Hip Arthroscopy Masterclass: Navigating Soft Tissue Pathology and Femoroacetabular Impingement
Key Takeaway
Welcome, fellows, to an immersive hip arthroscopy masterclass. We'll meticulously dissect the anatomy, refine our preoperative planning, and execute each surgical step for soft tissue pathology, including labral tears, FAI, and ligamentum teres lesions. Expect real-time surgical directives, critical pearls, and comprehensive discussions on avoiding pitfalls and managing postoperative care. Let's scrub in.
Comprehensive Introduction and Patho-Epidemiology
The evolution of hip arthroscopy over the past two decades represents one of the most profound paradigm shifts in modern orthopedic surgery. Historically viewed as a joint inaccessible to minimally invasive techniques due to its deep anatomical location and highly constrained osseous architecture, the hip is now routinely accessed to address a myriad of complex soft tissue and bony pathologies. This transformation has been driven by a deeper biomechanical understanding of the joint, primarily the conceptualization of femoroacetabular impingement (FAI) by Ganz and colleagues, alongside rapid advancements in specialized arthroscopic instrumentation and fluid management systems. Today, arthroscopy for soft tissue pathology of the hip is not merely a diagnostic tool, but a definitive therapeutic intervention aimed at restoring native biomechanics, alleviating debilitating pain, and potentially altering the natural history of degenerative joint disease.
Before a surgeon even considers making an incision, they must possess an absolute, uncompromising mastery of the underlying patho-epidemiology. Soft tissue lesions of the hip—encompassing labral tears, articular cartilage delamination, and ligamentum teres ruptures—frequently coexist and present with remarkably similar, often insidious, symptoms. The epidemiological profile of these patients is broad, ranging from the elite adolescent athlete with acute apophyseal avulsions and labral tears to the middle-aged recreational enthusiast suffering from chronic, progressive FAI-induced chondral damage. Because the hip joint is innervated primarily by the L3 nerve root, pain is frequently referred to the medial thigh, groin, or even the knee, leading to a notoriously high rate of misdiagnosis. Many patients endure years of ineffective treatments for presumed groin strains, sports hernias, or lower lumbar radiculopathies before the true intra-articular origin of their pathology is identified.
A high index of suspicion, coupled with an exhaustive diagnostic workup, is paramount. The modern orthopedic surgeon must recognize that soft tissue pathology in the hip rarely occurs in isolation; it is almost universally the downstream consequence of an underlying morphological abnormality or a biomechanical failure. The etiologies generally distill down to a fundamental mismatch between mechanical load and tissue capacity: supraphysiologic loads applied to normal tissue (as seen in acute trauma or elite athletics), physiologic loads applied to structurally abnormal tissue (such as in developmental dysplasia of the hip), or, most commonly, mildly supraphysiologic loads repeatedly applied to mildly abnormal osseous morphology (the classic FAI scenario). Understanding this interplay is the cornerstone of successful surgical intervention.
Our goal in hip arthroscopy is never simply the debridement of torn tissue. The objective is the meticulous restoration of the joint's functional anatomy. This requires a comprehensive approach that addresses both the symptomatic soft tissue lesion and the underlying osseous deformity that caused it. Failure to recognize and correct the driving pathomorphology—for instance, repairing a labrum without resecting the offending cam lesion—will inevitably lead to surgical failure, recurrent tearing, and accelerated joint deterioration. Therefore, the masterclass in hip arthroscopy begins not with the scalpel, but with the rigorous intellectual exercise of defining the precise mechanical environment of the individual patient's hip.
Detailed Surgical Anatomy and Biomechanics
The hip joint is a masterpiece of evolutionary engineering, perfectly balancing the contradictory demands of robust weight-bearing stability and a wide, multi-planar range of motion. To navigate this space arthroscopically, the surgeon must possess a three-dimensional understanding of its structures, recognizing not just their static locations, but their dynamic interplay during the gait cycle and athletic maneuvers. The joint is divided arthroscopically into two distinct working areas: the central compartment (intracapsular, medial to the labrum, requiring traction for access) and the peripheral compartment (intracapsular, lateral to the labrum, accessed without traction).
The Acetabular Labrum and Chondrolabral Junction
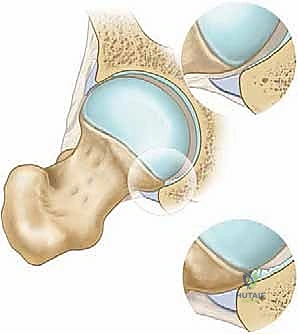
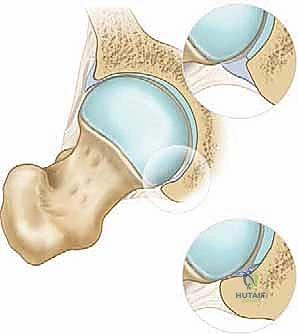
The acetabular labrum is a continuous fibrocartilaginous ring, triangular in cross-section, that attaches to the bony rim of the acetabulum. Think of it as an essential biomechanical extension of the acetabulum, deepening the socket by approximately 21% and increasing the articular surface area by 28%. While it possesses minimal intrinsic mechanical properties for primary load bearing, its most critical function is the maintenance of the joint's hydraulic seal. This seal traps synovial fluid within the central compartment, maintaining a negative intra-articular pressure that provides a suction effect, contributing significantly to joint stability. Furthermore, this pressurized fluid layer ensures boundary lubrication, protecting the underlying articular cartilage from direct mechanical shear.

The morphology and size of the labrum are highly variable. Anteriorly and superiorly, it tends to be wider and thinner, making it more susceptible to impingement and shear forces. Conversely, the posterior labrum is generally thicker, more consistent in morphology, and less frequently injured, serving as an excellent anatomical landmark during initial arthroscopic orientation. Unlike the shoulder, the hip does not possess a true capsulolabral complex; the thick hip capsule attaches to the bone of the acetabulum just proximal to the labral base. Therefore, isolated labral tears in the hip do not inherently result in gross macroscopic instability in the same manner as a Bankart lesion in the shoulder, though they do result in micro-instability due to the loss of the hydraulic seal.
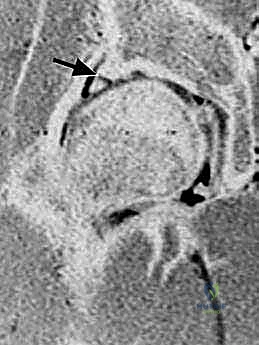
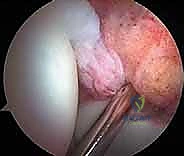
The chondrolabral junction—the transition zone between the fibrocartilaginous labrum and the hyaline articular cartilage of the lunate surface—is a critical watershed area. In a healthy joint, this transition is seamless. However, in the setting of cam impingement, the shear forces generated by the aspherical femoral head specifically target this junction. This leads to the classic "delamination" lesion, where the hyaline cartilage is sheared off the underlying subchondral bone while the labrum may remain superficially intact, creating a hidden pocket of devastating chondral damage that must be meticulously probed during diagnostic arthroscopy.
Osseous Architecture and the Ligamentum Teres
The osseous architecture of the acetabulum features the horseshoe-shaped lunate articular surface, which surrounds the non-articular central acetabular fossa. This fossa is primarily occupied by the ligamentum teres, a pulvinar of adipose tissue, and synovial folds. The transverse acetabular ligament traverses the inferior aspect of the fossa, connecting the anterior and posterior horns of the lunate surface, effectively completing the acetabular ring inferiorly. This ligament is a vital landmark for proper acetabular component positioning during arthroplasty and serves as the inferior boundary of the central compartment during arthroscopy.
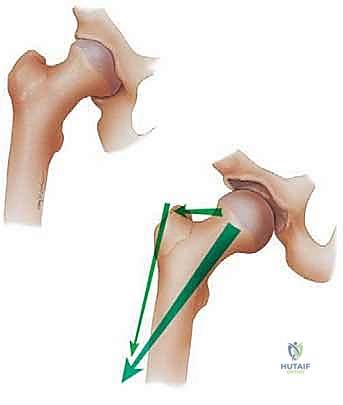
The femoral head forms approximately two-thirds of a perfect sphere, articulating with the lunate surface. Medially, the fovea capitis serves as the robust attachment site for the ligamentum teres. The relationship between the femoral head and the femoral neck is defined by the head-neck offset. Normally, the diameter of the femoral neck is about 65% of the femoral head diameter. This critical ratio, along with the normal concavity of the anterior femoral neck, allows for unimpeded, impingement-free range of motion, particularly in deep flexion and internal rotation.
The ligamentum teres is a complex, serpentine structure originating from the transverse acetabular ligament and the posterior margin of the acetabular fossa, inserting into the fovea capitis. While its primary role in childhood is to carry the artery of the ligamentum teres (a branch of the obturator artery) to supply the developing femoral head, its function in adulthood was historically dismissed as vestigial. However, contemporary research has illuminated its importance. It is heavily innervated with nociceptive and proprioceptive fibers, making it a potent pain generator when torn or inflamed. Biomechanically, it acts as a secondary stabilizer, becoming most taut in positions of adduction, flexion, and external rotation, preventing subluxation. Hypertrophy of the ligamentum teres is frequently observed in dysplastic hips, acting as a compensatory stabilizer, which paradoxically makes it more susceptible to degenerative tearing.
Pathogenesis of Femoroacetabular Impingement and Soft Tissue Lesions
The pathogenesis of intra-articular hip soft tissue lesions is predominantly mechanical. While acute macrotrauma (such as a high-energy twisting injury or a lateral impact causing an articular fracture) and purely degenerative cascades occur, the vast majority of labral and chondral pathology is driven by Femoroacetabular Impingement (FAI). FAI is a dynamic, pathomechanical process characterized by abnormal contact between the proximal femur and the acetabular rim during terminal ranges of motion.
Cam and Pincer Morphologies
FAI is broadly categorized into two primary morphological types: Pincer and Cam, though the majority of patients present with a mixed morphology. Pincer impingement is characterized by global or focal over-coverage of the femoral head by the acetabulum. This can result from general coxa profunda, protrusio acetabuli, or focal cranial retroversion of the acetabulum. In Pincer FAI, the primary point of failure is the labrum. During hip flexion, the linear impact of the femoral neck against the prominent acetabular rim crushes the labrum, leading to intrasubstance degeneration, tearing, and eventually ossification of the labral base. Secondary articular cartilage damage occurs later in the disease process, often presenting as a "contrecoup" lesion on the posteroinferior acetabulum, caused by the levering of the femoral head out of the socket during anterior impingement.
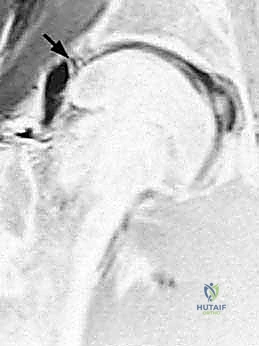
Cam impingement, conversely, is a femoral-sided pathology characterized by an aspherical femoral head-neck junction. This loss of normal concavity, often described as a "pistol grip" deformity or a decreased head-neck offset, creates a cam effect. As the hip moves into flexion and internal rotation, this prominent osseous bump is forcefully levered into the joint space. Unlike the crushing mechanism of Pincer FAI, Cam impingement generates massive shear forces directly at the anterosuperior chondrolabral junction. These shear forces cause the hyaline cartilage to delaminate from the subchondral bone, often peeling it back while leaving the labrum pushed outward. This mechanism explains why Cam lesions are associated with rapid, devastating, and often irreversible articular cartilage destruction in young, active patients.
Dysplasia, Trauma, and Degenerative Cascades
Beyond FAI, acetabular dysplasia represents the other end of the morphological spectrum. Dysplasia is characterized by insufficient acetabular coverage of the femoral head (a lateral center-edge angle of less than 20 degrees). This lack of coverage leads to a drastically reduced articular contact area. Consequently, normal physiological joint reaction forces are concentrated over a much smaller surface, leading to edge-loading. To compensate for the osseous instability, the labrum hypertrophies significantly. This enlarged, weight-bearing labrum is highly susceptible to fatigue failure, tearing, and inversion into the joint space. Recognizing dysplasia is critical, as isolated arthroscopic labral repair in a severely dysplastic hip without addressing the bony instability (e.g., via a periacetabular osteotomy) is a well-documented cause of rapid surgical failure and accelerated osteoarthritis.
Traumatic soft tissue injuries, while less common than insidious FAI, require careful evaluation. A direct lateral blow to the greater trochanter, common in contact sports or motor vehicle accidents, can transmit immense force across the joint line, resulting in acute chondral shear fractures or transchondral impaction injuries. These lesions often occur in the setting of normal osseous morphology and require high-resolution imaging for detection.
Finally, the natural history of all untreated, mechanically abnormal hips is a predictable progression toward end-stage degenerative joint disease. As the labral seal is lost and the articular cartilage delaminates, the joint environment shifts from an anabolic, well-lubricated state to a catabolic, inflammatory state. Subchondral cysts develop, osteophytes form in an attempt to stabilize the failing joint, and joint space narrowing ensues. Once advanced degenerative changes are present (Tönnis grade 2 or 3), the utility of arthroscopy diminishes precipitously, and the focus must shift toward arthroplasty.
Clinical Evaluation and Advanced Diagnostic Imaging
The clinical evaluation of the hip requires a meticulous, systematic approach. Because the hip is a deep joint, visual inspection and direct palpation are of limited utility compared to the knee or shoulder. The diagnosis relies heavily on a detailed patient history, specific provocative physical examination maneuvers, and high-quality, specialized imaging modalities. Patients typically describe an insidious onset of deep, aching groin or anterolateral hip pain. The "C-sign," where the patient cups their hand over the greater trochanter with the thumb posterior and fingers gripping deep into the anterior groin, is highly characteristic of intra-articular pathology.
Physical Examination Provocative Maneuvers
The physical examination must evaluate the lumbar spine, pelvis, and extra-articular hip structures to rule out confounding pain generators. For intra-articular pathology, the Log Roll test is highly specific. With the patient supine, the examiner passively internally and externally rotates the extended leg. This maneuver moves only the femoral head within the acetabulum without tensioning the extra-articular musculature or the joint capsule; reproduction of pain or mechanical clicking strongly suggests an intra-articular source.
The FADIR (Flexion, Adduction, Internal Rotation) test is the hallmark provocative maneuver for anterior impingement. The hip is passively flexed to 90 degrees, adducted, and internally rotated. This forces the anterolateral femoral head-neck junction against the anterosuperior acetabular rim. While highly sensitive for an irritable hip and FAI, it is not perfectly specific, as it can also aggravate iliopsoas tendinitis. The FABER (Flexion, Abduction, External Rotation) test is used to assess for concurrent sacroiliac joint pathology, intra-articular hip pathology, or iliopsoas tightness. A comprehensive assessment of bilateral range of motion is mandatory; patients with significant Cam morphology will almost universally demonstrate an obligate external rotation during hip flexion and a marked decrease in internal rotation at 90 degrees of flexion compared to the contralateral side.
Radiographic, MRI, and CT Modalities
Imaging begins with high-quality, properly positioned radiographs. An anteroposterior (AP) pelvis radiograph is non-negotiable. It must be perfectly centered over the symphysis pubis, with neutral pelvic tilt (evidenced by a distance of 1-2 cm between the tip of the coccyx and the superior border of the symphysis) and neutral rotation (symmetrical obturator foramina). This view allows for the calculation of the Lateral Center-Edge Angle (LCEA), Tönnis angle, and the assessment of Pincer signs such as the cross-over sign, prominent ischial spine sign, and posterior wall sign.

A standardized lateral radiograph of the affected hip—typically a Dunn 45-degree view or a cross-table lateral—is essential for evaluating the anterior femoral head-neck junction. This is where the alpha angle is measured; an angle greater than 50-55 degrees suggests a pathologic Cam lesion. Radiographs must also be scrutinized for subtle signs of joint space narrowing, as less than 2mm of joint space is a strong relative contraindication for arthroscopy.

Magnetic Resonance Imaging (MRI), preferably a 1.5-Tesla or 3-Tesla system using dedicated surface coils, is the gold standard for soft tissue evaluation. While standard non-contrast MRI is excellent for detecting labral tears, paralabral cysts, and subchondral edema, Magnetic Resonance Arthrography (MRA) with intra-articular gadolinium provides superior sensitivity for subtle labral detachments and chondral delamination. However, the surgeon must be cautious not to over-interpret normal anatomic variants, such as the sublabral sulcus, as pathological tears.
Computed Tomography (CT) with 3D reconstruction is increasingly utilized for preoperative templating. It provides unparalleled visualization of the complex, three-dimensional osseous morphology, allowing the surgeon to precisely map the location and extent of Cam and Pincer lesions, calculate femoral version, and plan the exact volume of bone resection required during osteochondroplasty.

Exhaustive Indications and Contraindications
The decision to proceed with hip arthroscopy must be based on a rigorous synthesis of the patient's history, physical examination, and imaging findings. The ideal candidate is a young to middle-aged, active individual with debilitating, mechanically reproducible hip pain that has failed a comprehensive trial of conservative management (including physical therapy focusing on core and pelvic/gluteal stabilization, activity modification, and potentially an intra-articular diagnostic/therapeutic corticosteroid injection) for a minimum of 3 to 6 months.
Indications include symptomatic labral tears, FAI (Cam, Pincer, or mixed), localized articular cartilage defects amenable to microfracture or chondroplasty, ligamentum teres ruptures, loose bodies, synovial chondromatosis, and certain cases of extra-articular pathology accessible via arthroscopy, such as internal or external snapping hip syndromes and proximal hamstring avulsions. The presence of mechanical symptoms—catching, locking, or sharp stabbing pain during specific movements—is a strong positive prognostic indicator for surgical success.
Conversely, patient selection is equally defined by knowing when not to operate. The most critical contraindication is advanced osteoarthritis. Arthroscopy in the setting of Tönnis grade 2 or 3 changes, or joint space narrowing of less than 2mm on any radiographic view, has a predictably high failure rate and may actually accelerate the need for total hip arthroplasty. Severe, unaddressed acetabular dysplasia (LCEA < 20 degrees) is another major contraindication; destabilizing an already shallow joint by releasing the capsule and debriding the hypertrophic labrum without addressing the bony coverage is disastrous.
| Parameter | Indications for Hip Arthroscopy | Relative / Absolute Contraindications |
|---|---|---|
| Clinical Presentation | Failed 3-6 months conservative tx; Positive mechanical symptoms (catching/locking); Positive FADIR/Log Roll; Relief from intra-articular injection. | Asymptomatic incidental findings on MRI; Primary diagnosis of lumbar radiculopathy or extra-articular pain generators. |
| Pathology | Symptomatic FAI (Cam/Pincer); Labral tears; Chondral defects; Loose bodies; Ligamentum teres rupture; Synovial disease. | Active joint infection (Absolute); Severe medical comorbidities precluding anesthesia (Absolute). |
| Radiographic Findings | Tönnis Grade 0 or 1; Joint space > 2mm; Alpha angle > 55° (Cam); LCEA 25°-39° (Normal coverage) or focal overcoverage (Pincer). | Tönnis Grade 2 or 3 (Absolute); Joint space < 2mm (Absolute); Severe Dysplasia (LCEA < 20°) without concurrent PAO (Absolute). |
| Patient Factors | Motivated patient; Realistic expectations; Commitment to rigorous post-operative rehabilitation. | Morbid obesity (Relative - limits traction and portal access); Advanced age with degenerative changes (Relative). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the foundation of a successful hip arthroscopy. Utilizing 3D CT reconstructions, the surgeon must mentally map the precise location of the impingement lesions. Knowing exactly how many millimeters of bone need to be resected from the femoral head-neck junction, and precisely where that resection should begin and end, prevents both under-resection (leading to residual impingement) and over-resection (risking iatrogenic femoral neck fracture).
Supine Versus Lateral Decubitus Positioning
Patient positioning is a matter of surgeon preference, with both the supine and lateral decubitus positions offering distinct advantages. In the supine position, the patient is placed on a specialized traction table with a well-padded, oversized perineal post. The operative leg is placed in slight flexion (10-15 degrees), abduction (10-15 degrees), and internal rotation to relax the strong iliofemoral ligament and maximize the joint space during traction. The non-operative leg is widely abducted to allow fluoroscopic access. The supine position facilitates easier orientation for surgeons transitioning from open hip surgery and provides excellent access for bilateral procedures.
In the lateral decubitus position, the patient lies on their non-operative side. Traction is applied via a specialized distractor. Proponents of this position argue that it allows the soft tissues to fall away from the joint, potentially providing better access to the peripheral compartment and reducing the risk of fluid extravasation into the abdomen. Regardless of the position chosen, the application of traction must be slow, controlled, and meticulously monitored. A minimum of 10mm of joint distraction is required to safely introduce instruments into the central compartment without scuffing the delicate articular cartilage. Traction time must be strictly limited (ideally under 90 minutes) to minimize the risk of neurapraxia to the pudendal, sciatic, or femoral nerves.
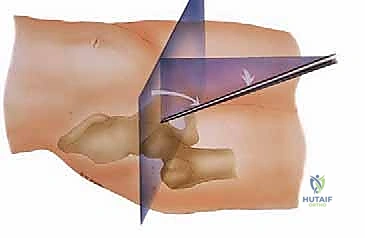
Portal Placement and Safe Zones
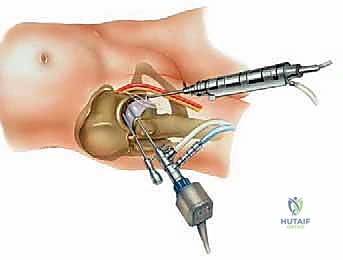
Establishing portals in the hip requires absolute precision to avoid catastrophic neurovascular injury. The joint is deep, and the margin for error is small. The three most common portals are the Anterolateral (AL), Mid-anterior (MAP), and Proximal Mid-anterior (PMAP) portals.
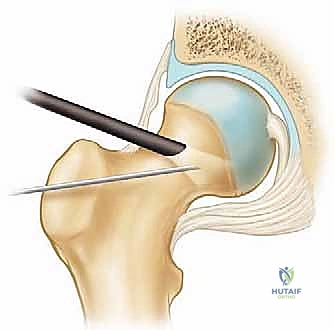
The Anterolateral (AL) portal is the workhorse viewing portal. It is established first, under fluoroscopic guidance, located 1 cm anterior and 1 cm superior to the tip of the greater trochanter. This portal enters the joint through the gluteus medius and minimizes risk to the superior gluteal nerve. The Mid-anterior (MAP) portal is created under direct arthroscopic visualization from the AL portal. It is located approximately 5-7 cm distal and slightly anterior to the AL portal, entering the joint through the interval between the rectus femoris and the gluteus medius. This portal must be placed carefully to avoid the lateral femoral cutaneous nerve (LFCN), which courses medially, and the ascending branches of the lateral circumflex femoral artery.
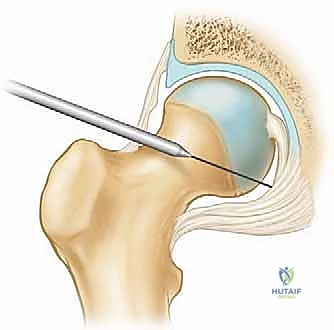
A needle is always used to localize the trajectory before making the skin incision. The capsule is thick and tough; therefore, a capsulotomy is almost universally required to maneuver instruments effectively. This is typically performed by connecting the AL and MAP portals with a specialized arthroscopic blade, cutting parallel to the labrum.
Step-by-Step Surgical Approach and Fixation Technique
The surgical procedure is systematically divided into central compartment work (performed under traction) and peripheral compartment work (performed with traction released). This structured approach ensures that all pathology is addressed efficiently while minimizing total traction time.
Diagnostic
Clinical & Radiographic Imaging Archive