Operative Management of Benign and Locally Aggressive Bone Tumors
Key Takeaway
This comprehensive surgical guide details the operative management of benign and locally aggressive bone tumors, including giant cell tumors, chondroblastomas, chondromyxoid fibromas, and osteoblastomas. It provides orthopedic surgeons with evidence-based protocols for intralesional curettage, adjuvant treatments, and defect reconstruction. Emphasizing precise surgical technique and biomechanical principles, this text serves as an essential resource for minimizing local recurrence and optimizing functional outcomes in orthopedic oncology.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of benign but locally aggressive bone tumors requires a delicate balance between complete oncologic eradication and the preservation of biomechanical function and joint kinematics. The raw literature extensively documents the evolution of treatment for Giant Cell Tumor of Bone (GCTB), Chondroblastoma, Chondromyxoid Fibroma (CMF), and Osteoblastoma. While histologically benign, these lesions exhibit a propensity for aggressive local destruction, cortical breach, and, in rare instances, benign pulmonary metastasis. These neoplasms correspond to Enneking Stage 3 (aggressive) benign bone tumors, characterized by their rapid growth, penetration of the cortical bone, and extension into the surrounding soft tissue envelope, necessitating a rigorous, oncologically sound surgical approach.
The epidemiology of these lesions reveals distinct demographic and skeletal predilections that are critical for differential diagnosis. Giant Cell Tumor of Bone predominantly affects skeletally mature individuals in their third to fifth decades of life, with a slight female predilection. It is classically located in the meta-epiphyseal region of long bones, with over 50% occurring around the knee (distal femur and proximal tibia), followed by the distal radius and sacrum. Conversely, Chondroblastoma is almost exclusively a tumor of the skeletally immature, arising in the epiphyses or apophyses of long bones (proximal humerus, distal femur, proximal tibia) in patients typically between 10 and 20 years of age. Chondromyxoid Fibroma, one of the rarest benign bone tumors (comprising less than 1% of all primary bone tumors), typically presents as an eccentric, metaphyseal lesion in the lower extremities of young adults. Osteoblastoma, accounting for approximately 1% of all primary bone tumors, has a strong predilection for the posterior elements of the spine and the metadiaphysis of long bones, predominantly affecting males in their second and third decades.
Recent advancements in molecular pathology have revolutionized our understanding of the patho-epidemiology of these tumors, providing novel diagnostic markers and therapeutic targets. GCTB is now known to be driven by specific mutations in the H3F3A gene (predominantly the G34W mutation), which is found in the neoplastic mononuclear stromal cells, while the multinucleated giant cells are reactive osteoclasts recruited via the RANK/RANKL pathway. Similarly, Chondroblastoma is characterized by a distinct mutation in the H3F3B gene (K36M mutation). Osteoblastoma frequently exhibits rearrangements of the FOS or FOSB genes, driving excessive woven bone formation. Understanding these molecular drivers is not merely an academic exercise; it directly influences clinical management, such as the deployment of Denosumab (a monoclonal antibody against RANKL) as a neoadjuvant therapy in complex GCTB cases to induce osteosclerosis and facilitate joint-sparing surgery.
Despite their benign histologic classification, the clinical presentation of these tumors is often marked by progressive, unrelenting pain, localized swelling, and restricted range of motion in the adjacent joint. Pathologic fractures are a frequent initial presentation, particularly in GCTB and CMF, where the tumor has significantly compromised the structural integrity of the host bone. A critical clinical pearl is the phenomenon of "benign metastasizing" GCTB; approximately 2% to 3% of GCTBs will embolize to the lungs, presenting as multiple bilateral pulmonary nodules. While these metastases are histologically benign and often indolent, they can occasionally cause progressive respiratory compromise. Consequently, routine preoperative high-resolution computed tomography (HRCT) of the chest is an absolute mandate for all patients presenting with a primary GCTB.
Detailed Surgical Anatomy and Biomechanics
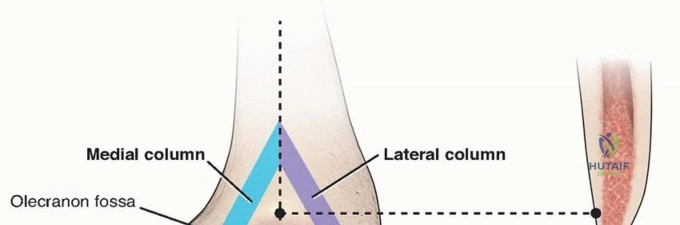
The surgical anatomy pertinent to locally aggressive bone tumors is intrinsically linked to their characteristic skeletal locations, dictating both the surgical approach and the complexity of the reconstruction. Because GCTB and Chondroblastoma are intimately associated with the articular surface—occupying the meta-epiphyseal and epiphyseal regions respectively—the surgeon must navigate the precarious millimeter-thin subchondral bone plate. In the distal femur, the tumor frequently expands into the medial or lateral condyles, threatening the insertions of the collateral ligaments and the origin of the cruciate ligaments. A thorough understanding of the extracapsular and intracapsular anatomy is paramount to ensure that the surgical approach, typically an extensile lateral or medial arthrotomy, provides adequate exposure without compromising the extensor mechanism or the vascular supply to the remaining articular cartilage.
In the pediatric population afflicted with Chondroblastoma, the surgical anatomy is further complicated by the presence of the open physis. The physis represents a critical barrier but also a highly vulnerable structure. The vascular supply to the epiphysis (epiphyseal vessels) and the metaphysis (metaphyseal vessels) must be meticulously preserved to prevent avascular necrosis of the articular segment. Surgical approaches must be carefully planned to either utilize a trans-metaphyseal route that meticulously avoids violating the growth plate, or a precise trans-epiphyseal core trajectory that minimizes the cross-sectional area of physeal damage, thereby mitigating the risk of subsequent limb-length discrepancy or angular deformity.
Osteoblastoma presents unique anatomical challenges due to its predilection for the posterior elements of the spine (pedicles, lamina, pars interarticularis, and spinous processes). The surgical anatomy here involves the intricate relationship between the expanding tumor mass, the spinal cord, exiting nerve roots, and the vertebral artery (in cervical lesions). The highly vascular nature of the tumor nidus, combined with the dense, sclerotic reactive bone that surrounds it, makes surgical navigation treacherous. Wide laminectomies or facetectomies are often required to achieve a marginal resection, which inherently destabilizes the spinal column, necessitating a profound understanding of spinal biomechanics to execute a rigid, multi-segmental instrumented fusion.
From a biomechanical perspective, the operative management of these tumors involves a transition from a state of critical bone loss to a state of restored load-bearing capacity. The creation of a large cortical window for extended curettage introduces a massive stress riser, significantly reducing the bone's torsional and bending strength. Reconstruction must address this mechanical deficit immediately. Polymethylmethacrylate (PMMA) bone cement acts as an excellent space-filler with high compressive strength, effectively transmitting loads across the defect and allowing for immediate weight-bearing. However, PMMA has a significantly higher Young's modulus than cancellous bone, leading to stress shielding and potential long-term issues at the cement-bone interface. Conversely, cancellous bone grafting provides excellent biological integration and remodeling but lacks immediate structural integrity, requiring prolonged periods of protected weight-bearing. The biomechanical compromise is often achieved through the use of composite reconstructions, utilizing structural allografts, prophylactic plating, and subchondral bone grafting (the "sandwich technique") to distribute loads physiologically while protecting the articular cartilage from cement-induced thermal necrosis.
Exhaustive Indications and Contraindications
The decision-making process for surgical intervention in locally aggressive benign bone tumors is governed by the necessity to eradicate the lesion, alleviate pain, prevent or treat pathologic fractures, and preserve maximum joint function. Unlike latent benign tumors (e.g., non-ossifying fibromas) which can often be observed, Enneking Stage 3 / Campanacci Grade III lesions invariably require aggressive surgical management. The gold standard for the majority of these tumors remains extended intralesional curettage coupled with local adjuvant therapy and meticulous defect reconstruction. However, the specific indications vary based on the tumor's histologic diagnosis, anatomical location, and the degree of cortical and articular destruction.
For Giant Cell Tumor of Bone, Campanacci Grade I (latent) lesions are exceedingly rare but can be managed with standard intralesional curettage. Campanacci Grade II (active) lesions, which represent the vast majority of presentations, are the classic indication for extended intralesional curettage, adjuvant application, and PMMA or bone graft reconstruction. Campanacci Grade III (aggressive) lesions, characterized by cortical breakthrough and soft tissue extension, present a therapeutic dilemma. If joint salvage is deemed possible based on preoperative MRI demonstrating intact subchondral bone, extended curettage remains the primary indication. However, if the joint is entirely destroyed, or if the tumor is massive and irresectable without catastrophic loss of function, en bloc wide resection with endoprosthetic or allograft reconstruction becomes the definitive indication.
Chondroblastoma and Osteoblastoma carry universal indications for prompt surgical intervention upon diagnosis. Chondroblastomas, due to their epiphyseal location, will inevitably cause progressive joint destruction, secondary osteoarthritis, and potential physeal arrest if left untreated. Osteoblastomas exhibit progressive local destruction, cause severe, unrelenting pain (often unresponsive to NSAIDs, unlike osteoid osteomas), and can lead to painful scoliosis or severe neurologic compromise when located in the spine. Chondromyxoid Fibroma, given its high recurrence rate with simple curettage and its tendency to radiographically and histologically mimic low-grade chondrosarcoma, requires either extended curettage for major weight-bearing bones or en bloc marginal resection for expendable bones (e.g., proximal fibula, ribs).
Contraindications to joint-sparing extended curettage are primarily anatomical and oncological. Absolute contraindications include the complete destruction of the subchondral bone plate making joint salvage impossible, frank malignant transformation (secondary osteosarcoma), or an active, uncontrolled surgical site infection. Relative contraindications include massive soft tissue extension where a functional limb cannot be preserved, or severe medical comorbidities precluding prolonged anesthesia. In cases where neoadjuvant Denosumab is utilized for GCTB, a relative contraindication to immediate curettage is the presence of an excessively thickened, gritty neocortex that traps microscopic tumor cells, which can significantly increase the risk of local recurrence if the surgeon is not prepared to perform an exceptionally aggressive burring of the cavity walls.
| Tumor Type | Primary Surgical Indications | Preferred Surgical Procedure | Absolute Contraindications for Joint-Sparing Surgery |
|---|---|---|---|
| Giant Cell Tumor (GCTB) | Campanacci II/III, pain, impending/actual pathologic fracture. | Extended intralesional curettage + adjuvants + PMMA/Graft. | Complete subchondral destruction, malignant transformation. |
| Chondroblastoma | Diagnosis confirmed, progressive pain, risk of physeal/articular collapse. | Meticulous curettage + bone grafting (avoid PMMA near physis). | Extensive joint destruction requiring arthroplasty (rare). |
| Chondromyxoid Fibroma | Pain, impending fracture, necessity to rule out chondrosarcoma. | Extended curettage (long bones) OR En bloc resection (expendable bones). | Expendable bone location (en bloc resection preferred over curettage). |
| Osteoblastoma | Progressive pain, spinal deformity/scoliosis, neurologic deficit. | Marginal en bloc resection (preferred) or aggressive extended curettage. | Spinal instability without planned concomitant instrumented fusion. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful oncologic and reconstructive surgery for locally aggressive bone tumors. The planning phase begins with a comprehensive imaging protocol. Plain orthogonal radiographs provide the initial assessment of the tumor's location, size, matrix characteristics, and the presence of a pathologic fracture. Magnetic Resonance Imaging (MRI) with and without intravenous gadolinium contrast is the gold standard for defining the intraosseous extent of the tumor, evaluating peritumoral edema, assessing soft tissue extension, and critically, determining the integrity of the subchondral bone plate. T1-weighted, T2-weighted, and STIR sequences are essential. Furthermore, a high-resolution Computed Tomography (CT) scan is utilized for precise cortical mapping, identifying areas of cortical thinning or breach, and facilitating 3D reconstructive templating.
A definitive histologic diagnosis via a core needle biopsy is an absolute prerequisite before any definitive surgical resection. The biopsy must be meticulously planned by the operating surgeon. The biopsy tract must be placed longitudinally, directly in line with the planned definitive surgical incision, ensuring that the entire tract can be excised in continuity with the tumor during the primary surgery. Transverse incisions or biopsies that traverse multiple anatomic compartments are strictly prohibited, as they contaminate otherwise clean tissue planes. In cases of CMF, the histologic differentiation from low-grade chondrosarcoma can be notoriously difficult; thus, the biopsy must be reviewed by a specialized musculoskeletal pathologist. For spinal Osteoblastomas, preoperative selective arterial embolization performed 24 to 48 hours prior to surgery is strongly recommended to devascularize the highly vascular nidus, thereby minimizing catastrophic intraoperative hemorrhage.
Templating and the utilization of custom cutting guides or 3D-printed anatomical models have become increasingly standard in complex meta-epiphyseal reconstructions. The surgeon must template the size and location of the cortical window, ensuring it is large enough to access all recesses of the tumor cavity without compromising more than 30% to 40% of the bone's diaphyseal circumference, which would necessitate prophylactic internal fixation. If en bloc resection and endoprosthetic reconstruction are anticipated (e.g., for a Campanacci III GCTB with joint destruction), precise templating of the resection level, stem diameter, and joint line restoration is critical. Neoadjuvant therapy with Denosumab may be employed for 3 to 6 months prior to surgery to downstage massive GCTB lesions, inducing a peripheral neocortex and facilitating joint salvage; however, the surgeon must plan for a more technically demanding curettage due to the hardened, gritty nature of the treated tumor.
Patient positioning is dictated by the anatomic site and the planned surgical approach, but strict adherence to oncologic principles remains constant. For lesions of the distal femur or proximal tibia, the patient is placed supine on a fully radiolucent operating table to allow for unhindered intraoperative fluoroscopy. A sterile pneumatic tourniquet is applied to the proximal thigh. Achieving a completely bloodless surgical field is not merely a matter of convenience; it is an absolute oncologic necessity. A bloodless field is critical for visually distinguishing between the grayish, friable tumor tissue, the reactive bone, and the normal healthy cancellous bone during the extended curettage and high-speed burring phases. The limb is prepped and draped widely to allow for extensile approaches or the harvesting of autologous bone graft from the iliac crest if required.
Step-by-Step Surgical Approach and Fixation Technique
Extended Intralesional Curettage and Adjuvants
The objective of extended intralesional curettage is to completely remove the macroscopic tumor and eradicate microscopic disease residing within the reactive zone, effectively achieving a marginal oncologic margin through intralesional techniques. A longitudinal incision is made over the involved bone, incorporating the previous biopsy tract. Utilizing standard extensile approaches (e.g., a lateral approach to the distal femur, elevating the vastus lateralis), the bone is exposed. A large, oval cortical window is created using a drill and osteotomes. The dimensions of this window are critical; it must be large enough to allow direct, unhindered visualization and instrumentation of all internal recesses of the tumor cavity.
Gross curettage is initiated using large ring curettes to systematically evacuate the friable, macroscopic tumor tissue, which is sent for definitive histopathology. Following gross removal, the "extended" phase of the procedure begins, representing the most critical step in minimizing local recurrence. A high-speed spherical burr is utilized to aggressively remove 2 to 3 mm of the reactive bone lining the entire cavity. The surgeon must systematically burr down to normal, bleeding cancellous bone. Special attention must be paid to the subchondral plate; the burr must be used with extreme delicacy to remove adjacent tumor without breaching the articular cartilage.
To further eradicate microscopic disease, chemical or physical adjuvants are systematically applied to the cavity walls. Phenol (89%) is a potent protein coagulant; it is applied using cotton applicators for three cycles of one minute each, followed by meticulous neutralization with absolute alcohol or copious saline lavage. Alternatively, Hydrogen Peroxide (3%) can be used to induce oxidative stress and mechanical bubbling, which clears microscopic debris from trabecular spaces. Argon Beam Coagulation is highly effective, delivering uniform, superficial thermal necrosis (2-3 mm deep) to the cavity walls. Liquid nitrogen (cryotherapy) provides profound deep necrosis but carries a significantly high risk of iatrogenic post-operative fracture and is therefore used with extreme caution.
Giant Cell Tumor of Bone Reconstruction
Following the application of adjuvants, the cavity is thoroughly irrigated with pulsatile lavage. Reconstruction of GCTB defects is typically performed using Polymethylmethacrylate (PMMA) bone cement. PMMA provides immediate structural stability, allowing for early weight-bearing rehabilitation. Furthermore, the exothermic reaction of PMMA as it polymerizes and cures (reaching temperatures up to 70°C) provides a secondary, physical thermal adjuvant effect, further extending the zone of necrosis. Radiographically, PMMA is highly radiopaque; any future radiolucent line developing between the cement mantle and the host bone is a highly sensitive and specific indicator of local tumor recurrence.
To protect the joint surface from thermal necrosis when the subchondral bone plate is extremely thin (<2 mm), the "sandwich technique" is employed. A layer of cancellous allograft or autograft is densely packed against the subchondral bone and articular cartilage. A layer of Gelfoam is often placed over the graft, and the remainder of the cavity is subsequently filled with pressurized PMMA. If the cortical window is exceptionally large, or if the remaining cortical bone is deemed mechanically insufficient, prophylactic internal fixation utilizing locking plates and screws is applied to bypass the stress riser and prevent postoperative pathologic fracture.
Chondroblastoma and Physeal Preservation
The surgical technique for Chondroblastoma is heavily influenced by the necessity to preserve the open physis and the adjacent articular cartilage. The approach is dictated by the lesion's precise location. For femoral head lesions, a surgical dislocation of the hip or a core decompression approach utilizing fluoroscopic guidance may be utilized. Recent literature highly supports the use of arthroscopic-assisted resection for intra-articular or subchondral lesions, allowing for direct visualization of the articular cartilage during curettage to prevent iatrogenic breach.
If the physis is open, a trans-metaphyseal approach is preferred, carefully angling the curettes to access the epiphyseal lesion without violating the growth plate. If the lesion is entirely epiphyseal and inaccessible from the metaphysis, a precise trans-epiphyseal approach using a minimal drill hole may be necessary, accepting a calculated, small risk of localized physeal arrest. Crucially, Phenol and PMMA are generally contraindicated in the treatment of Chondroblastoma due to the high risk of chemical and thermal necrosis to the sensitive physis and articular cartilage. Instead, extended curettage relies heavily on aggressive mechanical burring and pulsatile lavage. The resulting cavity is densely packed with cancellous autograft (harvested from the iliac crest) or structural allograft to provide biological support and promote rapid incorporation.
Osteoblastoma and Spinal Resection
The surgical approach for Osteoblastoma depends heavily on its appendicular versus spinal location. For appendicular metaphyseal lesions, aggressive intralesional curettage with a high-speed burr is performed, similar to GCTB, though the nidus is exceptionally vascular and gritty. For diaphyseal cortical lesions, an en bloc marginal resection (removing the tumor with a continuous cuff of normal bone) is preferred to guarantee complete removal. The resulting segmental defect is reconstructed with structural intercalary allografts and rigid plate fixation.
Spinal Osteoblastomas require a highly specialized approach. Following preoperative embolization, the goal is complete marginal excision. Intralesional curettage in the spine carries an unacceptably high recurrence rate and risks catastrophic epidural tumor seeding. If the tumor involves the pedicle or lamina and causes spinal canal stenosis, a wide laminectomy or facetectomy is meticulously performed to decompress the neural elements and achieve a marginal resection. Because this extensive bony resection inherently destabilizes the spinal segment, concomitant posterior spinal instrumentation and fusion—utilizing pedicle screws, rods, and autologous bone grafting—are universally required to restore spinal column stability and alignment.
Complications, Incidence Rates, and Salvage Management
The operative management of locally aggressive bone tumors is fraught with potential complications, ranging from local oncologic failure to catastrophic structural collapse. The most prevalent complication across all tumor types in this category is local recurrence. Despite meticulous extended intralesional curettage and the use of adjuvants, the local recurrence rate for GCTB ranges from 15% to 25%. Chondroblastoma exhibits a recurrence rate of 10% to 15%, while Chondromyxoid Fibroma can recur in up to 25% to 30% of cases if treated with simple curettage alone (reduced to <5% with extended techniques or en bloc resection). Recurrence typically presents within the first two to three years postoperatively and is identified radiographically by progressive osteolysis or a new radiolucent halo around a PMMA cement mantle.
Structural and biomechanical failures constitute the second major category of complications. Iatrogenic intraoperative fractures or postoperative pathologic fractures occur in 5% to 10% of cases, primarily due to an underestimation of the mechanical compromise caused by the cortical window or failure to utilize prophylactic internal fixation. Subchondral collapse and secondary osteoarthritis are significant risks, particularly in GCTB and Chondroblastoma, where the tumor has extensively undermined the articular surface. Thermal necrosis of the articular cartilage from PMMA curing, or chemical necrosis from phenol seepage, can accelerate this degenerative process. In the pediatric population treated for Chondroblastoma, physeal arrest leading to limb-length discrepancy or angular deformity is a dreaded complication, occurring in approximately 5% to 8% of trans-epiphyseal approaches.
Biological complications include deep surgical site infections, which occur in 2% to 5% of cases, heavily influenced by the duration of surgery, the size of the soft tissue envelope, and the use of massive allografts. The most devastating, albeit rare, biological complication is malignant transformation. Secondary osteosarcoma or undifferentiated pleomorphic sarcoma can arise in the bed of a previously treated GCTB in approximately 1% to 2% of cases. This risk is exponentially increased if the patient previously received radiation therapy for an unresectable lesion. Malignant transformation is characterized by rapid, destructive bone loss, soft tissue mass formation, and a profound change in the patient's pain profile, necessitating immediate wide en bloc resection and systemic chemotherapy.
| Complication | Estimated Incidence | Primary Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Local Recurrence | 15% - 25% (GCTB) | Incomplete extended curettage, microscopic residual disease. | Repeat extended curettage + adjuvants; En bloc resection if joint destroyed. |
| Postoperative Fracture | 5% - 10% | Large cortical window (>30% diameter), lack of prophylactic plating. | Open Reduction Internal Fixation (ORIF) + supplemental grafting/PMMA. |
| Secondary Osteoarthritis | 10% - 20% | Subchondral collapse, thermal/chemical cartilage necrosis. | Joint-preserving osteotomy (early); Total Joint Arthroplasty (late/severe). |
| Physeal Arrest (Deformity) | 5% - 8% (Pediatric) | Iatrogenic damage during trans-epiphyseal approach. | Epiphysiodesis (contralateral), corrective osteotomies, limb lengthening. |
| Malignant Transformation | 1% - 2% (GCTB) | Prior radiation therapy, multiple local recurrences. | Wide en bloc resection, endoprosthetic reconstruction, systemic chemotherapy. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation of patients treated for locally aggressive bone tumors must be meticulously tailored to the anatomic location of the tumor, the extent of the bony resection, and the specific reconstructive modality utilized. The overarching goal is to restore normal joint kinematics and muscular strength while protecting the structural integrity of the reconstruction until definitive biological healing or mechanical stability is assured.
Phase I: Immediate Post-Operative Period (Weeks 0-6)
During the immediate postoperative phase, the primary objectives are wound healing, edema control, and the prevention of deep vein thrombosis. Weight-bearing status is the most critical variable and is entirely dictated by the reconstruction. If a GCTB defect was reconstructed with PMMA bone cement and the remaining cortical integrity is robust (or prophylactically plated), the patient is permitted immediate weight-bearing as tolerated. The high compressive strength of PMMA allows for early mechanical loading. Conversely, if the defect was reconstructed with cancellous autograft or allograft (as is standard for Chondroblastoma and Osteoblastoma), the patient is strictly restricted to toe-touch or partial weight-bearing. Early, passive, and active-assisted range of motion (ROM) exercises of the adjacent joints are initiated immediately to prevent capsular contractures and preserve articular cartilage nutrition.
Phase II: Intermediate Rehabilitation (Weeks 6-12)
As the patient enters the intermediate phase, radiographic evaluation is critical. For bone graft reconstructions, evidence of early graft incorporation and cortical consolidation must be observed before advancing weight-bearing status. Patients are progressively transitioned to full weight-bearing. Physical therapy focuses on aggressive active ROM and the initiation of closed-kinetic-chain strengthening exercises. Proprioceptive training and gait normalization are emphasized. For spinal Osteoblastoma patients who underwent instrumented fusion, rigid orthoses (TLSO or cervical collars) may be gradually weaned during this phase, while core stabilization and paraspinal strengthening exercises are carefully introduced.
Phase III: Advanced Rehabilitation and Return to Function (Months 3-6+)
The advanced phase aims to return the patient to their pre-morbid level of function, including heavy labor or athletic activities. This requires full, painless ROM and muscular strength equal to at least 90% of the contralateral limb. Plyometric exercises, sport-specific drills, and high-impact loading are gradually introduced. However, patients with massive intra-articular resections or those requiring large structural allografts may have permanent restrictions on high-impact sports to prevent late mechanical failure of the construct.
Concurrent with physical rehabilitation, a strict oncologic surveillance protocol must be rigorously maintained. For GCTB and other aggressive lesions, plain radiographs of the operative site and a chest radiograph or high-resolution chest CT are mandated every 3 months for the first 2 years. This intensive early surveillance is designed to detect the peak incidence of both local recurrence and benign pulmonary metastasis. Surveillance is subsequently spaced to every 6 months up to 5 years, and annually thereafter up to 10 years, as late recurrences, though rare, are documented in the literature.
Summary of Landmark Literature and Clinical Guidelines
The contemporary operative management of benign and locally aggressive bone tumors is deeply rooted in decades of landmark orthopedic oncology literature and evolving international clinical guidelines. The foundational framework for understanding and treating Giant Cell Tumor of Bone was established by Campanacci et al. in their seminal 1987 publication. By analyzing hundreds of cases, Campanacci developed the three-tiered radiographic grading system (Latent, Active, Aggressive) that remains the universal standard for guiding surgical decision-making today. This work definitively proved that simple curettage was insufficient, firmly establishing extended intralesional curettage as the gold standard to reduce the historically high local recurrence rates.
The paradigm of surgical management for GCTB experienced a seismic shift with the introduction of Denosumab. The landmark phase II clinical trials led by Chawla et al. (2013) and Thomas et al. (2010) demonstrated the profound efficacy of this RANKL inhibitor in treating unresectable GCTB and downstaging massive Campanacci III lesions. These studies showed that Denosumab rapidly eliminates the multinucleated giant cells, halts bone destruction, and induces a dense
