Hip Disarticulation: An Advanced Intraoperative Masterclass
Key Takeaway
Embark on an immersive journey through a hip disarticulation. This masterclass provides a granular, step-by-step guide from preoperative planning and intricate anatomical dissection to meticulous closure. Fellows will grasp neurovascular precautions, muscle interval navigation, and critical decision-making for complex limb salvage cases, ensuring optimal patient outcomes and functional recovery.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater. Today, we are undertaking an advanced, challenging, yet profoundly impactful procedure: the hip disarticulation. This intervention is not merely an amputation; it is a meticulously planned, anatomically precise resection through the coxofemoral joint, most frequently necessitated by aggressive oncological disease, severe trauma, or recalcitrant infection. Our primary objective transcends simple tumor extirpation or source control; we are simultaneously tasked with providing the patient with the most robust possible foundation for future function, prosthetic fitting, and overall quality of life. The psychological and physiological magnitude of this operation cannot be overstated, demanding the utmost respect and technical precision from the surgical team.
Historically, hip disarticulation was a procedure fraught with exorbitant mortality rates, often performed as a desperate, life-saving measure for battlefield trauma or advanced sepsis. However, with the advent of modern anesthesia, advanced cross-sectional imaging, sophisticated perioperative critical care, and multidisciplinary oncological management, the safety profile and functional outcomes of this radical amputation have improved dramatically. Today, it remains a critical weapon in the orthopedic oncologist’s armamentarium, reserved for scenarios where limb-sparing techniques are oncologically unsafe or anatomically impossible.
The patho-epidemiology of conditions necessitating hip disarticulation is heavily skewed toward high-grade musculoskeletal malignancies. Extensive soft tissue sarcomas of the proximal thigh, particularly those invading the neurovascular bundle or extending proximally toward the inguinal ligament, represent the most common indication. Primary bone sarcomas, such as osteosarcoma, Ewing sarcoma, and chondrosarcoma of the proximal femur with massive soft tissue extension or skip metastases, also frequently require this approach. Beyond oncology, we occasionally encounter catastrophic trauma with unsalvageable crush injuries or vascular compromise, as well as severe, necrotizing soft tissue infections or chronic, recalcitrant osteomyelitis of the proximal femur that threatens the patient's life.
Understanding the profound biomechanical and metabolic implications of this procedure is essential. A hip disarticulation removes the entire lever arm of the lower extremity, entirely altering the patient's center of gravity and sitting balance. The energy expenditure required for ambulation with a prosthesis following a hip disarticulation is exponentially higher—often reported to be up to 200% greater than normal, baseline ambulation. Consequently, our surgical execution must be flawless, prioritizing the creation of a durable, well-padded, and pain-free soft tissue envelope that can withstand the unique sheer and compressive forces imparted by a prosthetic socket.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of pelvic and proximal femoral anatomy is the absolute prerequisite for a successful hip disarticulation. The surgeon must navigate a complex three-dimensional labyrinth of muscular compartments, critical neurovascular bundles, and dense fascial planes.
Osteology: The Bony Compass
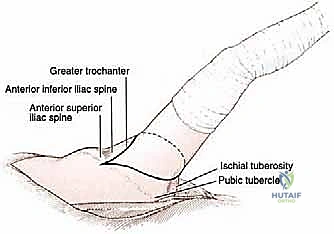
The bony architecture of the pelvis and proximal femur dictates our surgical margins and muscular releases. The pubic tubercle serves as our primary anterior landmark, situated medial to the inguinal ligament. Moving laterally, the Anterior Superior Iliac Spine (ASIS) marks the most anterior projection of the ilium and the origin of the sartorius muscle. Slightly distal and deep lies the Anterior Inferior Iliac Spine (AIIS), the origin of the rectus femoris. Posteriorly, the ischial tuberosity is a critical landmark; it is the primary weight-bearing structure during sitting and the origin of the hamstring musculature. On the proximal femur, the greater trochanter serves as the insertion point for the powerful gluteal and deep external rotator muscles, while the lesser trochanter, located medially, is the insertion site for the iliopsoas tendon. Understanding these attachments is vital, as they must be systematically detached to free the proximal femur.
Neurovascular Structures: Proceed with Caution
The neurovascular anatomy in this region is unforgiving. Anteriorly, the femoral triangle is our primary zone of danger and control. Bordered superiorly by the inguinal ligament, laterally by the sartorius, and medially by the adductor longus, it houses the femoral neurovascular bundle. The relationship of these structures, from lateral to medial, follows the classic NAVEL mnemonic: Nerve, Artery, Vein, Empty space (femoral canal), and Lymphatics. Control of the common femoral artery and vein is the most critical early step of the procedure to prevent catastrophic hemorrhage.
Deeper dissection requires management of the profunda femoris artery and its medial and lateral circumflex branches, which supply the thigh musculature and the hip joint. Medially, the obturator artery and nerve exit the obturator foramen to supply the adductor compartment. Posteriorly, the superior and inferior gluteal arteries, branches of the internal iliac system, must be meticulously identified and ligated as they exit the greater sciatic foramen. The sciatic nerve, the largest peripheral nerve in the body, exits the pelvis deep to the piriformis muscle. Its proper management—high transection and burying deep within the muscular bed—is paramount to preventing debilitating postoperative neuromas.
Muscular Intervals and Biomechanics
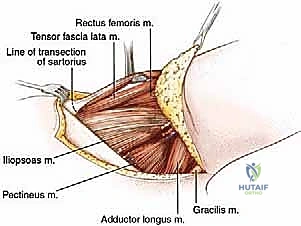
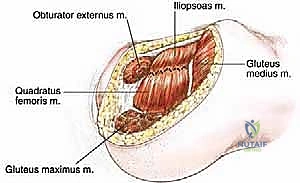
Our dissection planes navigate through distinct muscular envelopes. The outer layer comprises the tensor fascia lata, gluteus maximus, and the iliotibial band. The anterior compartment contains the sartorius, iliopsoas, rectus femoris, and pectineus. The medial compartment houses the adductor group (longus, brevis, magnus) and the gracilis. The posterior compartment includes the hamstrings, while the lateral/gluteal region contains the gluteus medius, minimus, and the short external rotators (piriformis, gemelli, obturator internus, quadratus femoris).
Biomechanically, the loss of these muscular attachments eliminates active hip flexion, extension, abduction, and adduction. The resulting stump relies entirely on the remaining gluteal musculature and the integrity of the posterior fasciocutaneous flap to provide a stable cushion against the ischial tuberosity. The hip joint capsule itself, a dense fibrous sleeve extending from the acetabular rim to the intertrochanteric line anteriorly and the femoral neck posteriorly, represents the final anatomical barrier. It must be circumferentially incised to expose the ligamentum teres, the transection of which finally liberates the lower extremity.
Exhaustive Indications and Contraindications
The decision to proceed with a hip disarticulation is never taken lightly. It requires a multidisciplinary consensus, typically involving orthopedic oncology, medical oncology, radiation oncology, vascular surgery, and rehabilitation medicine. The indications are generally absolute when life is threatened by a local disease process that cannot be eradicated by lesser means.
While limb-sparing techniques are the gold standard for most lower extremity sarcomas, specific anatomical and oncological factors mandate radical amputation. Extensive soft tissue sarcomas of the proximal thigh that encase the femoral neurovascular bundle or invade the hip joint capsule often preclude a functional or oncologically safe limb salvage. Unresectable local recurrences, particularly in previously irradiated fields where tissue planes are obliterated and wound healing is compromised, frequently necessitate disarticulation. Furthermore, pathological fractures of the proximal femur complicated by massive hematoma and tumor seeding, which are unresponsive to neoadjuvant therapies, leave disarticulation as the only viable oncological option.
In non-oncological settings, catastrophic trauma with complete avulsion of the femoral vessels and massive crush injury to the thigh musculature may require emergent disarticulation to prevent fatal crush syndrome and sepsis. Similarly, fulminant necrotizing fasciitis extending into the proximal thigh and groin, or chronic, recalcitrant periprosthetic joint infections with massive bone loss and vascular compromise, may occasionally force the surgeon's hand toward this radical extirpative procedure.
| Category | High-Yield Clinical Scenarios | Clinical Rationale & Considerations |
|---|---|---|
| Absolute Indications | Massive proximal thigh sarcoma encasing the femoral neurovascular bundle. | Limb salvage is impossible without leaving macroscopic tumor (R2 resection) or creating an ischemic, functionless limb. |
| Absolute Indications | Unresectable local sarcoma recurrence in a previously irradiated field. | Severe scarring and tissue fibrosis prevent safe margins; high risk of catastrophic wound failure with lesser procedures. |
| Absolute Indications | Catastrophic crush injury with unsalvageable vascular compromise. | Emergent life-saving measure to prevent crush syndrome, myoglobinuric renal failure, and overwhelming sepsis. |
| Relative Indications | Palliative resection for fungating, bleeding, and intractable painful tumors. | Performed strictly for quality of life improvement and local symptom control, even in the presence of known distant metastases. |
| Absolute Contraindications | Tumor involvement extending into the acetabulum or pelvic side wall. | Hip disarticulation will result in positive margins. These patients require a hemipelvectomy (internal or external). |
| Relative Contraindications | Severe cardiopulmonary comorbidities. | The massive physiological stress of the surgery and the extreme energy demands of postoperative prosthetic ambulation may be prohibitive. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a hip disarticulation is largely determined before the patient ever enters the operating room. Exhaustive preoperative planning dictates our surgical approach, anticipates anatomical variations, and ensures the achievement of wide, negative surgical margins while preserving the maximal amount of healthy tissue for flap reconstruction.
Comprehensive Imaging and Staging Studies
Advanced cross-sectional imaging is the cornerstone of our preoperative blueprint. Computed Tomography (CT) of the pelvis and lower extremity provides critical detail regarding the tumor's effect on bone integrity, identifying subtle cortical breaches or intra-articular extension that might alter our surgical margins. Furthermore, CT angiography is invaluable for mapping the vascular tree, particularly when dealing with large tumors that may displace or encase the external iliac or common femoral vessels.
Magnetic Resonance Imaging (MRI) remains the gold standard for evaluating soft tissue extension and intraosseous marrow involvement. We meticulously scrutinize the MRI for any evidence of tumor spread proximal to the lesser trochanter or into the ischiorectal fossa. Any suggestion of tumor involvement in the acetabulum or superior to the intended plane of transection is a strict contraindication to standard hip disarticulation, necessitating a shift toward hemipelvectomy. A whole-body technetium-99m bone scan or a PET-CT is mandatory to rule out distant osseous metastases, which heavily influences the overall intent of the surgery (curative versus palliative).
Biopsy and Patient Optimization
A definitive tissue diagnosis via core needle or incisional biopsy is an absolute prerequisite. The biopsy tract must be carefully planned so that it can be cleanly excised en bloc with the amputation specimen. Following diagnosis, patient optimization becomes our primary focus. Nutritional parameters (albumin, prealbumin) must be optimized to mitigate the high risk of postoperative wound complications.
Psychological preparation is equally critical. The impending loss of an entire limb is a catastrophic life event. Early integration of psychiatric support, peer counseling from functional amputees, and preoperative consultations with a certified prosthetist are essential steps to manage expectations and foster postoperative resilience. Given the extensive manipulation of major pelvic veins, patients are at an exceptionally high risk for deep venous thrombosis (DVT) and pulmonary embolism (PE). Aggressive mechanical and pharmacological DVT prophylaxis protocols are instituted, and the placement of an inferior vena cava (IVC) filter is strongly considered in high-risk patients.
Flap Design and Patient Positioning
The standard approach utilizes a long posterior myocutaneous flap, primarily composed of the gluteus maximus and overlying skin, which is folded anteriorly to close the defect. This provides a robust, well-vascularized cushion over the ischial tuberosity. However, if the tumor involves the posterior compartment or gluteal region, an atypical anterior flap based on the quadriceps musculature may be required.
For positioning, the patient is typically placed in a full lateral decubitus position on a radiolucent table, with the affected side up. The torso is rigidly secured using a vacuum beanbag, and an axillary roll is placed to protect the dependent brachial plexus. The operative leg is draped free to allow for aggressive, multi-planar manipulation—a critical requirement for exposing the various muscular compartments and ultimately dislocating the hip joint. All bony prominences on the dependent side are meticulously padded to prevent pressure necrosis during this lengthy procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a hip disarticulation is a masterclass in systematic anatomical dissection. We proceed with deliberate speed, ensuring absolute hemostasis and rigorous adherence to oncological margins.
Step 1: Incision and Initial Exposure
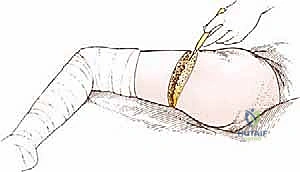
We begin by mapping our incisions based on our preoperative flap design. The standard anterior incision starts at the ASIS, curves distally and medially following the inguinal ligament toward the pubic tubercle, and extends into the perineal crease. The posterior limb begins just anterior to the greater trochanter, sweeping distally and posteriorly across the proximal thigh, extending well below the gluteal fold to ensure adequate length for the posterior flap, before curving medially to meet the anterior incision.
Using a #10 scalpel, we incise through the skin and subcutaneous tissue down to the fascia. Superficial vessels, including the superficial epigastric and superficial circumflex iliac arteries, are meticulously identified, clamped, divided, and ligated. We elevate the skin flaps slightly to expose the underlying muscular fascia, taking care not to undermine the skin excessively, which could compromise its delicate subdermal vascular plexus.
Step 2: Anterior Dissection and Neurovascular Control
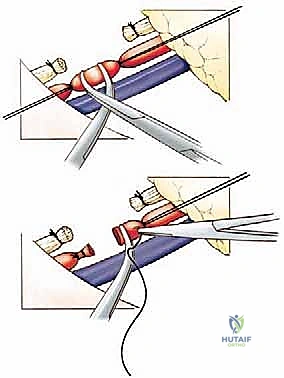
The most critical early step is securing the femoral neurovascular bundle. We incise the deep fascia over the femoral triangle, entering the fossa ovalis. The femoral sheath is opened, and we systematically isolate the structures.
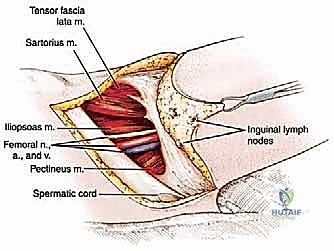
The femoral artery is isolated first. We place two heavy silk ties proximally and one distally. The artery is transected, and the proximal stump is reinforced with a suture ligature (transfixion stitch) to prevent catastrophic post-operative blowout. We then repeat this exact process for the femoral vein, taking care to avoid tearing its delicate walls, which can lead to rapid, massive hemorrhage. The femoral nerve, lying lateral to the vessels, is identified, drawn distally under gentle tension, sharply transected high within the pelvis, and allowed to retract deep into the psoas muscle belly to minimize the risk of a symptomatic neuroma.
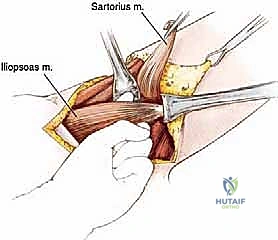
Following neurovascular control, we proceed with the anterior muscular releases. The sartorius is detached from the ASIS, and the rectus femoris is released from the AIIS. The pectineus is transected near its insertion on the femur. We then identify the iliopsoas tendon, trace it to its insertion on the lesser trochanter, and transect it, exposing the anterior capsule of the hip joint.
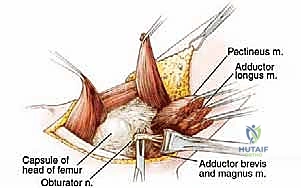
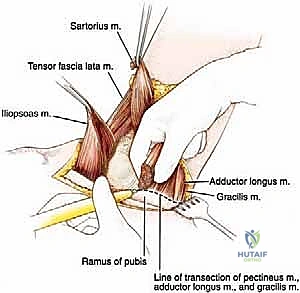
Step 3: Medial Dissection
Moving medially, we address the adductor compartment. The adductor longus, brevis, and magnus, along with the gracilis, are systematically detached from their origins on the pubis and ischium. During this phase, we must meticulously identify and ligate the obturator artery and vein as they exit the obturator foramen. The obturator nerve is similarly identified, tensioned, and transected high to allow it to retract into the pelvis.
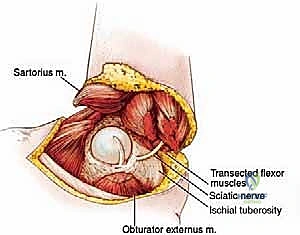
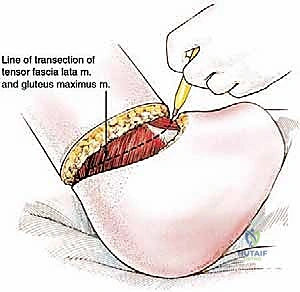
Step 4: Posterior and Lateral Dissection
The leg is now internally rotated to expose the lateral and posterior structures. We develop the posterior flap by incising the fascia lata and elevating the gluteus maximus muscle off its insertion on the linea aspera and the iliotibial tract. The gluteus maximus is reflected proximally, preserving its dominant blood supply from the superior and inferior gluteal arteries.
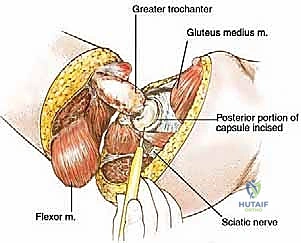
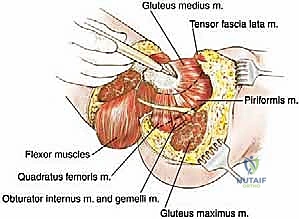
Deep to the gluteus maximus, we encounter the short external rotators (piriformis, gemelli, obturator internus, quadratus femoris). These are transected near their insertions on the greater trochanter. This exposure reveals the sciatic nerve. The management of the sciatic nerve is paramount; it is accompanied by the vasa nervorum (artery to the sciatic nerve), which can bleed profusely. The nerve is isolated, securely ligated to control the intrinsic artery, sharply transected as high as possible beneath the piriformis, and allowed to retract deep into the sciatic notch.
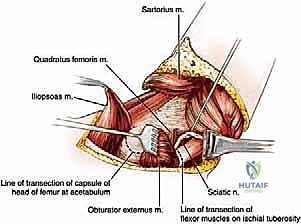
Step 5: Disarticulation and Closure
With all muscular and neurovascular attachments released, the hip joint capsule is now fully exposed circumferentially. We perform a radical capsulotomy, incising the thick fibrous tissue around the acetabular rim.
The leg is then forcefully externally rotated and extended, subluxating the femoral head from the acetabulum. This maneuver exposes the ligamentum teres, which is sharply transected with heavy Mayo scissors or a scalpel. The remaining posterior capsular attachments are divided, and the limb is completely freed and passed off the sterile field for pathological analysis.
Hemostasis is meticulously verified. The acetabulum is inspected, and any remaining articular cartilage may be curetted or left intact depending on surgeon preference, though leaving it generally causes no adverse effects. We place large-bore, closed-suction drains deep within the wound bed. The robust posterior gluteal flap is then brought anteriorly. The gluteal fascia is sutured securely to the inguinal ligament and the periosteum of the pubis, creating a strong myodesis that covers the acetabulum and provides a muscular cushion.
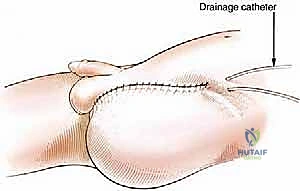
The subcutaneous tissues are closed in multiple layers with absorbable sutures to eliminate dead space, and the skin is approximated with non-absorbable sutures or surgical staples. A bulky, compressive soft dressing is applied to minimize edema and protect the incision.
Complications, Incidence Rates, and Salvage Management
Hip disarticulation is associated with a high morbidity profile, reflecting the radical nature of the resection and the often-compromised systemic state of the oncological patient. Anticipation, early recognition, and aggressive management of complications are vital for patient survival and functional recovery.
Wound complications are the most frequent source of morbidity. Flap necrosis, ranging from superficial epidermolysis to full-thickness myocutaneous failure, occurs in up to 20-30% of cases. This is particularly common in patients with prior radiation therapy, severe malnutrition, or when the posterior flap was inadvertently thinned during dissection. Management ranges from local wound care and negative pressure wound therapy (NPWT) for minor dehiscence to aggressive surgical debridement and rotational flap coverage (e.g., vertical rectus abdominis myocutaneous [VRAM] flap) for massive necrosis.
Infection, both superficial and deep, is a constant threat, exacerbated by the proximity of the incision to the perineum. Deep surgical site infections require prompt return to the operating room for radical debridement and targeted intravenous antibiotic therapy.
Phantom limb pain (PLP) and symptomatic neuromas are notoriously difficult to manage. Despite high, tensioned transection of the sciatic and femoral nerves, up to 80% of patients will experience some degree of phantom sensation or pain. Multimodal pharmacological management (gabapentinoids, tricyclic antidepressants, targeted nerve blocks) is the first line of defense. Refractory neuromas may require surgical excision and targeted muscle reinnervation (TMR), a technique increasingly utilized at the time of the index amputation to mitigate these risks.
| Complication | Estimated Incidence | Prevention & Salvage Management Strategies |
|---|---|---|
| Flap Necrosis / Dehiscence | 15% - 30% | Prevention: Preserve gluteal blood supply; optimize nutrition. Salvage: NPWT, surgical debridement, VRAM flap reconstruction. |
| Surgical Site Infection (SSI) | 10% - 25% | Prevention: Meticulous hemostasis, prolonged perioperative antibiotics, perineal isolation. Salvage: I&D, deep tissue cultures, infectious disease consultation. |
| Phantom Limb Pain / Neuroma | 50% - 80% | Prevention: High nerve transection, burying nerve ends in muscle, primary TMR. Salvage: Pharmacotherapy, desensitization therapy, surgical neuroma excision. |
| Deep Vein Thrombosis / PE | 5% - 15% | Prevention: Aggressive chemoprophylaxis, early mobilization, IVC filter in high-risk patients. Salvage: Therapeutic anticoagulation, critical care support for massive PE. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following a hip disarticulation is a marathon, not a sprint. It requires a dedicated, multidisciplinary team comprising physiatrists, physical therapists, prosthetists, and psychologists. The rehabilitation protocol is phased, ensuring tissue healing before subjecting the stump to the extreme forces of a prosthesis.
Phase 1: Acute Postoperative and Healing Phase (Weeks 0-4)
The immediate focus is on wound healing, pain control, and medical stabilization. Patients are mobilized out of bed as early as postoperative day one to prevent atelectasis and DVT. Physical therapy focuses on upper extremity strengthening, core stability, and transfers (bed to wheelchair). The stump is managed with soft compressive dressings to reduce edema and shape the soft tissues. Strict adherence to positional guidelines is enforced to prevent hip flexion contractures of the contralateral limb.
Phase 2: Pre-Prosthetic Training and Core Strengthening (Weeks 4-8)
Once the surgical wound is completely healed and the sutures are removed, the focus shifts to aggressive core and contralateral limb strengthening. The patient must develop exceptional upper body strength and cardiovascular endurance, as ambulation with a hip disarticulation prosthesis is incredibly taxing. Desensitization techniques for the stump are initiated to prepare for socket wear. Patients begin single-leg ambulation with crutches or a walker.
Phase 3: Prosthetic Fitting and Initial Ambulation (Weeks 8-12)
The gold standard for prosthetic management is the Canadian-style hip disarticulation prosthesis. This design utilizes a molded plastic socket that encases the hemipelvis, suspending over the iliac crests. The hip joint is positioned anteriorly to the weight-bearing line, providing stability during the stance phase. The fitting process requires multiple iterations by a highly skilled prosthetist. Initial ambulation occurs within parallel bars, focusing on weight shifting, pelvic control, and initiating the swing phase through pelvic tilt rather than active hip flexion.
Phase 4: Advanced Ambulation and Community Integration (Months 3+)
As the patient gains confidence and strength, training progresses to dynamic ambulation outside the parallel bars, navigating uneven terrain, ramps, and stairs. The energy expenditure remains a significant limiting factor; many patients ultimately choose to utilize a wheelchair for long distances and reserve the prosthesis for household or limited community ambulation. Continuous psychological support is crucial during this phase as patients adapt to their new functional baseline.
Summary of Landmark Literature and Clinical Guidelines
The surgical technique and oncological management surrounding hip disarticulation have been refined over decades of rigorous academic study. Historical literature, such as Boyd's seminal descriptions of the anatomical approach, laid the foundation for the modern procedure, emphasizing the necessity of the posterior gluteal flap.
Modern clinical guidelines, heavily influenced by the National Comprehensive Cancer Network (NCCN) and the Musculoskeletal Tumor Society (MSTS), dictate that hip disarticulation should be reserved for cases where limb salvage cannot achieve an R0 (microscopically negative) margin without compromising essential neurovascular structures.
Recent literature focuses heavily on functional outcomes and complication mitigation. Studies by Sugarbaker and others have extensively documented the high energy demands of prosthetic ambulation, validating the clinical observation that many older or systemically compromised patients ultimately abandon their prostheses in favor of wheelchair mobility. Furthermore, contemporary surgical literature increasingly advocates for the integration of Targeted Muscle Reinnervation (TMR) at the time of index amputation. Recent prospective trials have demonstrated that preemptive TMR significantly reduces the incidence and severity of both phantom limb pain and symptomatic neuromas, marking a paradigm shift in how we manage the transected peripheral nerves during these massive extirpative procedures.
Ultimately, hip disarticulation remains a formidable operation. However, through meticulous preoperative planning, precise anatomical dissection, and dedicated multidisciplinary rehabilitation, we can offer these patients not only definitive oncological control but also a viable pathway to functional independence and a meaningful quality of life.
