Operative Management of Benign Bone Tumors of the Hand

Key Takeaway
Benign and locally aggressive bone tumors of the hand, including osteochondromas, giant cell tumors, and aneurysmal bone cysts, require meticulous surgical planning. Treatment ranges from marginal excision to wide resection and reconstruction. This guide details the indications, biomechanics, and step-by-step surgical approaches for managing these complex upper extremity neoplasms while preserving hand function and minimizing recurrence.
Comprehensive Introduction and Patho-Epidemiology
The evaluation and management of osseous and synovial neoplasms within the intricate anatomical confines of the hand demand a rigorous, evidence-based, and highly structured approach. While the vast majority of primary hand tumors are benign, their anatomical proximity to critical neurovascular structures, delicate flexor and extensor tendon mechanisms, and complex articular surfaces makes surgical intervention exceptionally challenging. The primary objectives of operative orthopaedic oncology in this domain are the complete eradication of the neoplastic lesion, the meticulous preservation of biomechanical function, and the absolute minimization of local recurrence. Achieving these goals requires a profound understanding of tumor biology, advanced imaging interpretation, and masterful surgical technique.
This comprehensive chapter delineates the pathophysiology, clinical presentation, and step-by-step surgical management of four distinct, clinically significant entities: Osteochondroma, Synovial Chondromatosis, Giant Cell Tumor (GCT) of bone, and Aneurysmal Bone Cyst (ABC). Each of these pathologies presents unique epidemiological profiles and biological behaviors. Osteochondromas, while representing the most common benign bone tumors globally, are paradoxically rare in the hand and carpus. They are developmental hamartomas arising from an aberrant focus of physeal cartilage. Conversely, Synovial Chondromatosis is an unusual, typically monoarticular mechanical condition characterized by benign, nodular cartilaginous metaplasia of the synovial membrane, rarely affecting the small joints of the hand such as the proximal interphalangeal (PIP) joint.
Aneurysmal Bone Cysts and Giant Cell Tumors represent locally aggressive, expansile, osteolytic lesions that pose a significant threat to the structural integrity of the metacarpals and phalanges. ABCs are characterized by blood-filled spaces separated by connective tissue septa containing fibroblasts, osteoclast-like giant cells, and reactive woven bone. They often present with rapid, insidious enlargement and can be primary or secondary to other lesions. GCTs in the hand are notoriously problematic, occurring in a younger demographic compared to their long-bone counterparts and exhibiting a significantly higher rate of local recurrence. They are characterized by a profound proliferation of mononuclear stromal cells and multinucleated osteoclast-like giant cells, with a documented, albeit rare, potential for benign pulmonary metastasis. Understanding the nuanced patho-epidemiology of these tumors is the foundational step in formulating an effective surgical strategy.
Cellular Biology and Tumor Microenvironment
The microenvironment of these benign yet locally destructive lesions dictates their clinical behavior and response to surgical intervention. In GCTs, the neoplastic cells are actually the mononuclear stromal cells, which express RANKL (Receptor Activator of Nuclear Factor Kappa-B Ligand). This expression aggressively recruits and activates normal host monocytes to fuse into the characteristic osteoclast-like giant cells, leading to profound localized osteolysis. This biological pathway explains the aggressive cortical destruction often seen in phalangeal and metacarpal GCTs and provides a rationale for the use of medical adjuvants like denosumab in systemic or unresectable cases.
In contrast, the pathophysiology of an ABC is driven by a localized hemodynamic disturbance, often initiated by a primary neoplastic process or trauma, leading to increased venous pressure and the creation of a dilated, expansile vascular bed. The septa within the cyst are highly active, containing reactive woven bone and giant cells, but lack the true neoplastic stromal cells seen in GCTs. Synovial chondromatosis relies on a completely different biological mechanism: the metaplastic transformation of the synovial intimal layer. The synovial lining begins to spontaneously produce foci of hyaline cartilage, which subsequently detach, derive nourishment from the synovial fluid, and eventually undergo endochondral ossification. Recognizing these distinct biological drivers is essential for the operating surgeon, as it directly influences the choice between simple excision, aggressive intralesional curettage with chemical adjuvants, or wide en bloc resection.
Detailed Surgical Anatomy and Biomechanics
The surgical anatomy of the hand presents a uniquely unforgiving landscape for the orthopaedic oncologist. Unlike the appendicular skeleton of the lower extremity, where generous muscular envelopes provide robust soft-tissue coverage and wide surgical margins are more readily achievable, the hand is characterized by a paucity of expendable soft tissue. The metacarpals and phalanges are intimately surrounded by a complex network of tendons, retinacular pulleys, and neurovascular bundles. The digital arteries and nerves travel in the volar-lateral and volar-medial aspects of the digits, lying mere millimeters from the periosteum of the phalanges. Expansile tumors, such as Aneurysmal Bone Cysts and Giant Cell Tumors, frequently attenuate the overlying cortex and distend the periosteum, displacing these critical neurovascular structures from their normal anatomical pathways and placing them at extreme risk during surgical exposure.
Biomechanically, the integrity of the hand relies on the precise balance of intrinsic and extrinsic forces acting across multiple highly congruent articular surfaces. The metacarpals serve as the foundational arches of the hand, transmitting immense compressive and bending forces during grip and pinch activities. When an osteolytic lesion compromises the diaphyseal or metaphyseal cortex, the load-bearing capacity of the bone plummets, precipitating a high risk of pathological fracture. A pathological fracture in the hand is not merely a structural failure; it introduces tumor cells into the surrounding soft tissues, potentially upgrading the local stage of the disease, complicating future resections, and drastically increasing the rate of local recurrence.
Tendon Gliding and Articular Implications
Exophytic lesions, most notably Osteochondromas, present a different biomechanical challenge. While they rarely compromise the structural integrity of the host bone, their outward growth acts as a mechanical space-occupying lesion within the tightly constrained compartments of the hand. An osteochondroma arising from the dorsal aspect of a proximal phalanx can impinge upon the extensor mechanism, causing a mechanical block to active extension, progressive tendon attrition, and potentially spontaneous tendon rupture. Volar lesions may interfere with the flexor tendon within its fibro-osseous pulley system, mimicking trigger finger or causing profound restriction in the range of motion.
Furthermore, when benign tumors encroach upon the subchondral bone or directly involve the joint space—as seen in Synovial Chondromatosis or epiphyseal GCTs—the delicate articular cartilage is threatened. Synovial chondromatosis generates multiple osteocartilaginous loose bodies that act as abrasive third bodies within the joint, rapidly accelerating articular cartilage wear and leading to early-onset secondary osteoarthritis. The surgical approach must therefore be meticulously planned to not only eradicate the neoplastic tissue but also to preserve the critical gliding planes of the tendons, protect the articular cartilage, and restore the biomechanical stability of the osseous architecture, often necessitating complex structural bone grafting or polymethylmethacrylate (PMMA) reconstruction.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for a benign bone tumor of the hand requires a careful risk-benefit analysis, balancing the natural history of the specific lesion against the inherent risks of hand surgery. Observation may be appropriate for asymptomatic, latent lesions discovered incidentally; however, the unique anatomical constraints of the hand often lower the threshold for surgical intervention.
Indications for surgery are generally categorized into diagnostic, mechanical, and oncologic imperatives. Diagnostically, any rapidly growing, painful, or radiographically aggressive lesion requires an excisional or incisional biopsy to definitively rule out malignancy, such as a chondrosarcoma or osteosarcoma. Mechanically, surgery is indicated when a lesion causes pain, restricts range of motion, impinges upon neurovascular structures, or compromises the structural integrity of the bone, thereby creating an unacceptable risk of pathological fracture. Oncologically, progressive destruction of the cortex, extension into the soft tissues, or recurrence following previous treatment mandates aggressive surgical ablation. Contraindications are typically relative and encompass severe medical comorbidities precluding anesthesia, active local infection, or situations where the anticipated functional loss from surgery outweighs the morbidity of the tumor itself.
Table of Operative Indications and Contraindications
| Tumor Type | Primary Surgical Indications | Relative & Absolute Contraindications |
|---|---|---|
| Osteochondroma | Pain, neurovascular impingement, mechanical block to joint motion, progressive angular deformity, growth post-skeletal maturity (suspicion of secondary chondrosarcoma). | Asymptomatic, non-growing lesions in skeletally mature patients (Relative). Active overlying skin infection (Absolute). |
| Synovial Chondromatosis | Symptomatic loose bodies causing mechanical locking, progressive joint pain, early signs of secondary osteoarthritis, restricted ROM. | Advanced, end-stage secondary osteoarthritis where simple synovectomy is insufficient (Requires arthrodesis/arthroplasty instead). |
| Aneurysmal Bone Cyst (ABC) | Rapid insidious enlargement, dull aching pain, cortical thinning with high risk of pathological fracture, antecedent trauma exacerbation. | Lesions in the healing phase with spontaneous ossification (Relative). Medically unstable patient (Absolute). |
| Giant Cell Tumor (GCT) | Aggressive osteolysis, cortical breakthrough (Campanacci Grade II/III), pathological fracture, local recurrence, pain. | Grade I asymptomatic lesions without impending fracture (Rarely observed, but possible). Inadequate biopsy confirmation prior to definitive resection. |
Pre-Operative Planning, Templating, and Patient Positioning
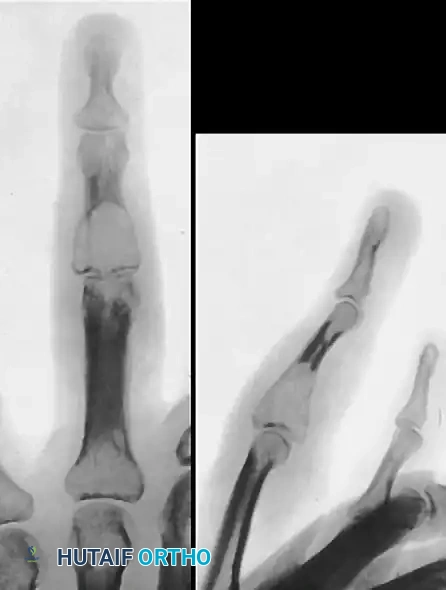
Meticulous pre-operative planning is the cornerstone of successful orthopaedic oncology in the hand. The evaluation begins with a comprehensive clinical examination, documenting the size, mobility, and exact anatomical location of the mass, as well as an exhaustive assessment of distal neurological and vascular status. Range of motion of all adjacent joints must be recorded to establish a baseline. High-quality, multi-planar plain radiographs are the initial imaging modality of choice, providing critical information regarding the lesion's matrix (e.g., calcified rings and arcs in chondroid lesions), the zone of transition, and the presence of periosteal reactions or cortical breakthrough.
Advanced cross-sectional imaging is virtually mandatory for aggressive lesions like ABCs and GCTs. Magnetic Resonance Imaging (MRI) with and without intravenous gadolinium contrast is the gold standard for defining the intraosseous extent of the tumor, evaluating soft tissue or neurovascular invasion, and assessing the thickness of the cartilage cap in osteochondromas (where a cap >1.5 cm in an adult is highly suspicious for malignant transformation). Computed Tomography (CT) is invaluable for precisely defining cortical integrity and planning the geometry of cortical windows or structural bone grafts. For highly vascular lesions such as ABCs, an arteriogram may be indicated to map the feeding vessels and plan for potential pre-operative embolization to minimize intraoperative hemorrhage.


Biopsy Principles and Operative Setup
If the diagnosis is ambiguous, a pre-operative biopsy is mandatory. The biopsy tract must be meticulously planned so that it can be completely excised en bloc during the definitive surgical procedure. In the hand, this dictates longitudinal incisions placed directly over the lesion, avoiding transverse incisions that contaminate multiple tissue planes.
Once the operative plan is finalized, templating is performed to determine the volume of bone graft or PMMA required, and to select appropriate hardware (K-wires, mini-plates) if structural reconstruction or arthrodesis is anticipated. The patient is positioned supine with the operative extremity extended onto a radiolucent hand table, allowing for unencumbered fluoroscopic access. A well-padded upper arm tourniquet is applied to ensure a bloodless surgical field, which is absolutely critical for identifying microscopic tumor tissue and protecting delicate neurovascular structures. Regional anesthesia, such as an axillary or supraclavicular brachial plexus block, is preferred as it provides excellent intraoperative muscle relaxation and prolonged post-operative analgesia, facilitating early rehabilitation.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution must be flawless, adhering strictly to oncologic principles while simultaneously respecting the delicate reconstructive requirements of the hand. The specific approach and technique vary drastically depending on the biological aggressiveness and anatomical location of the tumor.
Excisional Biopsy of Osteochondroma
For osteochondromas, the goal is complete extraperiosteal resection. A longitudinal or lazy-S incision is made directly over the palpable mass. For phalangeal lesions, a mid-axial or dorsal approach is utilized. The extensor mechanism is carefully mobilized; if the lesion is volar, the flexor tendon sheath is identified and retracted. The critical step is incising the normal periosteum at the base of the stalk and elevating it away from the lesion. The resection must include the entire cartilage cap and the overlying perichondrium to prevent recurrence. An osteotome or oscillating microsaw is used to resect the stalk flush with the normal cortical contour of the host bone. The medullary canal is inspected to ensure no residual cartilage remains.

Arthrotomy and Synovectomy for Synovial Chondromatosis
Synovial chondromatosis requires a systematic clearing of the joint space. Standard dorsal approaches to the wrist or PIP joint are utilized. A formal arthrotomy is performed, and all loose bodies are meticulously extracted. Copious irrigation with normal saline under pressure is employed to flush out microscopic cartilaginous fragments hidden in the volar recesses. A comprehensive subtotal or total synovectomy is mandatory to address the underlying metaplastic tissue. Synovial resectors and fine rongeurs are used to clear the capsule, taking extreme care not to destabilize the collateral ligaments or damage the articular cartilage.
Intralesional Curettage and Reconstruction for ABC and GCT
For locally aggressive lesions like ABCs and Grade I/II GCTs, extended intralesional curettage is the standard of care. A generous longitudinal cortical window is created to allow complete visualization of the tumor cavity. Aggressive curettage using variously angled curettes removes the gross tumor. This is followed by high-speed burring of the cavity walls to extend the margin into normal-appearing cancellous bone, breaking down the microscopic bony ridges where tumor cells harbor.

Adjuvant treatment is critical. The cavity is treated with 89% phenol (carefully applied with cotton-tipped applicators, avoiding soft tissue spillage) followed by absolute alcohol neutralization, or via cryotherapy with liquid nitrogen. The resulting defect must be reconstructed. For GCTs, packing the cavity with polymethylmethacrylate (PMMA) bone cement is highly advantageous; the exothermic reaction of polymerization provides an additional thermal adjuvant effect, it offers immediate structural stability allowing for early mobilization, and it provides a radiopaque background making the detection of early local recurrence much easier on follow-up radiographs. For ABCs, particularly in younger patients, packing with autologous cancellous bone graft from the distal radius or iliac crest is often preferred.


Wide Resection, Ray Amputation, and Transposition
For Campanacci Grade III GCTs, massive recurrent lesions, or tumors that have completely destroyed the articular surface and surrounding cortex, wide en bloc resection is required. Poorly executed marginal excisions have an unacceptably high tendency to recur. When a digit is deemed unsalvageable, a ray amputation is indicated.


A racquet-shaped incision is made around the base of the involved digit. Tendons are transected under tension to allow proximal retraction. Digital nerves are identified, drawn distally, transected sharply, and allowed to retract deep into the soft tissues to prevent painful neuroma formation. The metacarpal is osteotomized at its base. To close the resultant gap and restore the functional and cosmetic arch of the hand, a ray transposition (e.g., transposing the 5th ray to the base of the 4th metacarpal) is performed. The adjacent metacarpal is osteotomized at its base, shifted laterally, and rigidly stabilized with K-wires or a low-profile titanium plate and screws.
Complications, Incidence Rates, and Salvage Management
Surgical intervention for benign bone tumors of the hand carries a distinct profile of potential complications, heavily influenced by the tumor's biological aggressiveness and the anatomical complexity of the resection. Local recurrence is the most formidable complication, particularly in cases of Giant Cell Tumor and Aneurysmal Bone Cyst. Recurrence rates for GCTs of the hand treated with curettage alone historically approached 50-70%; however, the introduction of high-speed burring and chemical/thermal adjuvants (phenol, cryotherapy, PMMA) has reduced this incidence to approximately 15-25%. ABCs also demonstrate a notable recurrence rate of 10-20% if the curettage is not exhaustively thorough.
Intraoperative complications include iatrogenic fracture of the attenuated cortical rim during curettage or burring, and inadvertent injury to the displaced digital neurovascular bundles. Post-operative complications encompass surgical site infection, delayed wound healing (especially following the use of cytotoxic adjuvants like phenol or liquid nitrogen), and profound joint stiffness secondary to tendon adhesions or capsular contracture. Malignant transformation is exceedingly rare but remains a catastrophic complication; osteochondromas have a <1% risk of transforming into secondary chondrosarcomas, while GCTs carry a 1-2% risk of malignant transformation, often associated with prior radiation therapy.
Table of Complications and Salvage Strategies
| Complication | Estimated Incidence | Salvage Management / Prevention Strategy |
|---|---|---|
| Local Recurrence (GCT/ABC) | 15% - 25% (with adjuvants) | Salvage: Repeat aggressive curettage + PMMA, or wide en bloc resection/ray amputation. Prevention: Exhaustive high-speed burring and meticulous use of chemical adjuvants. |
| Pathological / Iatrogenic Fracture | 5% - 10% | Salvage: Internal fixation with mini-plates/K-wires, structural bone grafting, or PMMA augmentation. Prevention: Careful handling of thinned cortices; prophylactic fixation if >50% cortex destroyed. |
| Joint Stiffness / Tendon Adhesions | 20% - 30% | Salvage: Intensive hand therapy, dynamic splinting, late surgical tenolysis or capsulotomy. Prevention: Meticulous hemostasis, early active range of motion (AROM), stable fixation. |
| Neurovascular Injury | < 2% | Salvage: Primary microsurgical epineurial or vascular repair. Prevention: Careful pre-operative MRI mapping, strict adherence to anatomical planes, use of loupe magnification. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation protocol must be meticulously tailored to the specific surgical procedure performed, the stability of the osseous reconstruction, and the integrity of the surrounding soft tissues. The overarching goal is to navigate the delicate balance between protecting the surgical reconstruction and preventing the rapid onset of debilitating hand stiffness. Collaboration with a certified hand therapist (CHT) is absolutely essential for optimal functional recovery.
Phase I: Acute Protection and Edema Control (Weeks 0-2)
Immediately post-operatively, the hand is immobilized in a bulky, non-compressive dressing reinforced with a volar plaster or fiberglass splint. The wrist is typically positioned in 20-30 degrees of extension, with the metacarpophalangeal (MCP) joints in 70-90 degrees of flexion, and the interphalangeal (IP) joints in full extension (the intrinsic-plus or "safe" position). Strict elevation of the extremity above the level of the heart is enforced to combat edema, which is the primary catalyst for early stiffness. Active range of motion (AROM) of the uninvolved digits, elbow, and shoulder is initiated immediately. For simple excisional biopsies (e.g., osteochondroma) where structural integrity is uncompromised, the bulky dressing may be removed at 3-5 days, and early AROM of the involved digit is commenced to prevent tendon adhesions.
Phase II: Intermediate Mobilization and Tissue Gliding (Weeks 2-6)
At the two-week mark, sutures are removed. If a structural reconstruction was performed (e.g., bone grafting for an ABC or PMMA packing for a GCT), the hand is transitioned to a custom-molded thermoplastic splint. Gentle, progressive AROM and active-assisted range of motion (AAROM) are initiated under the guidance of the CHT. Tendon gliding exercises are emphasized to differentiate the movement of the flexor digitorum superficialis (FDS) and profundus (FDP). If a ray transposition or complex osteotomy was performed, rigid immobilization is maintained, and motion is restricted to the uninvolved digits until early radiographic signs of callus formation are evident, typically around 4-6 weeks. Pin site care (if K-wires were utilized) is performed daily with chlorhexidine or hydrogen peroxide solutions.
Phase III: Late Strengthening and Return to Function (Weeks 6-12+)
Once clinical and radiographic union of any osteotomies or bone grafts is confirmed, the protective splint is progressively weaned. Passive range of motion (PROM) and dynamic splinting may be introduced to address any residual joint contractures. Progressive resistive exercises (PREs) utilizing putty, hand grippers, and weighted devices are initiated to restore grip and pinch strength. Work hardening and sport-specific drills are incorporated late in this phase. Patients are monitored with serial radiographs at 3, 6, 12, and 24 months to ensure full consolidation of grafts and to vigilantly screen for any early signs of local tumor recurrence.
Summary of Landmark Literature and Clinical Guidelines
The operative management of benign bone tumors of the hand is heavily guided by landmark oncologic principles established over the past several decades. The Campanacci grading system remains the foundational framework for evaluating and treating Giant Cell Tumors. Campanacci's original work delineated the biological behavior of GCTs into latent (Grade I), active (Grade II), and aggressive (Grade III) categories, directly correlating the radiographic appearance with the required surgical aggressiveness. This classification dictates that while Grade I lesions may occasionally be managed with simple curettage, Grade II and III lesions mandate extended curettage with adjuvants or wide resection.
The evolution of adjuvant therapies has been extensively documented in the orthopaedic oncology literature. Studies by Balke et al. and Becker et al. have definitively demonstrated that the addition of high-speed burring and chemical adjuvants (such as phenol or liquid nitrogen) combined with PMMA reconstruction significantly reduces the local recurrence rate of hand GCTs from over 50% to approximately 20%. The use of PMMA is now widely considered the gold standard for GCT reconstruction, not only for its immediate biomechanical stability but also for its thermal necrosis effect on microscopic residual tumor cells.
Furthermore, clinical guidelines from the Musculoskeletal Tumor Society (MSTS) and the American Academy of Orthopaedic Surgeons (AAOS) emphasize the critical importance of proper biopsy techniques. A poorly executed biopsy that contaminates neurovascular bundles or separate anatomical compartments can transform a salvageable digit into one requiring amputation. Therefore, current guidelines strongly advocate that the biopsy and definitive resection should be performed by the same surgical team, ideally one with specialized training in orthopaedic oncology, ensuring that the ultimate goal of complete tumor eradication and maximal functional preservation of the hand is achieved.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons in surgical preparation and board reviews (AAOS, FRCS, Arab Board).
