Comprehensive Surgical Management of Benign Soft-Tissue Tumors and Tumor-Like Lesions

Key Takeaway
Benign soft-tissue tumors and tumor-like lesions encompass a diverse group of pathologies, including lipomas, peripheral nerve sheath tumors, and synovial proliferative disorders. Accurate diagnosis relies heavily on advanced MRI modalities to differentiate these from malignant sarcomas. Surgical management typically involves marginal excision or meticulous enucleation, prioritizing the preservation of adjacent neurovascular structures while minimizing recurrence risk through complete lesional resection.
Comprehensive Introduction and Patho-Epidemiology
The diagnosis and management of benign soft-tissue tumors and tumor-like lesions represent a fundamental pillar of operative orthopaedics and musculoskeletal oncology. While these lesions inherently lack metastatic potential, their local behavior can range from highly indolent and asymptomatic to locally aggressive, causing significant neurovascular compromise, joint destruction, and functional impairment. For the orthopaedic surgeon, the paramount challenge lies in accurately differentiating these benign entities from soft-tissue sarcomas prior to any surgical intervention. A meticulously planned approach—incorporating advanced magnetic resonance imaging (MRI), precise histopathological interpretation, molecular diagnostics, and anatomically sound surgical execution—is mandatory.
The epidemiology of benign soft-tissue masses dictates that they outnumber their malignant counterparts (soft-tissue sarcomas) by a staggering ratio of at least 100:1. Adipocytic tumors, specifically lipomas, are the most ubiquitous benign tumors of mesenchymal origin, predominantly affecting middle-aged adults with a slight predilection for females. However, the exact pathophysiological drivers vary drastically across the spectrum of benign lesions. For instance, classic lipomas often exhibit karyotypic abnormalities involving chromosome 12q13-15, leading to the dysregulation of the HMGA2 gene. Conversely, tenosynovial giant cell tumors (TGCT), which encompass both localized giant cell tumors of the tendon sheath (GCTTS) and diffuse pigmented villonodular synovitis (PVNS), are driven by a specific translocation t(1;2)(p13;q37). This translocation results in the overexpression of Colony-Stimulating Factor 1 (CSF1), which recruits a massive, non-neoplastic inflammatory infiltrate of macrophages that drives the clinical bulk and destructive nature of the disease.
Peripheral nerve sheath tumors (PNSTs), primarily schwannomas and neurofibromas, present another distinct pathophysiological entity. Schwannomas arise eccentrically from the Schwann cells of the nerve sheath and are typically solitary. In contrast, neurofibromas are intimately intertwined with the nerve fascicles and are frequently associated with Neurofibromatosis Type 1 (NF1), an autosomal dominant condition caused by mutations in the NF1 tumor suppressor gene on chromosome 17q11.2. The plexiform variant of neurofibroma is particularly concerning due to its pathognomonic association with NF1 and its significantly elevated risk (approximately 8-10%) of undergoing malignant transformation into a malignant peripheral nerve sheath tumor (MPNST). Understanding these deep molecular and epidemiological nuances is critical for the orthopaedic surgeon, as it directly dictates the aggressiveness of the surgical approach and the necessity for long-term surveillance.
Detailed Surgical Anatomy and Biomechanics
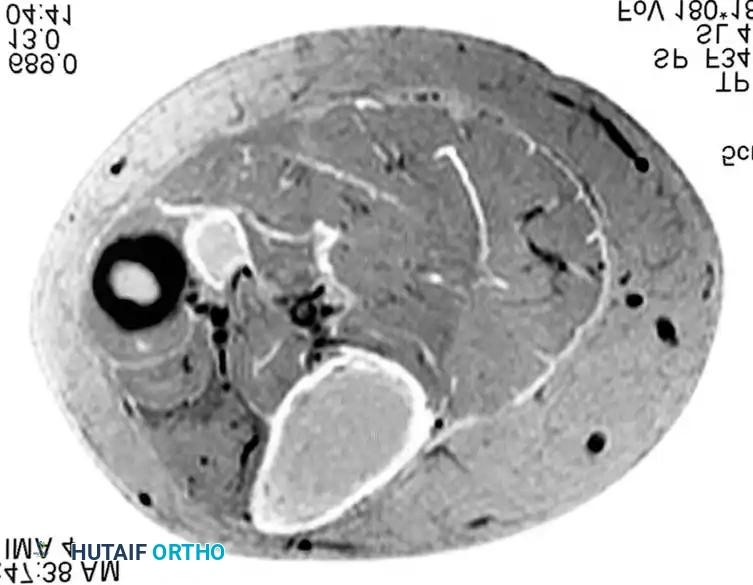
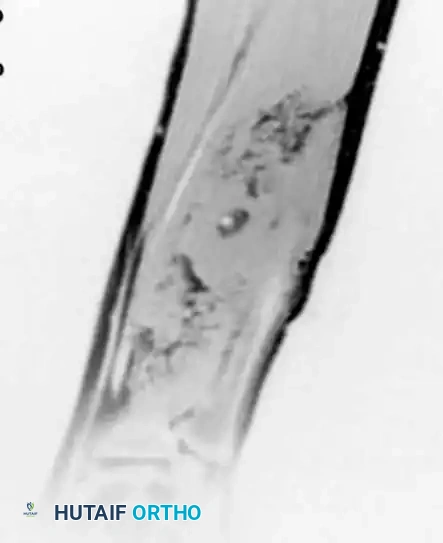
A profound understanding of compartmental anatomy, fascial boundaries, and neurovascular topography is the cornerstone of safe and effective soft-tissue tumor surgery. The musculoskeletal system is divided into distinct anatomical compartments enveloped by deep investing fascia. Benign soft-tissue tumors typically respect these fascial boundaries, expanding within the compartment rather than aggressively invading through it, a feature that distinguishes them biomechanically and radiographically from high-grade sarcomas. When planning an excision, the surgeon must conceptualize the lesion's relationship to the surrounding functional structures. For example, an intramuscular lipoma within the deep posterior compartment of the calf will alter the biomechanics of the soleus and gastrocnemius, potentially presenting with exercise-induced claudication or mimicking chronic exertional compartment syndrome due to increased intracompartmental pressures.
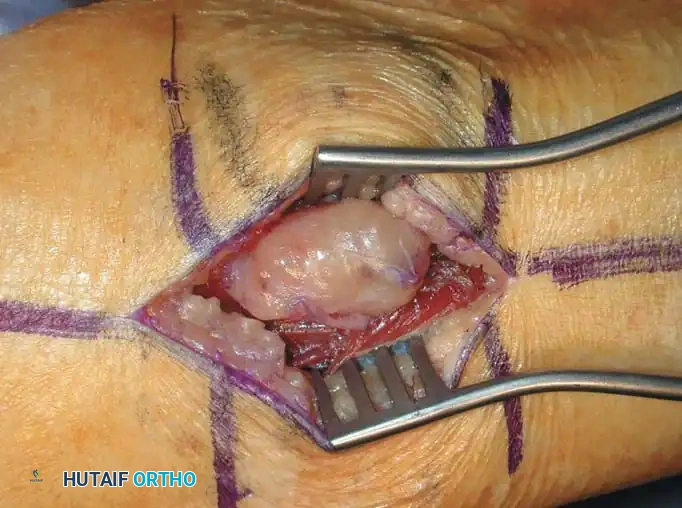
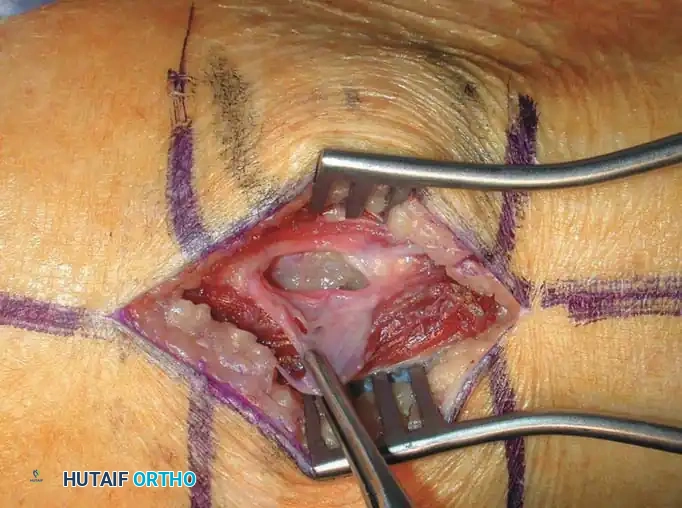
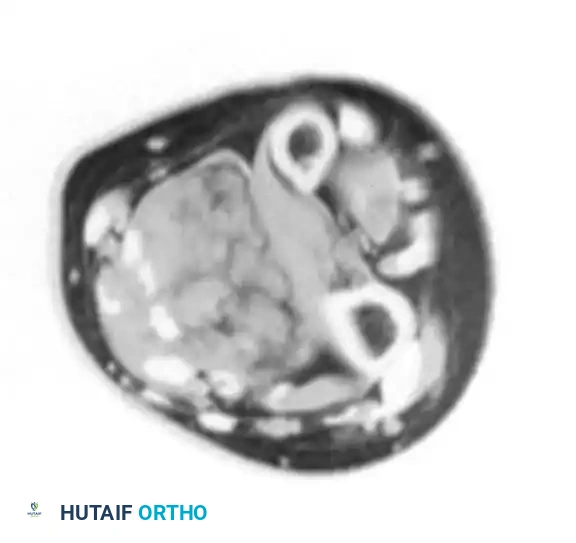
The surgical anatomy of peripheral nerves is of paramount importance when addressing PNSTs. A peripheral nerve is composed of individual axons bundled into fascicles by the perineurium; these fascicles are further bundled together and surrounded by the epineurium. Schwannomas possess a true capsule and grow eccentrically, displacing the functional nerve fascicles peripherally. The surgical plane for enucleation lies between the tumor capsule and the epineurium. In stark contrast, neurofibromas grow centrally within the endoneurium, expanding the fascicle itself. This intrinsic anatomical relationship dictates that true enucleation of a neurofibroma is frequently impossible without sacrificing the involved fascicle, fundamentally altering the surgical biomechanics and risk profile of the procedure.
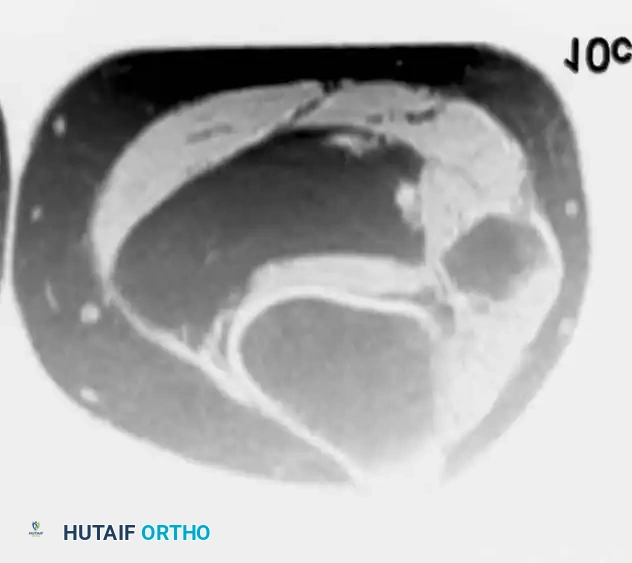
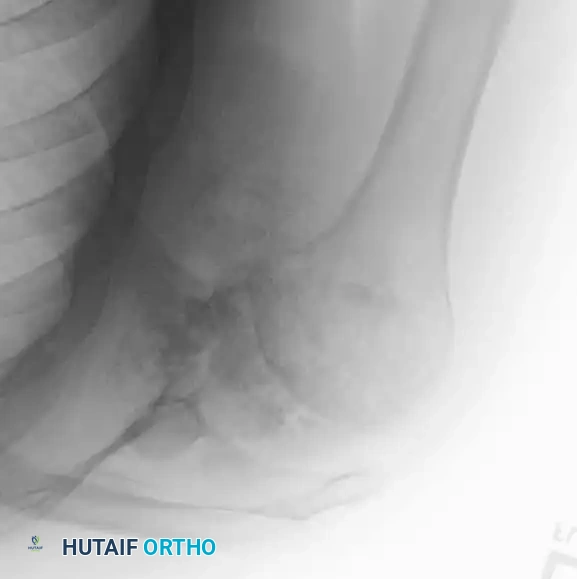
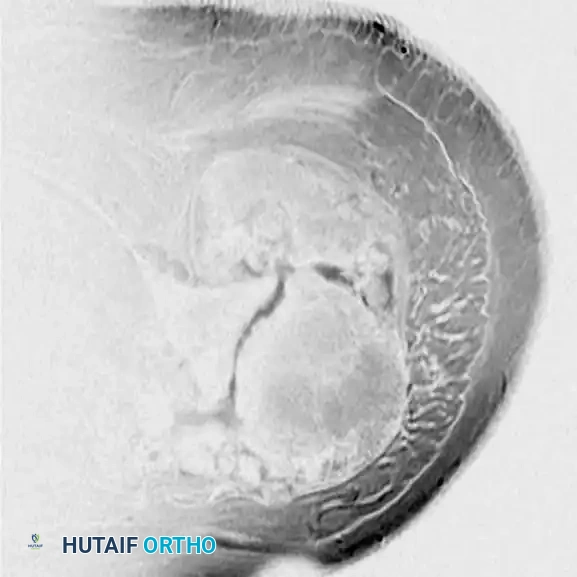
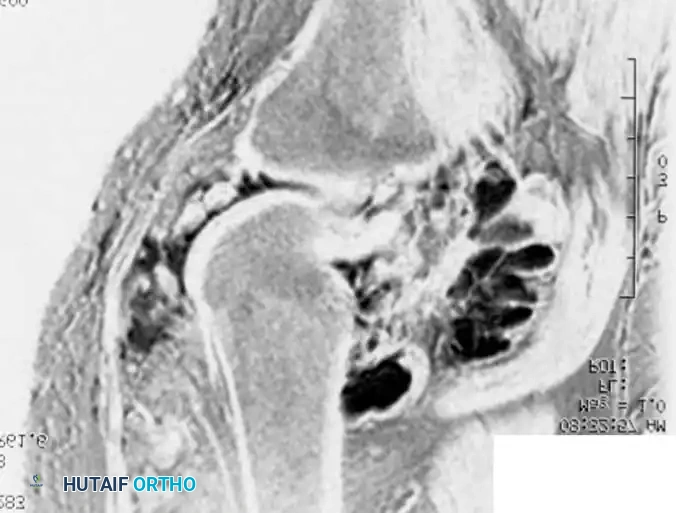
In the context of synovial proliferative lesions like PVNS and synovial chondromatosis, the surgical anatomy shifts to the intra-articular and capsular domains. The synovial lining is a highly vascularized membrane responsible for producing synovial fluid and maintaining joint homeostasis. When afflicted by diffuse PVNS, the hypertrophic, villous synovium acts as a space-occupying lesion that disrupts normal joint kinematics. The profound hemosiderin deposition and enzymatic degradation driven by the inflammatory infiltrate lead to the rapid mechanical wear of the articular cartilage. Biomechanically, the joint becomes stiff, painful, and prone to recurrent hemarthrosis. Complete eradication requires a comprehensive understanding of the joint's recesses—such as the posterior compartments of the knee or the inferior capsular recess of the shoulder—as failure to access and clear these anatomical blind spots inevitably leads to disease recurrence and accelerated secondary osteoarthritis.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for a benign soft-tissue tumor must be highly individualized, balancing the natural history of the lesion against the inherent risks of surgery. Not all benign masses require excision. The classic "leave me alone" lesions, such as asymptomatic, superficial, well-circumscribed lipomas, are often best managed with observation and patient reassurance. However, when lesions become symptomatic, exhibit rapid growth, or present diagnostic ambiguity, surgical intervention becomes mandatory.
The absolute indications for surgery include progressive neurological deficit (e.g., a schwannoma causing motor weakness or intractable radicular pain), impending joint destruction (e.g., diffuse PVNS or advanced synovial chondromatosis), and diagnostic uncertainty. The latter cannot be overstated: if an MRI reveals a deep, heterogenous mass with thick septations or nodular enhancement, the lesion must be treated as a potential sarcoma. In such cases, an incisional or core needle biopsy is the primary indication, followed by definitive surgical planning based on the histopathological diagnosis. Contraindications are generally relative and center around severe patient comorbidities, coagulopathies, or scenarios where the functional morbidity of the resection outweighs the benefit.
| Lesion Type | Primary Indications for Surgery | Relative / Absolute Contraindications |
|---|---|---|
| Lipoma / Adipocytic Tumors | Rapid growth, pain, mechanical restriction, diagnostic uncertainty (ruling out Atypical Lipomatous Tumor). | Asymptomatic, stable superficial lesions; high surgical risk patients. |
| Schwannoma | Intractable mechanically induced pain (Tinel's), progressive motor/sensory deficit. | Asymptomatic lesions discovered incidentally; lack of microsurgical expertise. |
| Neurofibroma (Plexiform) | Suspicion of malignant transformation (MPNST), severe pain, massive functional impairment. | Diffuse involvement of major nerve plexus where resection guarantees profound paralysis. |
| PVNS / TGCT (Diffuse) | Recurrent hemarthrosis, progressive joint destruction, mechanical locking. | End-stage secondary osteoarthritis (better suited for total joint arthroplasty). |
| Intramuscular Hemangioma | Severe exertional pain, failed conservative/interventional management (embolization). | Diffuse, infiltrative lesions where complete resection requires unacceptable muscle sacrifice. |
| Glomus Tumor | Exquisite point tenderness, cold hypersensitivity, nail plate deformity. | None absolute; relative contraindication if active distal phalanx infection is present. |
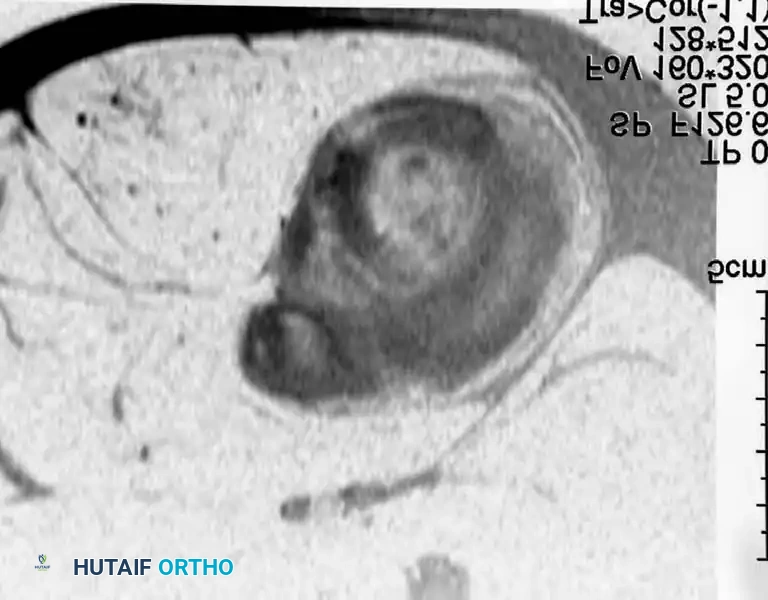
Pre-Operative Planning, Templating, and Patient Positioning
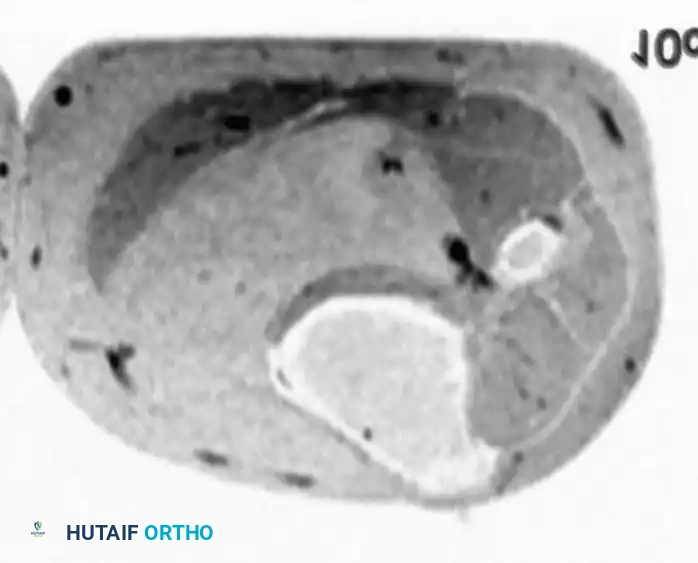
Thorough pre-operative planning is the bulwark against catastrophic intraoperative complications and the dreaded "oops procedure"—the unplanned excision of an unrecognized sarcoma. The workup must begin with a high-quality, contrast-enhanced MRI of the affected extremity. The MRI protocol should include T1-weighted, T2-weighted, and Short Tau Inversion Recovery (STIR) or fat-suppressed sequences. For adipocytic tumors, the presence of thick (>2mm) septations or non-adipose nodular components on T1 sequences necessitates a pre-operative core needle biopsy to rule out an Atypical Lipomatous Tumor (ALT) or well-differentiated liposarcoma. The biopsy tract must be meticulously planned so that it can be excised en bloc with the tumor if the lesion proves to be malignant.

Patient positioning is dictated by the anatomical location of the tumor and the necessity for extensile exposures. For extremity lesions, the patient should be positioned to allow for a full 360-degree preparation of the limb. A sterile tourniquet is mandatory for vascular lesions (hemangiomas) and highly recommended for deep intramuscular tumors to maintain a bloodless field, facilitating the identification of critical neurovascular structures. However, the tourniquet should be deflated prior to final closure to ensure meticulous hemostasis, as postoperative hematomas are a primary source of morbidity.
For peripheral nerve sheath tumors, pre-operative templating involves mapping the trajectory of the parent nerve. The surgical team must ensure the availability of operating microscopes or high-powered surgical loupes, micro-dissection instruments, and intraoperative neuromonitoring (somatosensory evoked potentials [SSEPs] and motor evoked potentials [MEPs]). Neuromonitoring provides real-time feedback during the delicate enucleation process, alerting the surgeon to impending iatrogenic nerve injury before it becomes irreversible. When addressing intra-articular lesions like PVNS, the surgeon must template for both arthroscopic and open approaches, ensuring that all necessary equipment, including aggressive synovial shavers and radiofrequency ablation wands, are immediately available.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of benign soft-tissue tumors generally relies on marginal excision, defined as removing the tumor through its pseudocapsule or reactive zone, leaving microscopically positive but macroscopically negative margins. However, the exact technique varies drastically depending on the histological entity. While soft-tissue tumor surgery does not traditionally involve rigid bony "fixation," the reconstruction and fixation of the surrounding soft-tissue envelope, tendinous insertions, and joint capsules are critical for restoring biomechanical stability post-resection.
Resection of Adipocytic Tumors and Intramuscular Lipomas
- Incision and Exposure: Utilize a longitudinal incision placed over the apex of the mass, strictly adhering to standard extensile exposure lines. Carry the dissection through the subcutaneous fat. For deep intramuscular lipomas, incise the deep investing fascia longitudinally to avoid transverse disruption of the muscle fibers.
- Dissection and Delivery: Identify the thin, fibrous pseudocapsule. Using blunt finger dissection or a Cobb elevator, sweep the normal skeletal muscle away from the tumor. Intramuscular lipomas often have a lobulated appearance that interdigitates with muscle fibers; meticulous care must be taken to follow these lobules to prevent leaving residual macroscopic disease.
- Hemostasis and Soft-Tissue Fixation: Once delivered, inspect the tumor bed. Cauterize the small perforating vessels that typically feed the base of the lipoma. To prevent massive seroma formation, the dead space must be obliterated. This is achieved via layered soft-tissue fixation, utilizing absorbable sutures to meticulously re-approximate the muscle bellies and deep fascia. A closed-suction drain is highly recommended for large dead spaces.
Enucleation of Peripheral Nerve Sheath Tumors
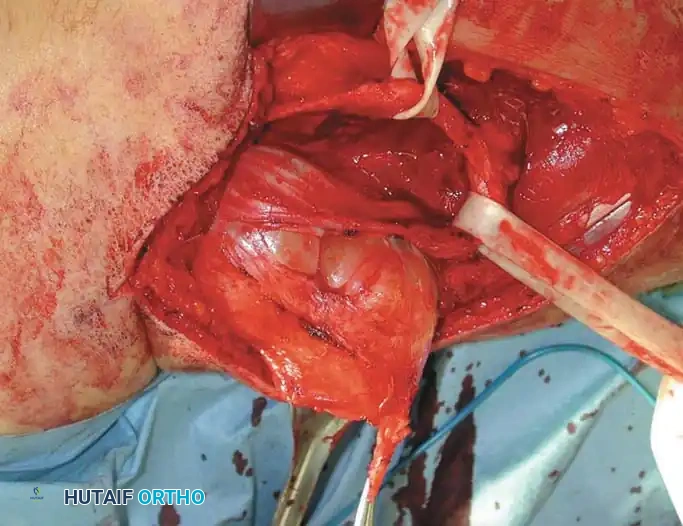
- Proximal and Distal Control: Expose the parent nerve in healthy, virgin tissue planes both proximal and distal to the tumor. Isolate the nerve using vessel loops to allow for gentle, atraumatic retraction.
- Epineurotomy: Under microscopic magnification, identify the splayed, functioning nerve fascicles draped over the tumor capsule. Utilize a micro-scalpel to make a longitudinal epineurotomy in a "safe zone" devoid of crossing fascicles.
- Micro-Enucleation: For schwannomas, establish the cleavage plane between the true tumor capsule and the surrounding fascicles. Use micro-dissectors and bipolar cautery to gently peel the fascicles away. The tumor is then "shelled out."
- Fascicular Management: If dealing with a solitary neurofibroma, the involved fascicle may need to be sacrificed. Intraoperative nerve stimulation is utilized to confirm that the fascicle is non-motor or redundant before sharp transection.

Synovectomy for Synovial Proliferative Lesions
- Arthroscopic vs. Open Approach: For localized GCTTS in the digits, a Bruner zigzag incision is utilized to expose the flexor tendon sheath, followed by meticulous marginal excision off the neurovascular bundles. For diffuse PVNS of the knee, a combined approach is often necessary.
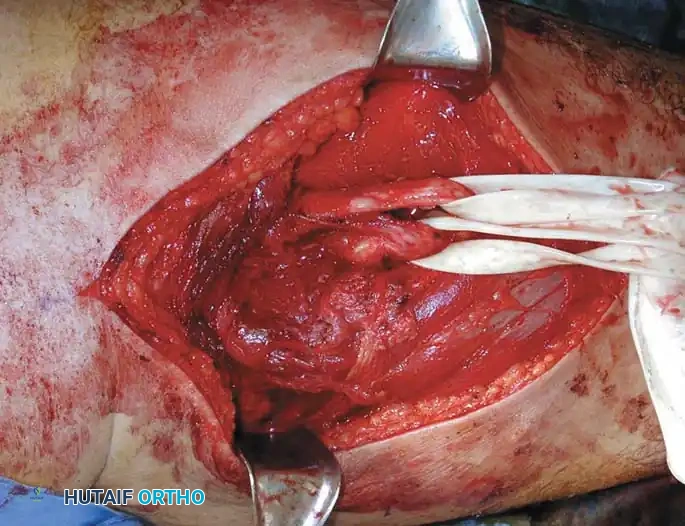
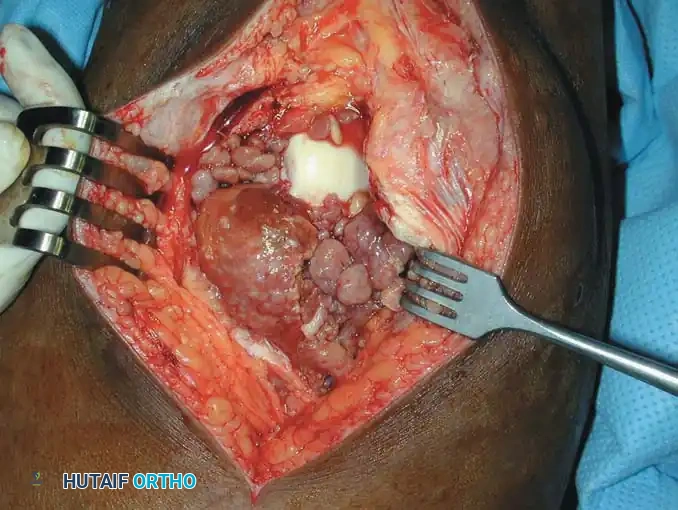
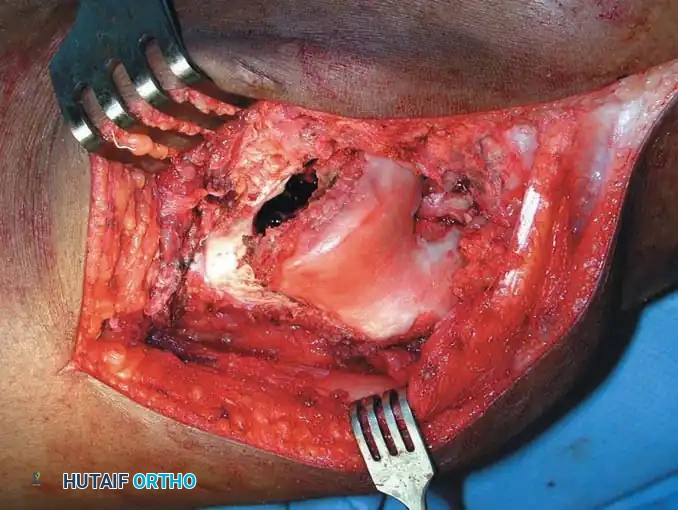
- Eradication of Disease: In the knee, perform an extensive anterior arthroscopic synovectomy utilizing aggressive shavers. For the posterior compartments, an open posteromedial or posterolateral approach is required to physically excise the thick, rust-colored, hemosiderin-laden synovium.
- Capsular Fixation and Closure: Following open synovectomy, robust capsular fixation and closure are imperative to prevent joint subluxation and massive postoperative hemarthrosis. Heavy absorbable sutures are used to repair the arthrotomy, ensuring a watertight seal.

Excision of Vascular Tumors and Glomus Malformations
- Glomus Tumor Excision: For subungual glomus tumors, perform a digital block and apply a finger tourniquet. Carefully remove or reflect the nail plate. Incise the nail bed longitudinally over the bluish discoloration.
- Tumor Delivery: The glomus tumor typically presents as a distinct, encapsulated 2-3 mm pearl. Enucleate the tumor utilizing fine tenotomy scissors.
- Nail Bed Fixation: The precise anatomical fixation of the nail bed is crucial to prevent postoperative nail deformity. Repair the nail bed utilizing 6-0 absorbable monofilament sutures, and replace the native nail plate (or a synthetic substitute) as a biologic dressing and splint.


Complications, Incidence Rates, and Salvage Management
The surgical management of benign soft-tissue tumors is generally safe, but complications can be profoundly debilitating when they occur. The most common immediate postoperative complications are hematomas and seromas, particularly following the resection of large intramuscular lipomas or highly vascular intramuscular hemangiomas. Meticulous intraoperative hemostasis, the judicious use of closed-suction drains, and compressive dressings are the primary prophylactic measures.
Nerve injury is the most feared complication during the excision of PNSTs. Transient neurapraxia is relatively common due to the traction and manipulation of the nerve fascicles during enucleation. However, permanent axonotmesis or neurotmesis resulting from iatrogenic transection of a major motor fascicle is a devastating outcome. If a major motor deficit is noted postoperatively, immediate re-exploration and microsurgical nerve repair or grafting may be indicated as a salvage procedure.
Recurrence is a significant issue for certain benign pathologies, most notably diffuse PVNS and aggressive fibromatosis (desmoid tumors, though increasingly managed medically). The recurrence rate for diffuse PVNS following open total synovectomy remains unacceptably high, approaching 40-50% in some series. Salvage management for recurrent PVNS often necessitates a multidisciplinary approach, incorporating postoperative external beam radiotherapy (EBRT) or the initiation of targeted systemic therapies, such as Pexidartinib (a CSF1R inhibitor), to control the microscopic residual disease.
| Complication | Associated Lesion / Procedure | Estimated Incidence | Salvage Management Strategy |
|---|---|---|---|
| Massive Hematoma / Seroma | Deep Intramuscular Lipoma, Hemangioma | 5 - 15% | Evacuation, layered soft-tissue fixation, prolonged closed-suction drainage, compression. |
| Iatrogenic Nerve Palsy | Schwannoma / Neurofibroma Enucleation | 2 - 5% (Permanent) | EMG at 6 weeks; if neurotmesis suspected, microsurgical nerve grafting or tendon transfers. |
| Local Recurrence | Diffuse PVNS / TGCT | 30 - 50% | Repeat radical synovectomy, Adjuvant External Beam Radiotherapy (EBRT), Pexidartinib. |
| Nail Plate Deformity | Subungual Glomus Tumor Excision | 10 - 20% | Meticulous primary nail bed repair; late reconstruction with nail bed grafting if severe. |
| Secondary Osteoarthritis | Synovial Chondromatosis, PVNS | Variable (Time-dependent) | Joint-preserving osteotomies in young patients; Total Joint Arthroplasty for end-stage disease. |

Phased Post-Operative Rehabilitation Protocols
Rehabilitation following the excision of a benign soft-tissue tumor is highly variable and must be tailored to the anatomical location of the lesion, the extent of the soft-tissue dissection, and the specific structures manipulated during surgery. A generic, one-size-fits-all approach is inadequate and can lead to either joint stiffness or the catastrophic failure of soft-tissue repairs.
Phase I: Immediate Post-Operative Protection and Wound Healing (Weeks 0-2)
The primary goal in the initial phase is the protection of the surgical site, mitigation of edema, and promotion of primary wound healing. For superficial excisions (e.g., subcutaneous lipomas), patients may bear weight as tolerated and perform gentle, active range of motion (ROM) exercises immediately. However, for deep intramuscular resections, the extremity is often placed in a bulky Jones dressing or a resting splint to minimize dead space shearing and hematoma formation. For nerve sheath tumors, the limb may be splinted in a position that relieves tension on the parent nerve. Cryotherapy and strict elevation are universally recommended.
Phase II: Restoration of Mobility and Early Strengthening (Weeks 2-6)
Once the surgical incisions have healed and sutures are removed, the focus shifts to restoring normal joint kinematics and preventing soft-tissue adhesions. For patients recovering from an extensive open synovectomy (e.g., for PVNS or synovial chondromatosis), aggressive, therapist-directed passive and active-assisted ROM is critical to prevent arthrofibrosis. Continuous Passive Motion (CPM) machines may be utilized in the immediate postoperative period for knee lesions. Strengthening begins with isometric contractions, gradually progressing to closed-kinetic-chain exercises as tolerated. If a muscle belly was significantly violated or detached during exposure, active concentric contraction of that specific muscle should be delayed until 4-6 weeks to allow for biological soft-tissue fixation and healing.
Phase III: Advanced Strengthening and Return to Function (Weeks 6-12+)
The final phase focuses on dynamic stabilization, proprioception, and the return to occupational or athletic activities. Patients undergo progressive resistance training and sport-specific functional drills. For patients who underwent enucleation of a peripheral nerve sheath tumor, neuropathic pain or hypersensitivity may persist; desensitization protocols and the judicious use of neuromodulating agents (e.g., gabapentin, pregabalin) are integrated into the rehabilitation plan. Full return to unrestricted high-impact activities is typically permitted once the patient achieves >90% contralateral limb strength and demonstrates pain-free, full ROM.
Summary of Landmark Literature and Clinical Guidelines
The evidence-based management of benign soft-tissue tumors is guided by decades of meticulous clinical observation, advancements in molecular pathology, and evolving surgical paradigms. The World Health Organization (WHO) Classification of Tumours of Soft Tissue and Bone remains the definitive, internationally recognized framework for the histological and molecular categorization of these lesions. The integration of molecular diagnostics into the WHO guidelines has revolutionized the field, particularly the use of MDM2 and CDK4 amplification assays to definitively differentiate large, deep-seated benign lipomas from well-differentiated liposarcomas (Atypical Lipomatous Tumors).
Landmark literature regarding the surgical approach to soft-tissue masses is heavily influenced by the principles established by Enneking and the Musculoskeletal Tumor Society (MSTS). Enneking's concepts of surgical margins
