in confirmed Tuberous Sclerosis (high recurrence rate). | Histopathology mandatory to confirm benign fibrous proliferation and rule out malignancy. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative clinical evaluation is the cornerstone of successful surgical management. For suspected glomus tumors, the clinical examination must include three classic provocative tests. Love’s pin test involves using the blunt end of a paperclip or a smooth Kirschner wire to apply pinpoint pressure systematically across the nail plate; a sharp, excruciating withdrawal response precisely localizes the tumor. Hildreth’s test involves inflating a pneumatic tourniquet at the base of the digit or the proximal arm; if the localized pain elicited by Love's test is completely abolished during ischemia, the test is positive and highly specific for a vascular glomus tumor. Finally, the cold sensitivity test, performed by applying an ice cube or cold saline syringe to the digit, will provoke severe, lingering pain in the presence of a glomus tumor.
Advanced imaging is highly recommended, and often mandatory, prior to surgical exploration. Because the nail plate frequently appears entirely normal, blind exploration based solely on clinical symptoms is fraught with high failure and recurrence rates. High-resolution Magnetic Resonance Imaging (MRI) with a dedicated superficial surface coil is the gold standard for preoperative localization of soft tissue subungual masses. On T2-weighted MRI sequences, a glomus tumor characteristically appears as a hyperintense, well-demarcated, ovoid lesion. MRI not only confirms the diagnosis but precisely maps the tumor's location (e.g., central, lateral, or proximal beneath the germinal matrix), dictating the optimal surgical approach. For subungual exostoses, standard orthogonal plain radiographs of the digit are usually sufficient, demonstrating a trabeculated bony outgrowth extending dorsally from the distal phalanx without continuity of the medullary canal.

Anesthetic management and patient positioning must be meticulously planned to ensure a bloodless, magnified surgical field. Procedures are typically performed on an outpatient basis under a comprehensive digital block utilizing 1% plain lidocaine mixed with 0.5% bupivacaine for prolonged postoperative analgesia. Epinephrine should generally be avoided in the digital block to prevent vasospasm, though some modern literature supports its safe use in healthy digits. A sterile digital tourniquet (such as a rolled surgical glove or a dedicated sterile Penrose drain) is applied at the base of the digit after exsanguination with an Esmarch bandage.
The patient is positioned supine. For upper extremity lesions, a standard radiolucent hand table is utilized. For lower extremity lesions, the patient is positioned with the foot extending slightly over the edge of the operating table, supported by a padded bump. Magnification is absolutely non-negotiable. The surgeon must utilize surgical loupes with a minimum magnification of 2.5x to 3.5x, supplemented by a high-intensity coaxial headlight. In cases of recurrent glomus tumors or extremely proximal lesions involving the germinal matrix, the use of an operating microscope may be indicated to ensure complete tumor extirpation while preserving the microscopic anatomy of the perionychium.
Step-by-Step Surgical Approach and Fixation Technique
Surgical Technique 87-13: Excision of Subungual Fibroma
The primary surgical objective in managing a subungual fibroma is complete tumor eradication with marginal excision, while meticulously minimizing iatrogenic trauma to the adjacent normal germinal and sterile matrices. Following the establishment of a bloodless field via digital tourniquet, the surgeon must first address the overlying nail plate. If the fibroma is located entirely beneath the nail, a partial longitudinal nail avulsion is performed. Using a Freer elevator, the nail plate is gently separated from the underlying sterile matrix and the overlying eponychium. A straight hemostat or nail splitter is then used to avulse only the portion of the nail plate directly overlying the symptomatic mass.
Under loupe magnification, the fibroma is identified. It typically presents as a firm, pearly-white or pale-pink nodule that is visually and texturally distinct from the surrounding highly vascularized, pink sterile matrix. Using a #15 or #67 Beaver blade, the tumor is excised sharply. The incision must carry down completely to the periosteum of the distal phalanx. It is imperative to include a microscopic 1- to 2-mm margin of macroscopically normal-appearing matrix tissue to mitigate the risk of local recurrence. Once excised, the subungual fibroma characteristically exhibits a dense, "gritty" resistance when sectioned on the back table. The resulting matrix defect is generally left open to heal by secondary intention, covered only with a non-adherent dressing (e.g., Xeroform or Adaptic). Primary closure is rarely possible without inducing undue tension and subsequent matrix deformity.
Subungual Exostosis Resection: Minimalist Approach (Lokiec et al.)
For smaller, well-localized exostoses that have not completely destroyed the overlying nail bed, a tissue-sparing approach (Technique 87-11) is highly advantageous to preserve the maximum amount of native nail plate.

The procedure begins by identifying the exact location of the exostosis. A narrow, longitudinal strip of the nail plate directly over the medial or lateral aspect of the exostosis is sharply removed. The remaining nail plate is then carefully dislodged and elevated from the matrix, utilizing it as a biological shield rather than discarding it. This exposure reveals the underlying distorted nail bed and the palpable bony mass beneath it.
A small, sharp osteotome is introduced into the defect. The osteotome must be positioned precisely parallel to the longitudinal axis of the distal phalanx. With controlled mallet strikes, the exostosis is resected flush with the host bone of the dorsal cortex in a single, contiguous piece. Care must be taken not to violate the distal interphalangeal joint proximally or to fracture the tuft distally. The resected bone is sent for histopathological analysis.

Following copious irrigation of the bony bed to remove any osteocartilaginous debris, the preserved native nail plate is relocated to its anatomical position. It is used to cover the raw phalangeal bone and the incised matrix, effectively acting as a rigid, custom-molded biologic dressing. The nail plate is secured in place using non-absorbable 4-0 nylon sutures placed through the distal hyponychium and the lateral nail folds.
Subungual Exostosis Resection: Formal Excision (Walling)
For massive exostoses, recurrent lesions, or those that have severely distorted and ulcerated through the nail bed, the formal exposure technique (Technique 87-12) described by Walling is required to ensure complete eradication and adequate matrix repair.
The procedure commences with a complete, atraumatic avulsion of the entire toenail or fingernail. A Freer elevator is swept beneath the nail plate, taking care to stay strictly in the subungual plane to avoid gouging the sterile matrix. A straight hemostat is then used to roll the nail plate off the digit, fully exposing the exostosis and the severely distorted, often thinned, overlying nail bed.
A precise, longitudinal incision is made directly through the center of the nail bed, directly over the maximum prominence of the exostosis. The surgeon must exercise extreme caution to strictly avoid extending this incision proximally into the germinal matrix or the eponychial fold, which would guarantee a permanent split-nail deformity.
Using fine skin hooks or 6-0 stay sutures, the incised nail bed is carefully reflected medially and laterally. The sterile matrix is often intimately adherent to the osteocartilaginous cap of the exostosis, requiring meticulous sharp dissection with a #15 blade to elevate the matrix flaps without buttonholing or macerating the delicate tissue.

Once the base of the exostosis is fully delineated, it is excised at its origin using a rongeur or a sharp osteotome. The excision must include wide margins, taking a small layer of normal underlying cortical bone to ensure no cartilaginous cap remnants are left behind, which is the primary cause of recurrence. The residual bony crater is smoothed with a high-speed diamond burr or a rasp. The nail bed flaps are then allowed to fall back together. Because the underlying mass has been removed, there is often redundant matrix tissue. The matrix is meticulously repaired using 6-0 absorbable sutures (e.g., chromic gut or Vicryl Rapide) in a tension-free manner.
Glomus Tumor Extirpation via Full-Thickness Flap (Horst and Nunley)
Historically, transungual approaches to glomus tumors resulted in unacceptably high rates of permanent nail deformity. Horst and Nunley revolutionized the management of these lesions by describing an advanced, matrix-sparing technique utilizing a full-thickness vascular skin flap.

The incision design is critical. The surgeon marks an inverted L-shaped incision around the affected nail. The short transverse leg of the "L" runs parallel to, and exactly 5 mm distal to, the distal edge of the nail (the hyponychium). The long longitudinal leg of the "L" runs 5 mm medial or lateral to the nail fold (depending on the tumor's location as mapped by MRI). This longitudinal incision extends proximally past the entire nail matrix, typically terminating at the level of the distal interphalangeal (DIP) joint flexion crease.
Elevation of the flap must be performed in a single, full-thickness layer directly down to the periosteum of the distal phalanx. Using a #15 blade, the surgeon sharply and meticulously elevates this composite flap—containing the skin, subcutaneous tissue, entire nail plate, and the intact sterile and germinal matrices—off the dorsal cortex of the distal phalanx. It is absolutely critical to maintain the plane directly on the bone to avoid penetrating or injuring the deep surface of the nail matrix.
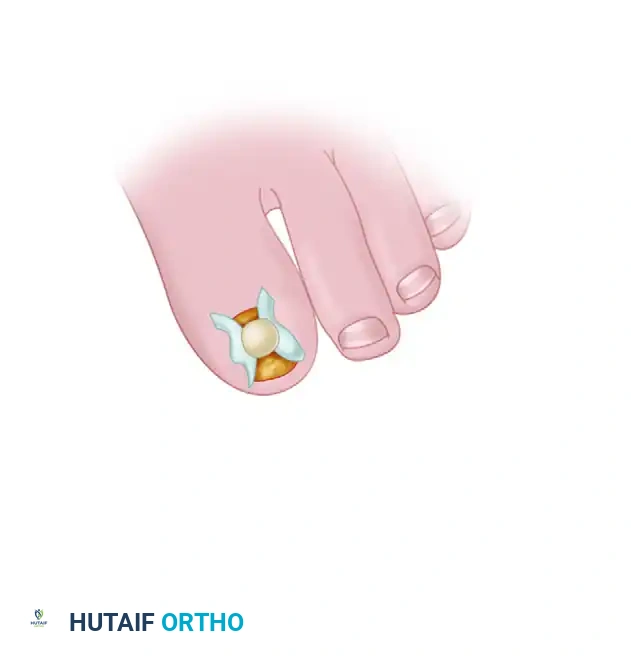
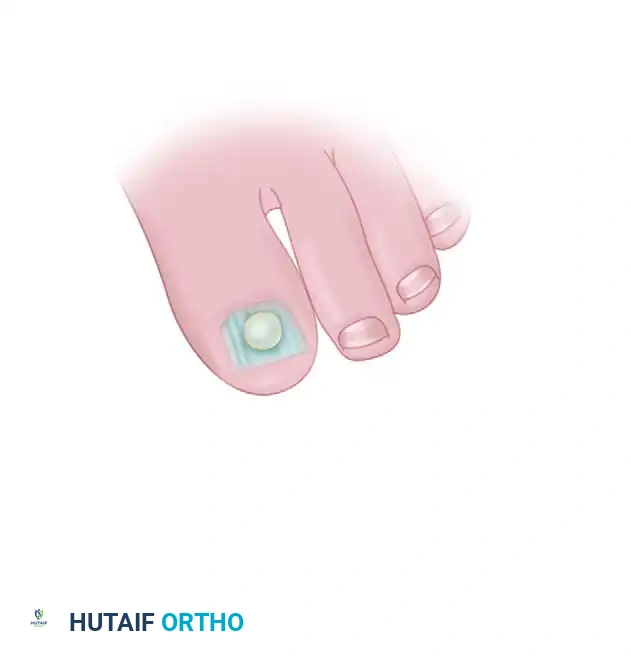
Once elevated, the composite flap is reflected dorsally and laterally. The surgeon inspects the deep (volar) surface of the reflected flap. The glomus tumor is typically glaringly obvious within the sub-matrix tissue. It appears as a distinct, ball-shaped or egg-shaped, opaque, semi-elastic structure with a characteristic bluish-red or violaceous hue. The tumor is usually well-encapsulated. Using a fine curette or a #67 Beaver blade, the tumor is shelled out completely. The surgeon must handle the tumor delicately to avoid breaching its capsule, which could lead to cellular seeding and recurrence.
Following excision, the dorsal cortex of the phalanx is inspected for any smooth, scalloped erosions caused by chronic pulsatile pressure from the tumor. The digital tourniquet is released prior to closure to ensure absolute hemostasis. Reactive bleeding is controlled meticulously with pinpoint bipolar electrocautery; monopolar cautery is strictly forbidden in this area due to the risk of thermal necrosis to the matrix. The full-thickness flap is then laid back into its anatomical position and secured with interrupted 5-0 or 6-0 nylon sutures.
Complications, Incidence Rates, and Salvage Management
The surgical management of subungual tumors is fraught with potential complications, primarily due to the unforgiving nature of the perionychial anatomy. The most frequent and distressing complication for the patient is postoperative nail dystrophy. This can manifest as longitudinal ridging, a permanent split nail, or non-adherence of the nail plate to the sterile matrix (onycholysis). Dystrophy is almost always the result of iatrogenic injury to the germinal matrix during exposure or overly aggressive electrocautery.
Tumor recurrence is another significant challenge. For glomus tumors, recurrence rates range from 5% to 15% in historical series, often due to the failure to identify multiple satellite lesions or incomplete marginal excision. Recurrent glomus tumors present a diagnostic dilemma, as the recurrent pain must be differentiated from postoperative neuroma or Complex Regional Pain Syndrome (CRPS). High-resolution MRI with gadolinium contrast is essential to identify recurrent tumor nodules.
Infection and wound healing complications, including subungual hematoma, can compromise the viability of the nail bed flaps. A rapidly expanding subungual hematoma creates intense pressure, causing severe pain and potential ischemic necrosis of the delicate matrix repair. Meticulous hemostasis prior to closure and the application of a properly designed non-compressive dressing are critical preventative measures.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Secondary Intervention |
|---|---|---|---|
| Nail Dystrophy (Split/Ridge) | 10% - 25% (Transungual) <2% (Flap approach) |
Iatrogenic injury to germinal matrix; excessive thermal necrosis from cautery. | Matrix reconstruction with split-thickness sterile matrix graft; permanent matrixectomy for severe cases. |
| Tumor Recurrence (Glomus) | 5% - 15% | Incomplete excision; presence of unrecognized satellite lesions; capsular breach. | Re-evaluation with contrast MRI; revision excision using operating microscope for magnification. |
| Recurrence (Exostosis) | 10% - 20% | Failure to remove the entire cartilaginous cap; inadequate bony margins. | Revision formal excision with aggressive burring of the phalangeal dorsal cortex. |
| Subungual Hematoma | 5% - 10% | Inadequate hemostasis after tourniquet release; overly tight wound closure. |
