Benign Hand Tumors: Comprehensive Surgical Management Guide

Key Takeaway
Benign tumors of the hand, including lipomas, giant cell tumors of the tendon sheath, and glomus tumors, require meticulous surgical management to preserve neurovascular function and minimize recurrence. This comprehensive guide details the pathophysiology, clinical presentation, and step-by-step surgical techniques for excising these lesions. Emphasizing precise dissection, appropriate imaging, and evidence-based postoperative protocols, it serves as an essential resource for orthopedic surgeons and hand specialists.
Comprehensive Introduction and Patho-Epidemiology
Benign tumors of the hand encompass a diverse, heterogeneous group of neoplasms arising from adipose, synovial, fibrous, neural, vascular, and osseous tissues. Although these lesions intrinsically lack malignant potential and rarely pose a threat to the patient's life, they frequently cause significant morbidity. This is primarily due to the complex, unyielding, and densely packed neurovascular anatomy of the hand and wrist. A mass effect that might be entirely asymptomatic in the thigh or abdomen can rapidly precipitate severe compressive neuropathies, mechanical restriction of tendon excursion, and devastating functional impairment when located within the rigid confines of the carpal tunnel, Guyon's canal, or the deep palmar spaces. Surgical management of these lesions therefore requires a profound, three-dimensional understanding of hand biomechanics, meticulous microsurgical technique, and strict adherence to oncologic principles to minimize recurrence while preserving maximal function.
Epidemiologically, the true incidence of benign hand tumors is difficult to ascertain, as many asymptomatic lesions remain unreported. However, clinical registries indicate that ganglion cysts (though technically reactive rather than true neoplasms) are the most frequently encountered masses, followed closely by giant cell tumors of the tendon sheath (GCTTS), which are the most common solid cellular tumors. Adipose tissue tumors, particularly lipomas, are also remarkably prevalent. Neural tumors such as schwannomas and neurofibromas, along with vascular anomalies like hemangiomas and glomus tumors, constitute the remainder of the frequently excised lesions. The demographic distribution varies significantly by histology; for instance, GCTTS exhibits a strong predilection for females in their fourth to sixth decades, whereas lipoblastomas are almost exclusively diagnosed in pediatric populations under the age of seven.
The pathogenesis of these benign neoplasms is increasingly understood at a molecular and cytogenetic level, shifting the paradigm from purely descriptive pathology to targeted molecular diagnostics. For example, GCTTS is now recognized to frequently harbor a t(1;2)(p13;q37) translocation, leading to the overexpression of colony-stimulating factor 1 (CSF1), which recruits a massive influx of non-neoplastic multinucleated giant cells and macrophages. Similarly, many benign lipomatous tumors exhibit aberrations in the 12q13-15 region involving the HMGA2 gene. Understanding these genetic underpinnings is not merely an academic exercise; it is becoming crucial in differentiating aggressive benign lesions from low-grade sarcomas, guiding both the extent of surgical resection and the potential for adjuvant systemic therapies in recurrent or diffuse disease.
Always approach a "simple" hand mass with a high index of suspicion. The clinical presentation of a benign lesion can mimic that of a soft tissue sarcoma, such as an epithelioid sarcoma or synovial sarcoma, both of which have a propensity to arise in the distal extremities of young adults. Inadequate preoperative imaging or an unplanned marginal excision (a "whoops" procedure) of an unrecognized aggressive malignant lesion can lead to catastrophic functional loss, the necessity for proximal amputation, or complex, anatomically destructive recurrences. Therefore, every hand mass must be treated with a standardized diagnostic algorithm, prioritizing definitive histopathological and radiological characterization prior to any definitive surgical intervention.

Detailed Surgical Anatomy and Biomechanics
The surgical anatomy of the hand is characterized by a series of specialized, interconnected, yet distinct fascial compartments that dictate the growth patterns and clinical presentation of benign tumors. The palmar aponeurosis, a robust triangular condensation of deep fascia, acts as an unyielding barrier to the volar expansion of deep-seated tumors. Consequently, neoplasms originating within the deep palmar space, midpalmar space, or thenar space tend to migrate along the paths of least resistance. These paths frequently follow the lumbrical canals, leading to tumor presentation at the web spaces or the periphery of the hand. This anatomical diversion means that the palpable mass is often only the "tip of the iceberg," with the bulk of the tumor sequestered deep within the intrinsic musculature, necessitating extensile surgical exposures.
The proximity of these tumors to critical neurovascular structures fundamentally alters their biomechanical impact and surgical management. The digital nerves and arteries, traversing the digits in a volar-lateral position, are intimately associated with the flexor tendon sheaths and Cleland's and Grayson's ligaments. Tumors such as giant cell tumors of the tendon sheath frequently originate from the synovial lining of these sheaths and aggressively wind around the digital nerves and vessels. As the tumor expands, it can displace the neurovascular bundle superficially or encase it entirely, increasing the risk of iatrogenic injury during excision. Furthermore, mass effect within confined spaces like the carpal tunnel directly compresses the median nerve against the transverse carpal ligament, leading to ischemic neuropraxia, demyelination, and the classic symptoms of carpal tunnel syndrome.

Biomechanically, the hand relies on an intricate balance of tendon excursion within a highly specialized retinacular pulley system. Benign tumors located adjacent to the metacarpophalangeal (MCP) or proximal interphalangeal (PIP) joints can act as mechanical blocks, severely restricting active and passive range of motion. A mass situated deep to the flexor tendons can displace them volarly, altering their moment arm and potentially causing a bowstringing effect if the overlying pulleys are compromised by the tumor or its subsequent surgical excision. The preservation of the A2 and A4 pulleys during tumor resection is paramount; failure to do so results in a significant loss of mechanical advantage, manifested as an active flexion lag and diminished grip strength.
Intraneural anatomy is particularly relevant when discussing lesions such as intraneural lipofibromas or schwannomas. The peripheral nerve is composed of individual fascicles enveloped by perineurium, which are bundled together and surrounded by the epineurium. Tumors that arise eccentrically from the epineurium (like schwannomas) can often be carefully enucleated by splitting the epineurium and dissecting parallel to the intact fascicles. Conversely, infiltrative lesions like intraneural lipofibromas interdigitate between and within the fascicles themselves. Attempting to dissect such fibroadipose tissue from the fascicles invariably disrupts the delicate vasa nervorum, leading to severe intraneural fibrosis, irreversible ischemia, and a devastating increase in neural deficit. Understanding this microanatomy dictates a strictly conservative surgical approach for infiltrative neural lesions.

Exhaustive Indications and Contraindications
The decision to proceed with surgical excision of a benign hand tumor requires a nuanced risk-benefit analysis, balancing the natural history of the specific neoplasm against the inherent risks of hand surgery. Observation with serial clinical examinations is often appropriate for small, asymptomatic, slow-growing lesions that do not interfere with hand mechanics or cause neurovascular compromise. However, proactive surgical intervention becomes mandatory when tumors begin to threaten the functional integrity of the hand. The primary goal of surgery is not merely the extirpation of the mass, but the preservation and restoration of optimal hand biomechanics and sensibility.
Absolute indications for surgical intervention include definitive evidence of neurovascular compromise. This manifests as progressive sensory deficits, intrinsic muscle wasting (such as thenar atrophy in the setting of a median nerve compressive lesion), or vascular insufficiency due to arterial compression. Additionally, any mass that mechanically blocks joint motion, prevents full tendon excursion, or causes significant lateral deviation of the digits necessitates excision. A critical absolute indication is a rapid increase in the size of the mass, changes in overlying skin characteristics, or the development of severe rest pain, all of which raise the specter of malignant transformation or an unrecognized soft tissue sarcoma, mandating immediate biopsy or wide excision.
Relative indications revolve around patient-reported symptoms that degrade quality of life but do not immediately threaten limb function. These include moderate, activity-related pain, localized tenderness, and significant cosmetic deformity that causes psychological distress to the patient. Recurrent tumors, such as a relapsing giant cell tumor of the tendon sheath, also represent a relative indication for re-excision, though the surgeon must counsel the patient that revision surgery carries a substantially higher risk of neurovascular injury and postoperative stiffness due to altered anatomical planes and dense scar tissue.
Contraindications to surgical excision are relatively few but critical to recognize. Absolute contraindications include severe systemic medical comorbidities that preclude the safe administration of regional or general anesthesia. Relative contraindications exist in the context of diffuse, highly infiltrative lesions (such as diffuse lipomatosis or certain extensive vascular malformations) where complete surgical extirpation is anatomically impossible without sacrificing critical motor or sensory nerves. In such cases, aggressive debulking may lead to profound morbidity that outweighs the benefits of tumor volume reduction, and alternative modalities or strictly conservative, symptom-targeted management should be employed.
| Indication Category | Specific Clinical Scenarios | Rationale for Intervention / Non-Intervention |
|---|---|---|
| Absolute Indications | Progressive neurovascular deficit (e.g., carpal tunnel syndrome from deep lipoma). | Prevent irreversible axonal loss and intrinsic muscle denervation. |
| Absolute Indications | Mechanical block to digital flexion/extension or joint deviation. | Restore normal tendon excursion and joint kinematics; prevent contractures. |
| Absolute Indications | Rapid growth, severe pain, or suspected malignancy. | Obtain definitive histopathology; achieve oncologic clearance if malignant. |
| Relative Indications | Cosmetically unacceptable deformity causing psychological distress. | Improve patient quality of life and psychosocial well-being. |
| Relative Indications | Mild to moderate activity-related discomfort. | Alleviate localized mass effect without risking major structural damage. |
| Absolute Contraindications | Medically unstable patient (e.g., recent myocardial infarction). | Avoid life-threatening perioperative cardiopulmonary complications. |
| Relative Contraindications | Diffuse, un-resectable infiltrative lesions (e.g., extensive macrodactyly lipofibroma). | Radical excision would result in a functionless, insensate digit. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful hand tumor surgery. The clinical evaluation must be exhaustive, beginning with a detailed history documenting the timeline of mass appearance, rate of growth, and associated symptoms such as pain, paresthesias, or weakness. Physical examination requires precise documentation of the mass's location, size, consistency, mobility, and adherence to overlying skin or underlying deep structures. Provocative maneuvers, including Tinel's sign over adjacent peripheral nerves, the Allen test to assess dual arterial inflow, and transillumination (to differentiate solid tumors from cystic lesions like ganglions), are mandatory. The surgeon must meticulously map sensory distributions using two-point discrimination and assess the strength of intrinsic and extrinsic musculature.
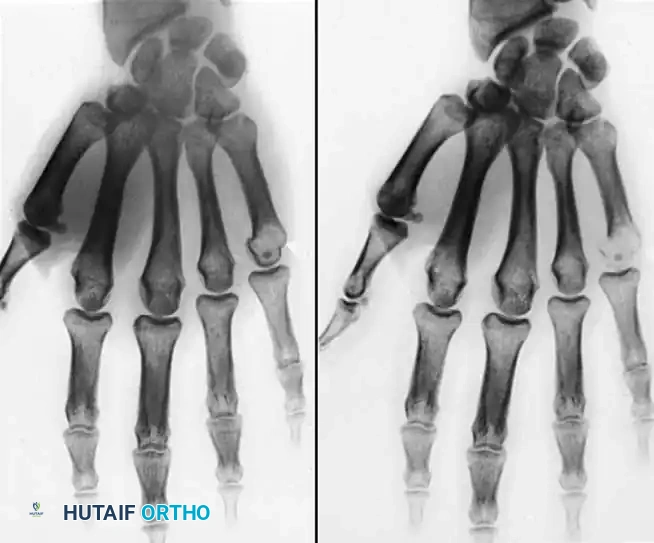
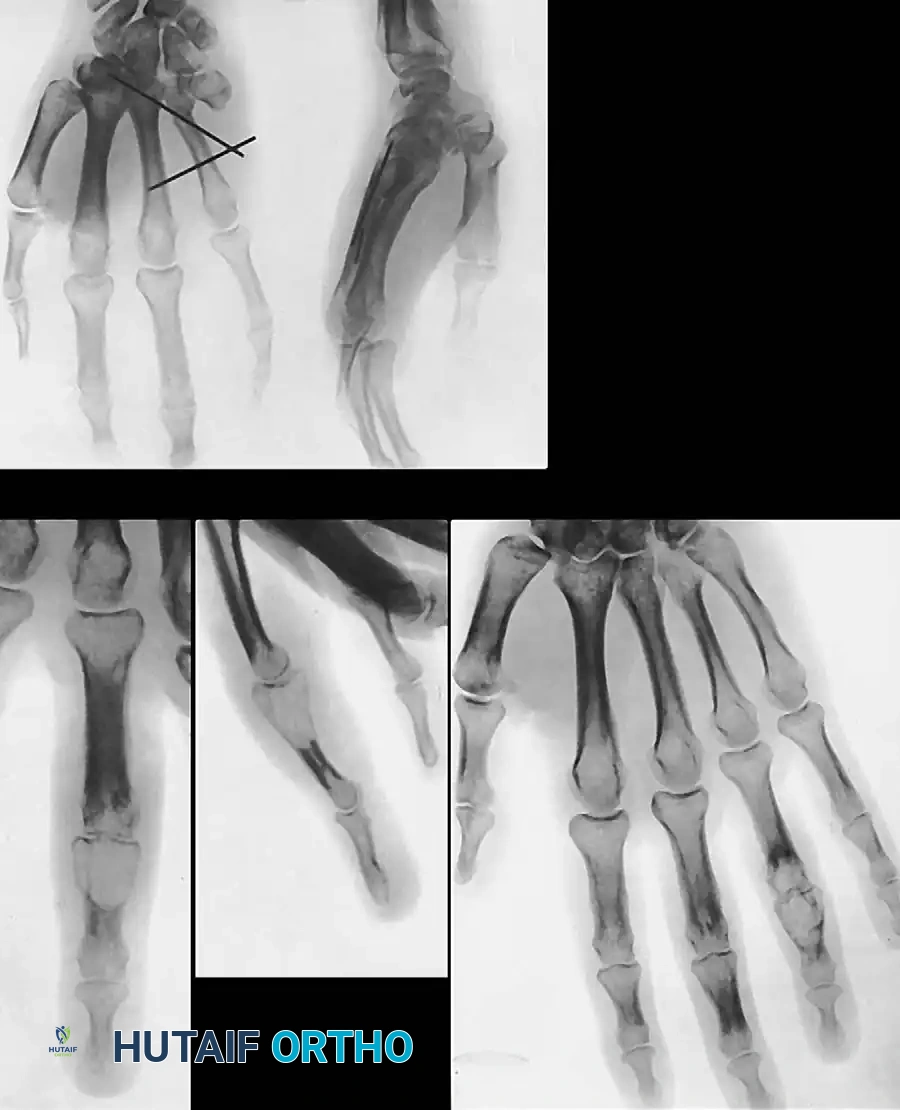
Radiographic imaging is indispensable. Plain radiographs (posteroanterior, lateral, and oblique views) are the initial modality of choice to evaluate for osseous involvement, periosteal reaction, or intralesional calcifications (often seen in vascular malformations with phleboliths or synovial chondromatosis). Ultrasound is a highly cost-effective, dynamic tool for differentiating solid from cystic masses and assessing the vascularity of the lesion using Doppler flow. However, Magnetic Resonance Imaging (MRI) with and without intravenous gadolinium contrast remains the gold standard for solid hand tumors. MRI provides unparalleled soft-tissue contrast, delineating the exact anatomical extent of the tumor, its relationship to neurovascular bundles, and its tissue characteristics (e.g., the high T1 signal of a lipoma versus the low T1/T2 signal with blooming artifact typical of a hemosiderin-laden GCTTS).

When the diagnosis remains equivocal after advanced imaging, or if there is any suspicion of malignancy, a preoperative biopsy is required. The biopsy must be planned with the definitive excision in mind. Longitudinal incisions should be strictly utilized, ensuring that the biopsy tract can be entirely excised en bloc with the tumor during the definitive procedure. Transverse incisions or poorly placed biopsy tracts can contaminate previously uninvolved anatomical compartments, potentially converting a limb-sparing procedure into an amputation if the lesion proves to be a sarcoma. For small, superficial lesions that are highly likely to be benign based on MRI, an excisional biopsy (marginal excision) may be performed as the primary diagnostic and therapeutic maneuver.
Patient positioning and operating room setup are critical for optimizing the surgical field. The patient is placed in the supine position with the affected upper extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. After meticulous exsanguination of the limb using an Esmarch bandage, the tourniquet is inflated to 250 mm Hg (or 100 mm Hg above the patient's systolic blood pressure) to ensure an absolutely bloodless field, which is non-negotiable for identifying microscopic satellite lesions and delicate neurovascular structures. The use of loupe magnification (minimum 3.5x) or an operating microscope is strongly recommended, particularly when dissecting tumors intimately associated with digital nerves or performing nerve grafting procedures.

Step-by-Step Surgical Approach and Fixation Technique
The surgical extirpation of benign hand tumors demands a highly methodical approach, prioritizing extensile exposures and the atraumatic handling of soft tissues. Incisions must be carefully designed to allow for proximal and distal extension if the tumor is larger than anticipated. Brunner zigzag incisions or mid-axial incisions are preferred for the digits, while extensile palmar incisions incorporating the existing flexion creases are utilized for the hand. Under no circumstances should an incision cross a flexion crease at a right angle, as this invariably leads to hypertrophic scarring and debilitating flexion contractures. Once the skin and subcutaneous tissues are incised, the surgeon must elevate thick skin flaps, preserving the subdermal vascular plexus to prevent tip necrosis or delayed wound healing.
Excision of Adipose Tissue Tumors
Lipomas, although composed of mature adipose tissue, present unique surgical challenges in the hand. For deep palmar lipomas, careful blunt and sharp dissection is mandatory. These tumors frequently sequester digital nerves and are invariably larger than clinically apparent, extending deep to the palmar aponeurosis. The surgeon must perform a marginal excision, meticulously dissecting along the delicate, flimsy capsule of the lipoma. It is imperative that this capsule is not breached; rupturing the capsule leads to the spillage of fatty lobules, which are easily lost in the surrounding normal adipose tissue, significantly increasing the risk of recurrence.

Fig. 1: Large palmar lipoma causing significant mechanical interference with grasp and digital flexion.

Fig. 2: Intraoperative view demonstrating extensive lobulation of the lipoma winding around digital nerves and flexor tendons.
Infiltrating lipomas and lipoblastomas require a more aggressive approach due to their lack of encapsulation and high recurrence rates. For infiltrating lipomas, a wide excision is recommended, balancing oncologic clearance with the preservation of essential motor function. The surgeon must trace the tumor as it interdigitates between individual muscle fibers, often requiring the sacrifice of small, non-critical muscle fascicles to achieve clear margins. For lipoblastomas in pediatric patients, the absence of cellular atypia and mitosis must be confirmed intraoperatively or preoperatively to rule out congenital liposarcoma. Complete marginal excision is the treatment of choice, with a reported recurrence rate of 14%.
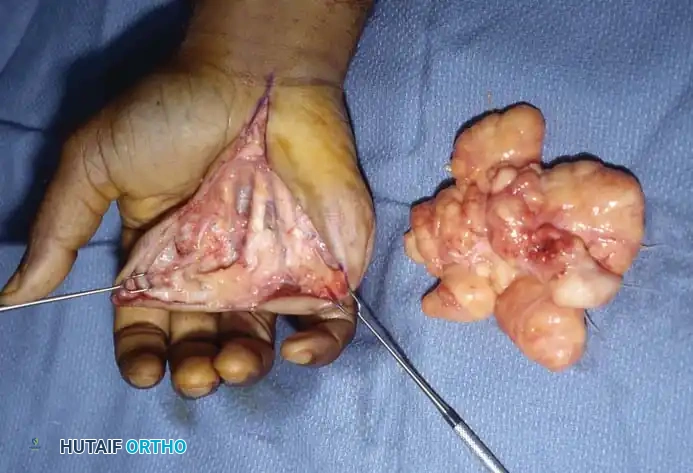
Fig. 3: Complete excision of the lipoma with surgical sparing of the flexor tendons and digital nerves.
Management of Intraneural Lipofibromas
Intraneural lipofibromas, predominantly affecting the median nerve, demand a strictly conservative surgical philosophy. The microscopic infiltration of fibroadipose tissue into the epineurium, separating and compressing individual nerve fascicles, makes complete excision impossible without causing catastrophic neurological deficits. The gold standard of treatment is surgical decompression. This involves a generous carpal tunnel release, extending proximally into the distal forearm fascia to thoroughly decompress the median nerve.

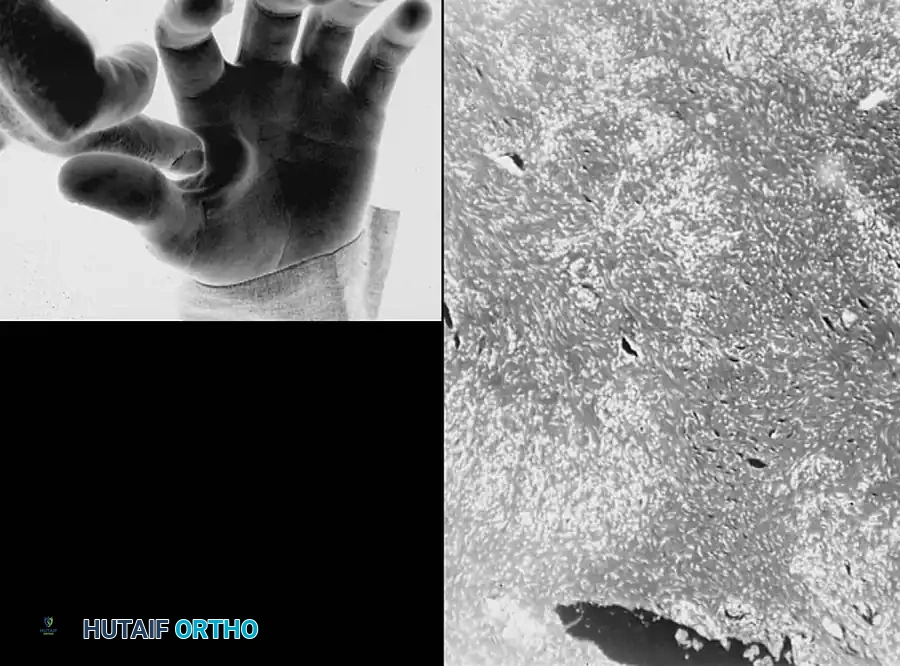
Fig. 4: Intraneural lipofibroma of the median nerve presenting with mild thumb enlargement and volar wrist pain.

Fig. 5: Surgical exposure revealing lipofibromatous tissue interspersed within and around the median nerve fascicles.
Intraneural excision or aggressive debulking of the median nerve is strictly contraindicated. Attempting to dissect the fibroadipose tissue from the fascicles invariably leads to severe intraneural fibrosis, ischemia, and a devastating increase in neural deficit. Following decompression, the nerve will remain enlarged and tortuous, but the extrinsic pressure is relieved, often halting the progression of symptoms.
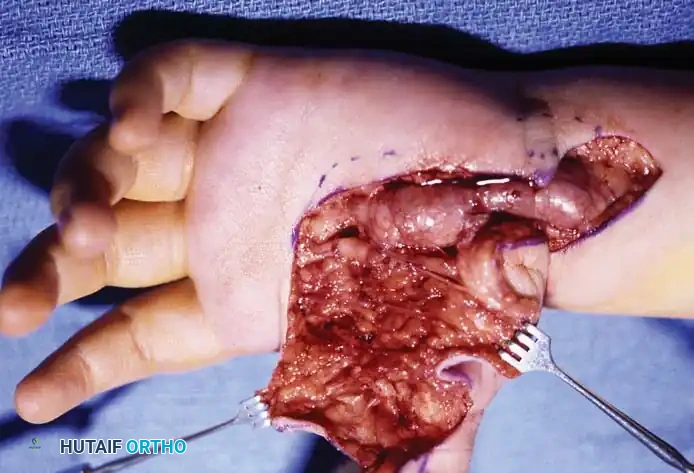
Fig. 6: Following conservative debulking and carpal tunnel release, the median nerve fascicles remain enlarged and tortuous, highlighting the infiltrative nature of the disease.
In highly selected cases where a non-critical digital nerve is exclusively involved and causing severe, localized symptoms, an en bloc excision of the affected nerve segment may be performed. This must be immediately followed by primary nerve reconstruction using an interpositional nerve graft (e.g., sural nerve or medial antebrachial cutaneous nerve). The nerve graft is meticulously sutured in place using 8-0 or 9-0 epineurial sutures under microscopic magnification. The patient must be extensively counseled preoperatively regarding the permanent sensory alteration and the lengthy recovery associated with nerve grafting.
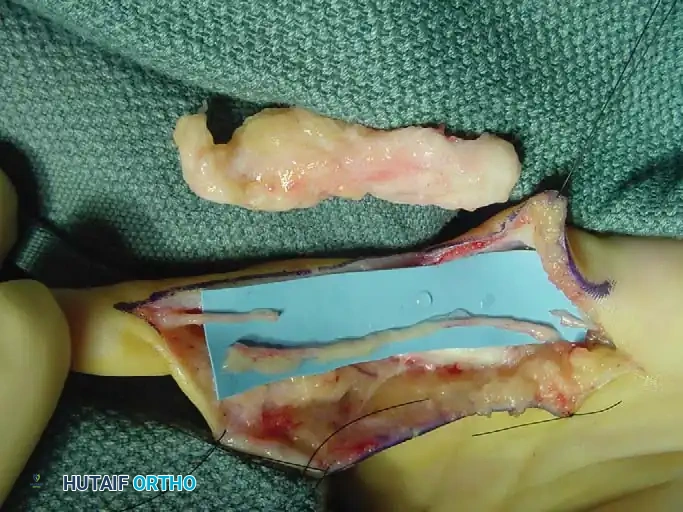
Fig. 7: Recurrent intraneural lipofibroma of the ulnar digital nerve to the small finger.
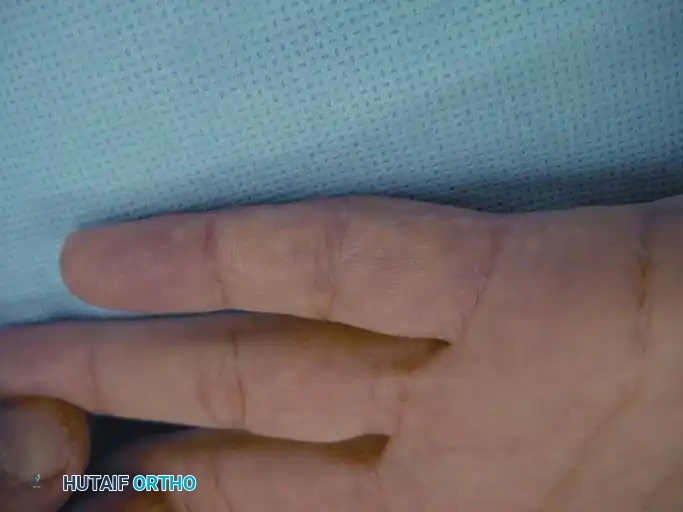
Fig. 8: Surgical exposure demonstrating a 4-cm segment of involved ulnar digital nerve with normal-appearing proximal and distal segments.

Fig. 9: En bloc excision of the digital nerve and tumor, with an interpositional nerve graft placed in proximity.
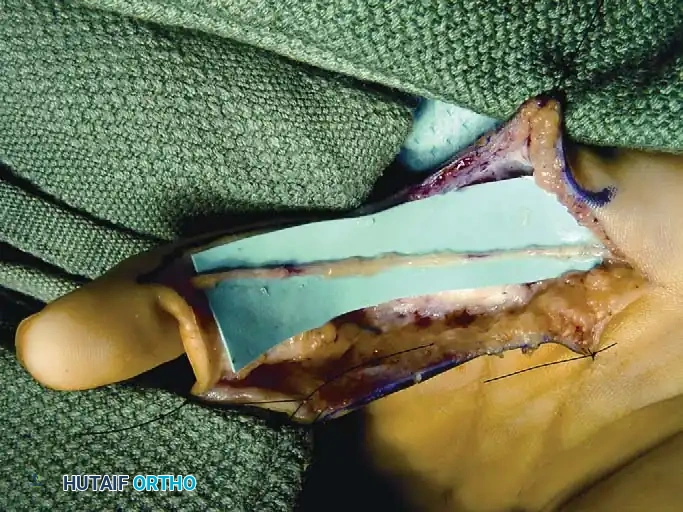
Fig. 10: Nerve graft meticulously sutured in place using 8-0 or 9-0 epineurial sutures under microscopic magnification.
Excision of Giant Cell Tumor of the Tendon Sheath
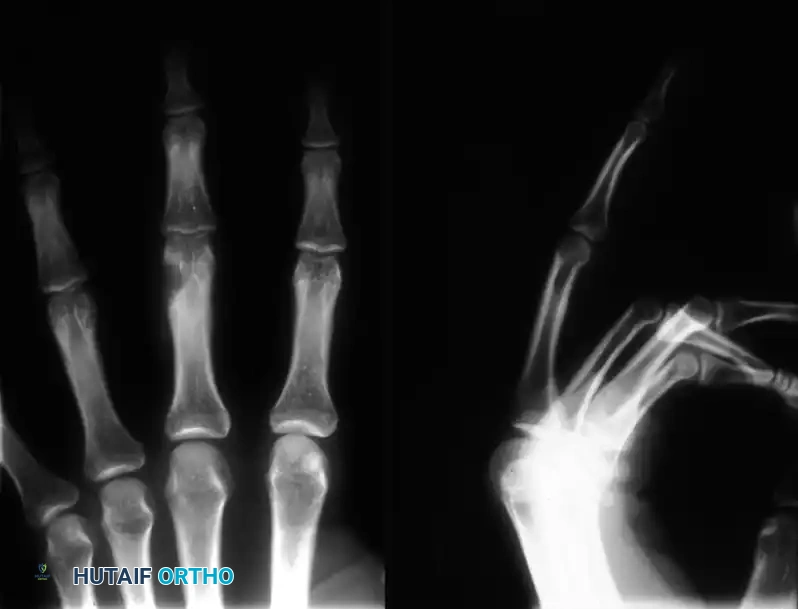
The excision of a Giant Cell Tumor of the Tendon Sheath (GCTTS) is notoriously difficult and fraught with high recurrence rates. These tumors, presenting as lobulated, yellowish-brown masses, frequently wind in and around the flexor tendons, infiltrate their synovial sheaths, and encircle the digital nerves and arteries. The surgical approach requires a wide exposure to visualize the entire extent of the tumor.

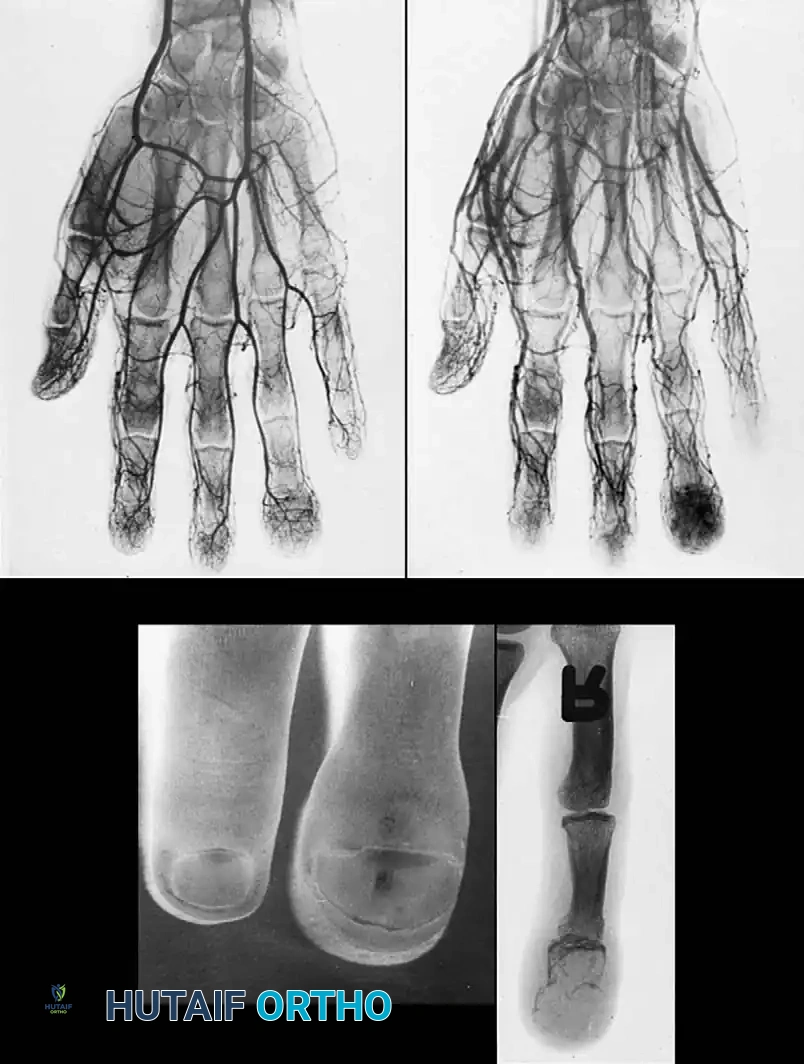
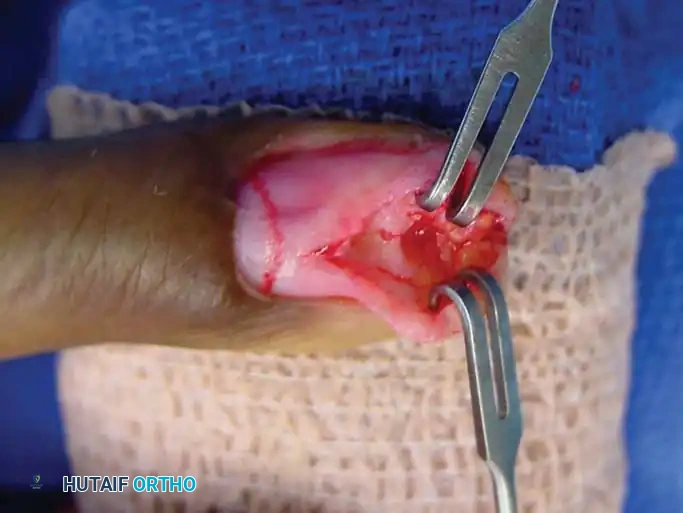
Fig. 11: Giant cell tumor of the tendon sheath demonstrating nearly circumferential involvement of the index finger tip.
Fig. 12: Surgical dissection showing a well-encapsulated giant cell tumor with its pathognomonic yellowish-brown color.
The surgeon must meticulously dissect the tumor off the neurovascular bundles using micro-scissors and magnification. GCTTS often exhibits satellite nodules—small, disconnected fragments of tumor tissue hidden within the tendon sheath or joint capsule. Failure to identify and excise these satellite lesions is the primary cause of recurrence. The involved segment of the flexor tendon sheath must be excised, taking care to preserve the critical A2 and A4 pulleys to prevent tendon bowstringing. If the tumor has invaded the underlying joint capsule or bone (causing pressure erosions visible on radiographs), a thorough curettage of the bone and excision of the involved capsule is mandatory.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the excision of benign hand tumors carries a distinct set of complications, ranging from minor wound healing issues to catastrophic neurovascular loss. The most prevalent complication across all benign tumor types is local recurrence. The incidence of recurrence varies drastically depending on the histology and the adequacy of the initial excision. For well-encapsulated lipomas, recurrence is exceptionally rare (<2%). However, for GCTTS, recurrence rates historically range from 10% to 45%, largely due to unrecognized satellite nodules or inadequate excision of the involved synovial sheath. Infiltrating lipomas carry a formidable recurrence rate of up to 60% due to their nonencapsulated, intermuscular growth pattern.
Iatrogenic neurovascular injury is the most devastating intraoperative complication. The intimate association of tumors with digital nerves and arteries makes them highly susceptible to transection, crush injury, or thermal damage from electrocautery. The incidence of digital nerve injury during GCTTS excision is estimated at 2-5%. If a nerve is inadvertently transected, immediate primary microsurgical repair using 8-0 or 9-0 nylon epineurial sutures must be performed. If a segment of the nerve is lost, an interpositional nerve graft or a nerve conduit (for gaps <1.5 cm) is required. Arterial injury, while less common, can lead to digital ischemia, particularly if the contralateral digital artery is absent or compromised. Immediate microvascular repair or vein grafting is necessary to salvage the digit.
Postoperative stiffness and tendon adhesions are common, particularly following the excision of tumors intimately associated with the flexor apparatus, such as GCTTS or deep palmar lipomas. The surgical trauma and subsequent hematoma formation promote dense scar tissue that tethers the flexor tendons to the surrounding structures, limiting active excursion. The incidence of clinically significant stiffness can exceed 20% in complex cases. Salvage management requires aggressive, formalized hand therapy. If therapy fails after 4-6 months, a secondary surgical tenolysis may be indicated, though this carries its own risks of re-adhesion and tendon rupture.
Complex Regional Pain Syndrome (CRPS) is a severe, debilitating complication characterized by disproportionate pain, autonomic dysfunction, and trophic changes. Its exact incidence following hand tumor excision is unknown but is generally considered to be between 1-3%. Prevention through meticulous, atraumatic surgical technique and adequate postoperative pain control is paramount. Once diagnosed, salvage management requires a multidisciplinary approach, including aggressive hand therapy, neuropathic pain modulators (e.g., gabapentin, amitriptyline), and potentially stellate ganglion blocks for refractory cases.
| Complication | Estimated Incidence | Salvage Management / Prevention Strategies |
|---|---|---|
| Local Tumor Recurrence | GCTTS: 10-45% Infiltrating Lipoma: 60% Lipoma: <2% |
Salvage: Wide re-excision, consider adjuvant radiotherapy for aggressive recurrent GCTTS. Prevention: Use operating microscope to identify satellite nodules; avoid capsular breach. |
| Digital Nerve Injury | 2-5% (higher in revisions) | Salvage: Immediate primary |
Clinical & Radiographic Imaging Archive