
Comprehensive Introduction and Patho-Epidemiology
The evolution of total ankle arthroplasty (TAA) represents one of the most dynamic and challenging frontiers in modern orthopedic surgery. Historically, ankle arthrodesis was the gold standard for end-stage tibiotalar osteoarthritis, offering predictable pain relief at the cost of sacrificing joint kinematics and accelerating adjacent joint degeneration. However, the advent of third-generation, unconstrained, mobile-bearing prostheses has revolutionized our algorithmic approach to the arthritic ankle. Among these, the HINTEGRA Total Ankle Arthroplasty system (Integra, Plainsboro, NJ) stands as a paragon of biomechanical engineering, designed specifically to restore the complex, multi-axial kinematics of the native ankle while minimizing the mechanical stresses at the bone-implant interface that plagued earlier rigid designs.

The patho-epidemiology of ankle osteoarthritis differs profoundly from that of the hip or knee. While primary osteoarthritis dominates in larger weight-bearing joints, the vast majority of ankle arthritis—upwards of 70 to 80 percent—is post-traumatic in etiology. These patients often present with a history of recurrent instability, severe malleolar fractures, or chronic osteochondral lesions, leading to asymmetric joint space narrowing, subchondral sclerosis, and complex multi-planar deformities. Consequently, the orthopedic surgeon is frequently faced with a younger, more active demographic demanding not just pain relief, but the preservation of highly functional mobility. The HINTEGRA system addresses these demands through its three-component, unconstrained architecture, which relies on the patient's native soft-tissue envelope rather than intrinsic prosthetic constraint to dictate the limits of motion.
The HINTEGRA prosthesis is meticulously engineered from a robust cobalt-chromium alloy, featuring a dual-coated undersurface of titanium fluid and hydroxyapatite. This 20% porosity coating is critical; it facilitates rapid osteointegration and long-term biologic fixation, effectively mitigating the risk of aseptic loosening. The mobile bearing, constructed from ultrahigh-molecular-weight polyethylene (UHMWPE), features a flat tibial articulating surface and a concave talar surface. By uncoupling axial rotation from flexion-extension, the mobile bearing absorbs shear forces that would otherwise be transmitted directly to the subchondral bone. This design philosophy allows for 50 degrees of congruent contact flexion-extension and 50 degrees of axial rotation, ensuring that physiological load transfer is maintained even in the presence of minor pre-existing deformities or slight implantation deviations.
Furthermore, the anatomical design of the HINTEGRA components emphasizes bone preservation, a critical factor given the relatively small osseous volume of the talus and distal tibia. The tibial component requires a minimal subcortical resection of merely 2 to 3 millimeters, utilizing a flat 4-mm-thick loading plate with pyramidal peaks and an anterior shield for immediate rigid fixation. Similarly, the conically shaped talar component mimics the native talar dome, featuring a smaller medial radius and anatomical medial and lateral wings that resurface the degenerative facets. This hemiprosthetic resurfacing approach not only optimizes the load-transfer area but also eradicates common sources of medial and lateral gutter impingement, thereby providing a comprehensive solution to the complex pathoanatomy of the arthritic ankle.
Detailed Surgical Anatomy and Biomechanics
Mastery of the HINTEGRA total ankle arthroplasty requires an intimate, three-dimensional understanding of the ankle's surgical anatomy and its intricate biomechanical interplay. The anterior approach is the workhorse corridor for this procedure, demanding precise navigation through highly concentrated neurovascular and tendinous structures. The initial dissection traverses the skin and subcutaneous fat, immediately encountering the superior extensor retinaculum. This fascial thickening must be carefully incised and mobilized to expose the anterior compartment tendons. From medial to lateral, the surgeon must identify the tibialis anterior (TA), the extensor hallucis longus (EHL), and the extensor digitorum longus (EDL). The optimal surgical interval is typically developed between the TA and EHL tendons, allowing for robust medial and lateral soft tissue sleeves that will later facilitate secure closure and prevent tendon subluxation.
The paramount anatomical hazard during the anterior approach is the anterior neurovascular bundle, which reliably courses between the EHL and EDL tendons. This bundle comprises the deep peroneal nerve and the anterior tibial artery. The deep peroneal nerve is responsible for motor innervation to the short extensors of the foot and provides critical sensory innervation to the first dorsal web space. Iatrogenic injury to this nerve, either through direct transection or aggressive retraction neuropraxia, can result in a devastating foot drop or chronic dysesthesia. Similarly, the anterior tibial artery, the primary vascular supply to the dorsum of the foot, must be meticulously protected. Retractors must be placed subperiosteally on the tibia and talus to shield this bundle laterally, ensuring it remains unmolested throughout the bony resections.
Beyond the anterior corridor, the surgeon must possess a deep respect for the peripheral anatomy that dictates the ankle's biomechanical envelope. The superficial peroneal nerve, though lateral to the primary incision, sends medial sensory branches across the talonavicular joint; aggressive distal dissection can easily tether or sever these branches, leading to painful neuromas. Posteriorly, the posterior tibial neurovascular bundle and the flexor hallucis longus (FHL) tendon lie in close proximity to the posterior capsule. When addressing severe equinus contractures requiring posterior capsular release, the surgeon must remain keenly aware of these structures to avoid catastrophic hemorrhagic or neurologic complications. Furthermore, the integrity of the medial deltoid ligament complex and the lateral collateral ligaments is non-negotiable. Because the HINTEGRA prosthesis is unconstrained, it relies entirely on the isometric tension of these ligamentous complexes to maintain coronal plane stability and prevent bearing spin-out or dislocation.
Biomechanically, the native ankle is not a simple hinge but a complex, multi-axial joint whose axis of rotation changes dynamically throughout the arc of motion. The unconstrained nature of the HINTEGRA system honors this complexity. The flat tibial surface allows the polyethylene meniscus to glide translationally and rotate axially, accommodating the changing instantaneous center of rotation. Meanwhile, the conical talar component, with its differing medial and lateral radii, replicates the natural frustum shape of the talus. This allows the ankle to naturally internally rotate during dorsiflexion and externally rotate during plantarflexion. The success of the procedure hinges on the surgeon's ability to balance the soft tissues perfectly; a tight deltoid will drive the bearing laterally, while lateral laxity will result in varus tilt. Therefore, the anatomical dissection is not merely about exposure, but about preserving the critical soft-tissue stabilizers that will ultimately govern the kinematic fidelity of the reconstructed joint.
Exhaustive Indications and Contraindications
The decision to proceed with a total ankle arthroplasty utilizing the HINTEGRA system requires a nuanced evaluation of the patient's pathology, physiological demands, and anatomical constraints. The primary indication is debilitating, end-stage osteoarthritis of the tibiotalar joint that has proven refractory to comprehensive conservative management, including non-steroidal anti-inflammatory drugs, targeted physical therapy, bracing, and intra-articular corticosteroid or biologic injections. This encompasses primary osteoarthritis, post-traumatic arthritis (which constitutes the vast majority of cases), and systemic inflammatory arthropathies such as rheumatoid arthritis. In the rheumatoid population, TAA is particularly advantageous, as it preserves motion in a foot that may already suffer from widespread, multi-joint arthritic stiffness and spontaneous fusions.
Patient selection is arguably the most critical determinant of long-term survivorship. The ideal candidate is typically an older, lower-demand individual with a well-aligned hindfoot and preserved vascular status. However, advancements in the HINTEGRA design have cautiously expanded these indications to include younger, moderately active patients who are willing to adhere to strict postoperative activity modifications (e.g., avoiding high-impact sports like running or jumping). Furthermore, the presence of adjacent joint arthritis—specifically in the subtalar or talonavicular joints—is a strong indication for TAA over arthrodesis. Fusing an ankle in the presence of subtalar arthritis will almost certainly exacerbate midfoot pain and accelerate global foot degeneration, whereas a mobile-bearing TAA can unload these adjacent joints and dramatically improve the patient's overall gait mechanics.
Conversely, the contraindications for HINTEGRA TAA must be rigidly respected to avoid catastrophic failure. Absolute contraindications include active or recent deep soft tissue or intra-articular infection, severe peripheral vascular disease that precludes wound healing, and Charcot neuroarthropathy. The profound loss of protective sensation and catastrophic bone fragmentation seen in Charcot joints will inevitably lead to rapid aseptic loosening, subsidence, and periprosthetic fracture. Additionally, severe, uncorrectable malalignment of the hindfoot or ankle (typically defined as greater than 15 to 20 degrees of rigid varus or valgus) is an absolute contraindication unless the surgeon is prepared to perform concurrent, complex osseous realignments and ligamentous reconstructions.
Relative contraindications require careful preoperative counseling and a highly individualized risk-benefit analysis. Avascular necrosis (AVN) of the talus is a classic relative contraindication; while small, localized lesions (less than 25% of the talar body) can often be bypassed or grafted during the talar preparation, extensive AVN compromises the structural integrity required to support the talar component, risking catastrophic subsidence. Severe osteoporosis poses a similar risk for component migration. Finally, younger age (under 50 years) and high physical demands remain relative contraindications due to the increased cumulative load and the inevitable risk of polyethylene wear and aseptic loosening over the patient's extended lifespan.
| Category | Specific Conditions | Rationale / Clinical Impact |
|---|---|---|
| Primary Indications | End-stage primary or post-traumatic OA, Rheumatoid arthritis. | Restores kinematics, relieves pain, preserves adjacent joints. |
| Strong Indications | Ipsilateral subtalar or midfoot arthritis. | Arthrodesis would exacerbate adjacent joint breakdown; TAA unloads them. |
| Absolute Contraindications | Active infection, Charcot neuroarthropathy, Severe PVD. | High risk of septic failure, catastrophic subsidence, or amputation. |
| Relative Contraindications | Talar AVN (>25%), Severe Osteoporosis, Uncorrectable deformity (>20°). | Risk of component subsidence, stress shielding, or edge-loading failure. |
Pre-Operative Planning, Templating, and Patient Positioning
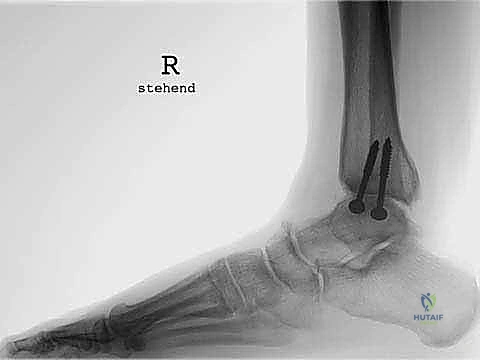
The foundation of a flawless HINTEGRA total ankle arthroplasty is laid long before the patient enters the operating theater, rooted in exhaustive preoperative planning and precise radiographic templating. Standard weight-bearing radiographs are the cornerstone of this assessment. The surgeon must obtain high-quality, standing anteroposterior (AP) views of the ankle, a lateral view of the foot and ankle, and an AP view of the foot. These images provide a macroscopic view of the tibiotalar joint destruction, the presence of osteophytes that may block motion or impinge on neurovascular structures, and the status of the syndesmosis. Crucially, weight-bearing films allow for the accurate quantification of coronal plane malalignment (varus/valgus tilt) and sagittal plane deformities (anterior or posterior translation of the talus), which dictate the required soft-tissue balancing and bone resection angles.
Templating, whether utilizing digital software or traditional acetate overlays, is a mandatory step that cannot be bypassed. The surgeon must estimate the appropriate size of both the tibial and talar components, ensuring that the implant footprint maximizes cortical rim coverage without overhanging and impinging on the malleoli. The HINTEGRA system offers six sizes, and templating helps anticipate the exact level of the tibial resection—typically aiming for a conservative 2 to 3 millimeters of subchondral bone removal to preserve the dense, load-bearing metaphyseal bone. Furthermore, templating on the lateral radiograph is vital for determining the optimal anterior-posterior position of the talar component. The center of rotation of the talar implant must align perfectly with the native anatomical axis to prevent kinematic mismatch, which would otherwise lead to early polyethylene wear and restricted range of motion.
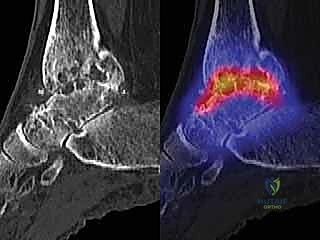
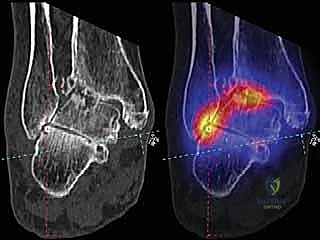
In cases of complex deformity, extensive bone loss, or suspected avascular necrosis, advanced imaging modalities become indispensable. A high-resolution computed tomography (CT) scan provides a detailed, three-dimensional topographical map of the subchondral bone stock, allowing the surgeon to precisely locate and quantify subchondral cysts that may require intraoperative curettage and bone grafting. Furthermore, Single-Photon-Emission Computed Tomography combined with CT (SPECT-CT) has emerged as a highly sophisticated tool for assessing the biologic viability of the talus. By superimposing metabolic activity (from the bone scan) over morphologic pathology (from the CT), SPECT-CT can definitively differentiate between viable, mechanically stressed bone and truly necrotic, avascular segments, thereby directly influencing the decision between TAA and arthrodesis.


Patient positioning in the operating room must be executed with meticulous attention to detail to ensure unobstructed fluoroscopic access and optimal limb alignment. The patient is positioned supine on a radiolucent operating table. A well-padded bump is placed under the ipsilateral hip to internally rotate the leg until the patella is pointing directly toward the ceiling; this neutralizes the natural external tibial torsion and ensures that the ankle mortise is perfectly aligned for true AP fluoroscopic visualization. A thigh tourniquet is applied to provide a bloodless surgical field, which is critical for identifying the delicate anterior neurovascular structures. The foot is positioned at the very edge of the table, allowing for unrestricted manipulation through a full arc of dorsiflexion and plantarflexion. Finally, the C-arm fluoroscopy unit must be brought in from the contralateral side, confirming that perfect AP and lateral views can be obtained seamlessly without breaking the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the HINTEGRA total ankle arthroplasty is a highly orchestrated sequence of precise bony resections and dynamic soft-tissue balancing. The procedure begins with a 10 to 12-centimeter longitudinal anterior incision, centered exactly between the medial and lateral malleoli, extending from the distal tibial metaphysis to the talonavicular joint. Meticulous hemostasis is achieved as the dissection deepens through the subcutaneous tissues. The superior extensor retinaculum is identified and longitudinally incised. The interval between the tibialis anterior (TA) and the extensor hallucis longus (EHL) is developed. The EHL, along with the extensor digitorum longus (EDL) and the critical anterior neurovascular bundle, is gently retracted laterally, while the TA is retracted medially. Deep self-retaining retractors are placed subperiosteally to expose the anterior capsule, which is then excised to reveal the tibiotalar joint.
The initial intra-articular step involves a comprehensive debridement. All anterior tibial and talar osteophytes must be aggressively resected using a combination of rongeurs and a high-speed burr. This osteophytectomy serves a dual purpose: it immediately restores the anterior impingement-free arc of motion and accurately delineates the true anatomical borders of the distal tibia and talar neck, which are essential landmarks for precise guide pin placement. Once the joint is cleared, the tibial alignment guide is assembled and secured to the anterior crest of the tibia, referencing the tibial tuberosity proximally to ensure perfect coronal and sagittal alignment.

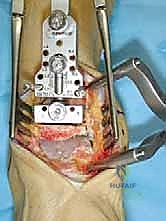
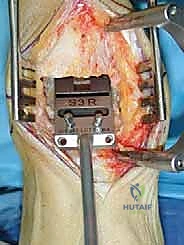
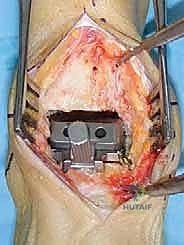
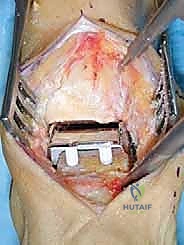
The tibial resection block is then pinned in place. The HINTEGRA system dictates a highly conservative tibial cut, removing only 2 to 3 millimeters of subchondral bone. This preserves the dense metaphyseal bone necessary to support the tibial baseplate and prevent subsidence. Under fluoroscopic guidance, the cutting block's position is verified. An oscillating saw is used to make the flat tibial cut, taking extreme care to stop short of the medial and lateral malleoli. Iatrogenic malleolar fracture during this step is a devastating complication that must be avoided by utilizing narrow saw blades and completing the corners with small osteotomes.


Following the tibial resection, attention turns to the talus. The talar cutting guide is positioned based on the previously established tibial plane, ensuring that the joint space will be perfectly rectangular in extension. The talar dome is resected to create a flat superior surface. Subsequently, the medial and lateral talar facets are prepared using specific chamfer guides and a high-speed burr or saw. The HINTEGRA talar component's unique design requires the removal of the degenerative cartilage on these facets, effectively resurfacing the medial and lateral gutters. This step requires meticulous precision to avoid violating the subtalar joint inferiorly or compromising the structural integrity of the talar body.



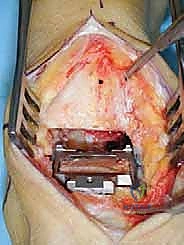
With the bony preparations complete, the trialing phase commences. Trial components for the tibia, talus, and a mobile bearing spacer are inserted. This is arguably the most critical phase of the operation, as it transitions from pure osseous geometry to dynamic soft-tissue balancing. The surgeon must assess the joint in full dorsiflexion and plantarflexion. The bearing must glide smoothly without lifting off (edge-loading) or impinging. Coronal stability is tested by applying varus and valgus stress; if the joint opens asymmetrically, targeted ligamentous releases (e.g., deep deltoid release for tight medial structures) or plications must be performed until perfect isometric tension is achieved. The thickness of the polyethylene trial (ranging from 5 to 9 mm) is adjusted to optimize ligamentous tension without overstuffing the joint.



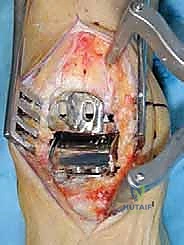
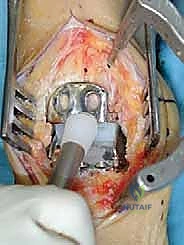
Once perfect kinematics and stability are confirmed with the trials, the final implants are introduced. The tibial component is impacted into place, allowing its pyramidal peaks to bite into the subchondral bone. The anterior shield is secured to the anterior tibial cortex using two titanium screws through oval slots, providing immediate, rigid primary fixation. The talar component is then impacted, its two pegs driving into the prepared talar dome, and its medial and lateral wings press-fitting securely against the facets. The definitive ultrahigh-molecular-weight polyethylene mobile bearing is then carefully inserted between the highly polished metallic surfaces.


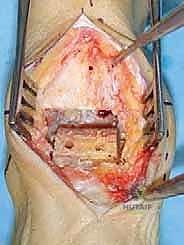
A final fluoroscopic and clinical check is mandatory. The surgeon must verify that the components are flush with the bone, the screws are appropriately seated, and the bearing is fully captured throughout the entire range of motion. Copious irrigation is performed to remove any bone debris that could trigger third-body wear. The extensor retinaculum is meticulously repaired to prevent tendon bowstringing, and the subcutaneous tissues and skin are closed in layers without tension. A sterile compressive dressing and a well-padded short-leg splint are applied with the ankle held in neutral dorsiflexion.







Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and advanced implant design, total ankle arthroplasty carries a distinct profile of intraoperative and postoperative complications that the orthopedic surgeon must be prepared to manage. Intraoperative malleolar fractures are among the most common immediate complications, occurring in approximately 2% to 5% of cases. These typically result from aggressive saw blade excursion
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding the-hintegra-total-ankle-arthroplasty