Mastering Benign Bone Tumors: Osteoblastoma, Chondromyxoid Fibroma, and Langerhans Cell Histiocytosis

Key Takeaway
Osteoblastoma is a rare, bone-forming neoplasm predominantly affecting the posterior elements of the spine in young adults. It presents with localized pain and potential neurological deficits. Management requires meticulous extended curettage or marginal resection, often necessitating complex spinal reconstruction. Langerhans cell histiocytosis, presenting frequently as vertebra plana or lytic lesions, is generally managed conservatively or with intralesional corticosteroid injection, reserving surgical decompression for progressive neurological compromise.
Comprehensive Introduction and Patho-Epidemiology
The diagnosis, classification, and management of benign bone tumors and tumor-like conditions require a rigorous, multidisciplinary approach encompassing orthopedic oncology, musculoskeletal radiology, and molecular pathology. While these lesions lack the metastatic potential characteristic of sarcomas, their local biological behavior spans a broad spectrum—from entirely quiescent, asymptomatic incidentalomas to highly aggressive, locally destructive lesions. This aggressive local behavior can lead to severe structural compromise, catastrophic neurological deficits (particularly in the axial skeleton), and profound patient morbidity. This comprehensive masterclass details the pathophysiology, epidemiology, and molecular basis of three distinct entities: Osteoblastoma, Chondromyxoid Fibroma (CMF), and Langerhans Cell Histiocytosis (LCH). Understanding the cellular origins and genetic drivers of these lesions is paramount for accurate diagnosis and the formulation of an optimal surgical strategy.
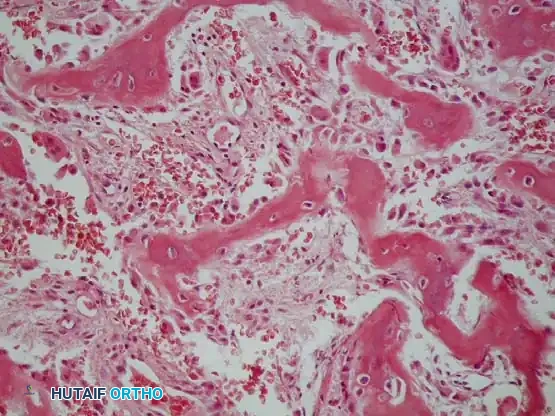
Osteoblastoma is a rare, primary bone-forming neoplasm, accounting for less than 1% of all primary bone tumors. It predominantly affects adolescents and young adults, with a peak incidence occurring strictly between the first and third decades of life (10 to 30 years of age). There is a distinct male predominance, with a male-to-female ratio approaching 3:1. Pathophysiologically, osteoblastoma is characterized by the proliferation of a highly vascularized, fibrovascular stroma that produces abundant, disorganized osteoid and primitive woven bone. Recent advancements in molecular pathology have revolutionized our understanding of osteoblastoma, revealing that a significant majority of these tumors harbor recurrent rearrangements of the FOS or FOSB genes. These genetic aberrations lead to the overexpression of c-Fos, a transcription factor that plays a critical role in osteoblast differentiation and bone formation, thereby driving the neoplastic proliferation of osteoblasts.


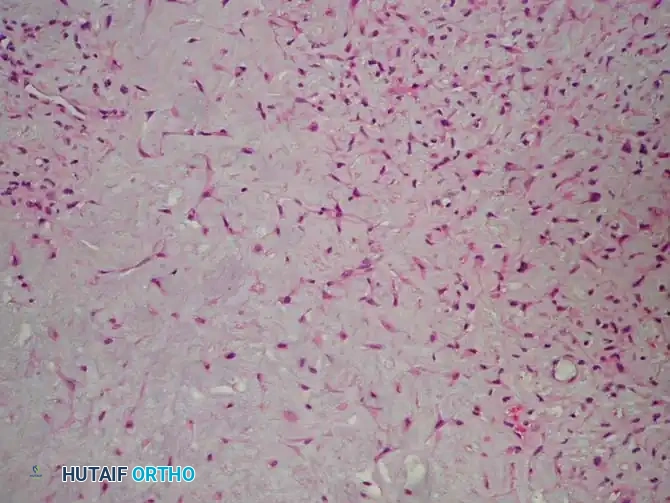
Chondromyxoid Fibroma (CMF) is another exceptionally rare benign bone tumor, representing approximately 0.5% of all primary bone neoplasms. Like osteoblastoma, it typically presents in the second and third decades of life. CMF is of chondroid origin and is histologically defined by a lobular architecture comprising an admixture of chondroid, myxoid, and fibrous tissues. The exact cellular lineage has historically been debated, but contemporary cytogenetic studies have identified recurrent chromosomal translocations involving the GRM1 (Glutamate Receptor, Metabotropic 1) gene on chromosome 6q24. The upregulation of GRM1 alters cellular signaling pathways, promoting the aberrant proliferation of chondromyxoid stromal cells. This molecular signature is highly specific to CMF and serves as a crucial diagnostic adjunct when differentiating CMF from chondrosarcoma or other cartilaginous lesions.
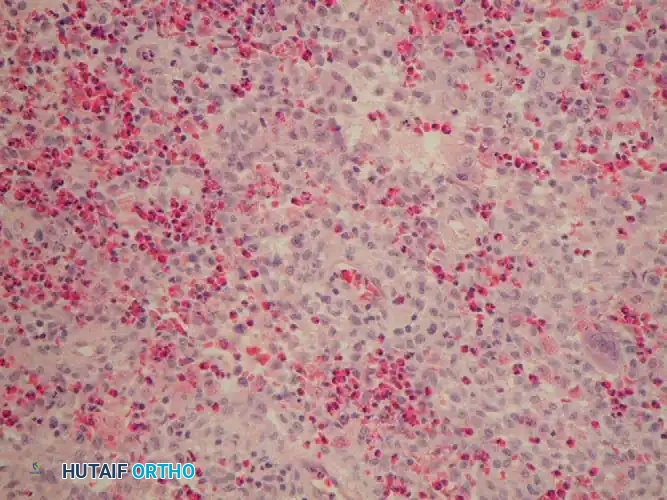
Langerhans Cell Histiocytosis (LCH), formerly known as Histiocytosis X, encompasses a spectrum of idiopathic disorders characterized by the clonal proliferation of aberrant Langerhans cells. The disease can affect virtually any organ system but most frequently involves the skeletal system, presenting as Eosinophilic Granuloma in its localized form. Eosinophilic granuloma typically affects children and young adults between 5 and 20 years of age. The pathophysiology of LCH has undergone a paradigm shift; once considered a reactive immune disorder, it is now definitively classified as an inflammatory myeloid neoplasm. This reclassification is driven by the discovery that up to 60% of LCH lesions harbor the BRAF V600E somatic mutation, which constitutively activates the MAPK/ERK signaling pathway, driving the uncontrolled proliferation of pathologic histiocytes and the subsequent recruitment of a robust inflammatory infiltrate, including eosinophils, macrophages, and multinucleated giant cells.
Detailed Surgical Anatomy and Biomechanics
The surgical management of benign bone tumors is heavily dictated by their anatomical location and the biomechanical role of the host bone. Osteoblastoma exhibits a striking predilection for the axial skeleton. Approximately 40% to 50% of all osteoblastomas are located in the spine, almost exclusively originating in the posterior elements—specifically the spinous processes, laminae, pedicles, and articular facets. Biomechanically, the posterior elements of the spine function as the primary tension band during flexion and provide critical rotational and translational stability via the facet joints. The expansile nature of osteoblastoma in this region often destroys the facet capsule and pars interarticularis, leading to localized instability. Furthermore, the tumor's proximity to the spinal cord and exiting nerve roots creates a high-risk neurovascular environment. Surgical resection almost inevitably requires the iatrogenic disruption of these posterior stabilizing structures, mandating concurrent instrumented spinal arthrodesis to prevent progressive kyphotic deformity and spondylolisthesis.

In the appendicular skeleton, Chondromyxoid Fibroma demonstrates a strong affinity for the metaphyseal regions of major long bones, particularly the proximal tibia, distal femur, and distal radius. The proximal tibial metaphysis is a critical load-bearing zone, subject to massive compressive forces during the stance phase of gait and complex torsional forces during pivoting activities. CMF typically presents as an eccentric, sharply circumscribed, osteolytic lesion that causes endosteal scalloping and asymmetrical cortical expansion. This eccentric cortical thinning creates a significant stress riser, drastically reducing the bone's polar moment of inertia and predisposing the patient to pathologic fracture under minimal physiologic loads. The surgical anatomy here is further complicated by the proximity of the lesion to the physis in skeletally immature patients, necessitating meticulous surgical technique to avoid physeal arrest and subsequent angular deformity or limb length discrepancy.


Langerhans Cell Histiocytosis is renowned as the "great imitator" due to its ubiquitous anatomical distribution and variable radiographic appearance. In the spine, LCH is the most common cause of vertebra plana—a severe, uniform flattening of the vertebral body. Biomechanically, the vertebral body is the primary anterior column support, responsible for bearing up to 80% of axial compressive loads. Despite the catastrophic radiographic appearance of vertebra plana, the posterior elements and intervertebral discs typically remain completely intact. This unique anatomical preservation means that, remarkably, the spine often remains mechanically stable, and the vertebral body frequently undergoes spontaneous reconstitution over time. In the appendicular skeleton, diaphyseal LCH lesions often exhibit an aggressive, permeative pattern of bone destruction with robust, lamellated periosteal reaction, mimicking acute osteomyelitis or Ewing sarcoma. These diaphyseal lesions compromise the cortical cylinder, significantly reducing the bone's resistance to bending and torsional moments.

When planning surgical intervention for any of these lesions, the orthopedic oncologist must possess an intimate understanding of the surrounding soft tissue envelopes and neurovascular bundles. For instance, extended curettage of a proximal tibial CMF requires careful navigation of the anterior tibial neurovascular bundle and the common peroneal nerve, particularly if the lesion extends laterally towards the fibular head. Similarly, resection of a cervical spine osteoblastoma demands meticulous exposure of the vertebral artery, which may be encased or displaced by the expansile tumor mass. The biomechanical reconstruction must be tailored to the specific anatomical defect, utilizing rigid internal fixation and structural bone grafting to immediately restore load-bearing capacity and facilitate early postoperative mobilization.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for benign bone tumors is a complex calculus that balances the natural history of the specific lesion against the inherent risks of surgery. Operative indications are primarily driven by the presence of intractable pain, the risk of impending pathologic fracture, progressive neurological deficit, and the biological aggressiveness of the tumor. Because osteoblastoma, CMF, and LCH possess distinctly different clinical trajectories, the indications for surgical management are highly specific to each entity. A thorough understanding of these indications, as well as strict adherence to contraindications, is essential to avoid unnecessary morbidity and optimize patient outcomes.
For Osteoblastoma, surgical intervention is almost universally indicated. These tumors are biologically active, continuously growing, and possess a well-documented, albeit rare, potential for aggressive local behavior and even malignant transformation into osteosarcoma. The hallmark symptom is unremitting, progressive pain that is classically unresponsive to nonsteroidal anti-inflammatory drugs (NSAIDs)—a key clinical feature distinguishing it from osteoid osteoma. In the spine, osteoblastoma frequently induces a painful, rigid scoliosis or torticollis, and the expansile mass can cause direct compression of the spinal cord or nerve roots, leading to myelopathy or radiculopathy. Therefore, the primary indications for surgical resection of osteoblastoma include the relief of severe pain, the decompression of compromised neural elements, the correction of secondary spinal deformity, and the prevention of further local tissue destruction.
| Condition / Tumor | Primary Surgical Indications | Absolute & Relative Contraindications |
|---|---|---|
| Osteoblastoma | Intractable pain unresponsive to NSAIDs; Progressive neurological deficit (myelopathy/radiculopathy); Impending structural failure; Secondary painful scoliosis. | Absolute: Medical instability precluding anesthesia. Relative: Asymptomatic incidentaloma (exceedingly rare); Inability to achieve safe margins without catastrophic neurological injury (consider embolization/medical management). |
| Chondromyxoid Fibroma | Symptomatic pain; Eccentric cortical destruction causing a high risk of pathologic fracture; Lesion expansion on serial imaging; Need for definitive histopathologic diagnosis. | Absolute: Active overlying soft tissue infection. Relative: Skeletally immature patient where curettage guarantees massive physeal destruction (requires highly specialized pediatric oncology approach). |
| Langerhans Cell Histiocytosis | Diagnostic biopsy required to rule out malignancy/infection; Impending/actual pathologic fracture in a long bone; Progressive neurological deficit in spinal LCH (rare). | Absolute: Asymptomatic vertebra plana without neurological deficit (observation is standard). Relative: Systemic, multisystem LCH (Letterer-Siwe disease) requiring primary systemic chemotherapy prior to local intervention. |
Chondromyxoid Fibroma is similarly treated with a proactive surgical approach. The natural history of CMF is one of progressive, localized bone destruction. If left untreated, the eccentric expansion of the tumor will inevitably compromise the structural integrity of the metaphysis, leading to a pathologic fracture. Furthermore, because the radiographic appearance of CMF can occasionally mimic more aggressive lesions such as chondrosarcoma or giant cell tumor of bone, surgical intervention is often indicated to obtain a definitive histopathological diagnosis. The standard indication is a symptomatic lesion that demonstrates cortical thinning or expansion, necessitating extended intralesional curettage and prophylactic stabilization to restore the biomechanical integrity of the affected limb.
Conversely, the indications for surgical intervention in Langerhans Cell Histiocytosis are significantly more conservative. Isolated eosinophilic granuloma of bone is frequently a self-limiting condition that may undergo spontaneous resolution, particularly following a simple core needle biopsy or intralesional corticosteroid injection. In the spine, the classic vertebra plana is typically managed conservatively with bracing and observation, as the anterior column often reconstitutes and neurological compromise is exceptionally rare. Surgical intervention in LCH is strictly reserved for specific, high-risk scenarios: obtaining diagnostic tissue when the presentation mimics Ewing sarcoma or osteomyelitis, stabilizing an impending or complete pathologic fracture in a major load-bearing long bone, or performing neural decompression in the rare event of retropulsed bone causing epidural compression.

Pre-Operative Planning, Templating, and Patient Positioning
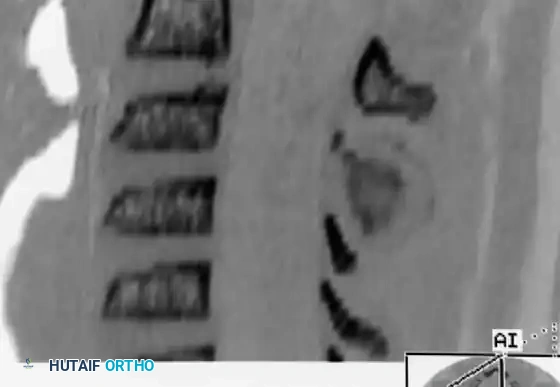
Flawless execution of orthopedic oncology procedures begins long before the initial incision. Exhaustive preoperative planning is the cornerstone of successful tumor resection, minimizing intraoperative surprises, reducing blood loss, and ensuring the complete eradication of neoplastic tissue while preserving maximal host biology. The planning phase relies heavily on advanced, multimodality imaging. Plain radiographs provide the initial assessment of the lesion's matrix, margins, and the overall mechanical axis of the limb or spine. However, high-resolution Computed Tomography (CT) is absolutely mandatory for surgical templating. CT exquisitely delineates the osseous margins, the precise extent of cortical destruction, and the presence of matrix mineralization. For spinal osteoblastomas, CT allows the surgeon to map the exact relationship of the tumor to the pedicles, facets, and vertebral foramina.
Magnetic Resonance Imaging (MRI) with and without intravenous gadolinium contrast is equally indispensable. MRI defines the true intraosseous extent of the tumor, identifying any skip lesions or marrow edema, and critically evaluates the soft tissue envelope. In the spine, MRI is the gold standard for assessing spinal cord compression, epidural tumor extension, and the patency of the vertebral arteries. Furthermore, because osteoblastomas are highly vascular neoplasms, preoperative diagnostic angiography with selective arterial embolization is strongly recommended for large spinal, pelvic, or sacral lesions. Embolization, performed 24 to 48 hours prior to surgery, induces tumor necrosis and dramatically reduces intraoperative hemorrhage, transforming a potentially life-threatening resection into a controlled, meticulous dissection.
Three-dimensional (3D) templating and intraoperative navigation have become standard of care in modern orthopedic oncology. Using the preoperative CT data, surgeons can generate 3D models to virtually simulate the resection planes and plan the optimal trajectory for reconstructive hardware. In complex pelvic or spinal resections, patient-specific cutting guides (PSIs) can be 3D-printed to ensure precise marginal resections. Intraoperative navigation systems, such as the O-arm coupled with stereotactic optical tracking, provide real-time, three-dimensional feedback, allowing the surgeon to confirm complete tumor excision and safely place pedicle screws or pelvic instrumentation in the setting of distorted, pathologically altered anatomy.

Patient positioning is a critical, yet often underappreciated, component of the surgical plan. For spinal osteoblastomas, the patient is meticulously positioned prone on a radiolucent Jackson spinal table. This positioning allows the abdomen to hang free, reducing intra-abdominal pressure and consequently decreasing epidural venous bleeding. The head is secured in a Mayfield skull clamp or a specialized foam face mask, ensuring neutral cervical alignment. For extremity lesions such as a proximal tibial CMF, the patient is positioned supine on a fully radiolucent operative table. A sterile pneumatic tourniquet is applied to the proximal thigh to provide a bloodless surgical field, which is essential for identifying microscopic tumor lobulations during extended curettage. The limb is prepped and draped free to allow intraoperative manipulation and multi-planar fluoroscopic assessment of the mechanical axis and hardware trajectory.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution for benign bone tumors requires a delicate balance between aggressive oncologic clearance and the preservation of functional host anatomy. The treatment of choice for Osteoblastoma is extended intralesional curettage or, preferably, marginal en bloc resection. When located in the posterior elements of the spine, a marginal resection is strongly advocated to minimize the risk of local recurrence. The patient is positioned prone, and a standard midline posterior approach is utilized. Subperiosteal dissection must be performed with extreme caution; the surgeon must avoid penetrating the highly vascular, thinned cortical shell of the tumor, which can precipitate massive hemorrhage. Using intraoperative navigation or fluoroscopy, the exact spinal levels are identified.
For a posterior element osteoblastoma, an en bloc resection (e.g., laminectomy and spinous process excision) is performed. A high-speed diamond burr is utilized to carefully disconnect the posterior elements from the pedicles, staying strictly outside the tumor capsule. Once the bony attachments are released, the ligamentum flavum is meticulously resected, and the dura and exiting nerve roots are fully decompressed. Because the resection of the posterior elements, pars interarticularis, and facets creates profound iatrogenic instability, an instrumented posterolateral fusion is universally required. Depending on the level, lateral mass screws (cervical spine) or pedicle screws (thoracolumbar spine) are placed using navigation guidance. The neural elements are protected, and the posterolateral gutters are decorticated and grafted with a combination of structural allograft and osteoinductive autograft to ensure a robust arthrodesis.


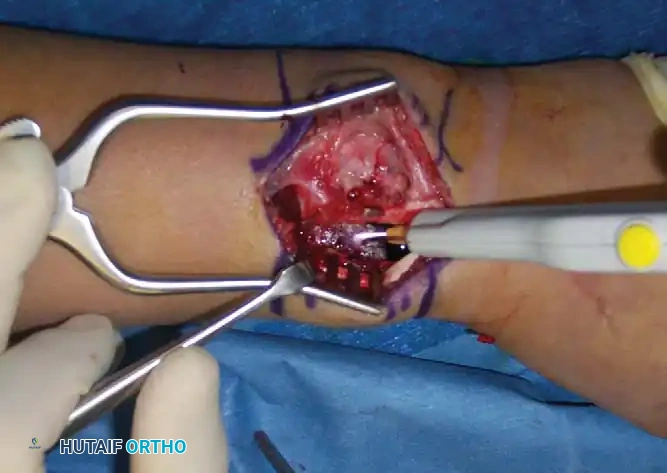
For Chondromyxoid Fibroma, the gold standard of treatment is extended intralesional curettage augmented with local chemical or thermal adjuvants. Simple curettage carries an unacceptably high recurrence rate of up to 25%. The surgical approach involves creating a generous cortical window over the lesion to allow complete, unhindered visualization of the tumor cavity. The macroscopic tumor is systematically removed using progressively smaller, angled curettes, ensuring that all cartilaginous lobulations and deep recesses are cleared. Once gross total resection is achieved, a high-speed burr is used to aggressively remove an additional 1 to 2 millimeters of reactive bone from the entire cavity wall. This "burr-down" technique breaks the microscopic tumor extensions that reside in the surrounding cancellous bone.
Following burring, the cavity must be sterilized using an adjuvant. Argon beam coagulation is highly effective and widely preferred; it delivers a stream of argon gas that conducts high-frequency electrical current, providing uniform thermal necrosis of the cavity walls with a minimal depth of penetration (1-2 mm), thereby protecting adjacent vital structures such as the physis or articular cartilage. Alternatively, anhydrous phenol followed by alcohol lavage can be utilized. The resulting massive bony void must then be reconstructed to restore structural integrity. The sterilized cavity is meticulously packed with a calcium phosphate bone graft substitute, autograft, or allograft. If the cortical destruction exceeds 50% of the bone's circumference, prophylactic internal fixation with a locking plate is mandated to prevent postoperative pathologic fracture.

The surgical management of Langerhans Cell Histiocytosis is generally less aggressive. For isolated eosinophilic granuloma of the appendicular skeleton, a minimally invasive approach is preferred. A Jamshidi needle or a small cortical window is used to obtain a diagnostic biopsy. Once the diagnosis is confirmed via frozen section, the lesion may undergo limited curettage. Often, the simple act of disrupting the lesion's microenvironment through biopsy is sufficient to induce healing. Intralesional injection of methylprednisolone is a highly effective adjunct that promotes rapid ossification of the lytic defect. In cases where the LCH lesion has caused massive cortical destruction in a weight-bearing bone, the cavity is curetted, grafted, and prophylactically stabilized with intramedullary nailing or plate osteosynthesis to permit immediate weight-bearing.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the management of benign bone tumors is fraught with potential complications. These complications can be broadly categorized into oncologic failures (local recurrence), structural and biomechanical failures (hardware pullout, pathologic fracture, pseudarthrosis), and neurovascular injuries. The incidence of these complications varies significantly based on the tumor histology, anatomical location, and the adequacy of the initial surgical resection. A comprehensive understanding of these risks and the appropriate salvage pathways is essential for the orthopedic oncologist.
Local recurrence is the most pressing oncologic concern. For Osteoblastoma, the recurrence rate ranges from 10% to 20%, almost exclusively occurring in cases where only an intralesional curettage was performed rather than a marginal resection. Recurrent osteoblastomas can be exceptionally aggressive, rapidly destroying local anatomy and complicating revision surgery due to altered landmarks and epidural scarring. For Chondromyxoid Fibroma, the historical recurrence rate following simple curettage was as high as 25%; however, with the modern application of high-speed burring and argon beam coagulation, this rate has plummeted to less than 5%. Recurrences of CMF typically present as progressive osteolysis at the margin of the bone graft and require immediate re-operation with wider margins and repeat adjuvant application.
| Complication Category | Specific Complication | Incidence Rate | Salvage Management Strategy |
|---|---|---|---|
| Oncologic Failure | Local Recurrence (Osteoblastoma) | 10% - 20% (Intralesional) | Revision marginal resection; Preoperative embolization; Extension of spinal fusion construct. |
| Oncologic Failure | Local Recurrence (CMF) | <5% (with adjuvants) | Repeat extended curettage; Aggressive argon beam coagulation; Structural bone grafting. |
| Biomechanical | Pathologic Fracture / Hardware Failure | 5% - 10% | Revision internal fixation (longer locking plates or intramedullary nails); Autogenous bone grafting for non-union. |
| Neurological | Dural Tear / CSF Leak (Spine) | 3% - 8% | Primary dural repair (6-0 Prolene); Fibrin glue sealant; Lumbar subarachnoid drain; Flat bedrest. |
| Malignant | Sarcomatous Transformation | <1% (Osteoblastoma) | Radical en bloc resection; Neoadjuvant/Adjuvant chemotherapy protocols for Osteosarcoma. |
Structural complications are prevalent, particularly following the resection of large metaphyseal lesions or complex spinal reconstructions. In the spine, pseudarthrosis (failure of fusion) can occur in up to 10% of cases, leading to hardware fatigue, screw breakage, and progressive deformity. Salvage requires revision surgery, meticulous decortication, and the application of potent osteoinductive agents such as Bone Morphogenetic Protein-2 (rhBMP-2). In the appendicular skeleton, the use of rigid calcium phosphate cements in CMF reconstruction can occasionally lead to stress shielding or delayed incorporation, predisposing the bone to fracture at the cement-bone interface.
A rare but catastrophic complication is the malignant transformation of a benign bone tumor. While exceedingly uncommon, cases of "aggressive osteoblastoma" undergoing transformation into low-grade or conventional osteosarcoma have been documented. This risk is profoundly elevated if the patient was previously subjected to radiation therapy. For this reason, radiation is strictly contraindicated for osteoblastoma and CMF, reserved only for anatomically inoperable lesions where surgical morbidity would be fatal. If malignant transformation occurs, the salvage management immediately shifts to a sarcoma protocol, necessitating neoadjuvant chemotherapy, radical wide resection with negative margins, and complex endoprosthetic reconstruction.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following the resection of benign bone tumors is a critical determinant of the ultimate functional outcome. The rehabilitation protocol must be highly individualized, taking into account the anatomical location of the lesion, the extent of the surgical resection, the type of biomechanical reconstruction performed, and the patient's baseline physiological status. A standardized, phased approach ensures the protection of the surgical construct while progressively restoring range of motion, muscular strength, and proprioception.
Phase 1: Protection and Early Healing (Weeks 0 to 6)
The primary objective of Phase 1 is to protect the surgical site, manage postoperative pain and edema, and prevent complications such as deep vein thrombosis (DVT) and joint contractures. For spinal osteoblastoma resections requiring instrumented fusion, patients are typically mobilized on postoperative day one. A rigid Thoracolumbosacral Orthosis (TLSO) or cervical collar is often prescribed to restrict extreme ranges of motion and protect the nascent fusion mass. Bending, lifting, and twisting (BLT) are strictly prohibited. For appendicular lesions like a proximal tibial CMF treated with curettage and grafting, weight-bearing status is dictated by the size of the cortical defect and the presence of prophylactic hardware. Massive defects may require strict non-weight-bearing (NWB) or toe-touch weight-bearing (TTWB) with crutches, while smaller, prophylactically plated lesions may allow for partial weight-bearing. Early, gentle passive and active-assisted range of motion (ROM) of the adjacent joints is initiated to prevent capsular adhesions.
Phase 2: Progressive Loading and Mobilization (Weeks 6 to 12)
Phase 2 commences upon clinical and radiographic evidence of early bone graft incorporation and stable spinal hardware. In the spine, patients are gradually weaned from their orthotics. Aquatic therapy is an excellent modality during this phase, providing a buoyant environment that unloads the spine while allowing
