

Comprehensive Introduction and Patho-Epidemiology
The evolution of total ankle arthroplasty (TAA) represents one of the most fascinating and challenging arcs in modern orthopedic surgery. For decades, ankle arthrodesis was the undisputed gold standard for end-stage tibiotalar arthritis. While arthrodesis reliably alleviates pain, it inherently sacrifices joint kinematics, leading to a profound alteration in the patient's gait cycle. This non-physiologic load transfer invariably precipitates secondary degenerative changes in the adjacent subtalar, talonavicular, and midfoot joints. The BOX (Bologna-Oxford) Total Ankle Arthroplasty emerged as a paradigm shift, designed not merely to resurface the joint, but to meticulously restore the native kinematics of the ankle mortise. Born from rigorous biomechanical analysis and the concept of the four-bar linkage mechanism, the BOX system represents a triumph of engineering tailored to the complex, multi-axial motion of the human ankle.
The patho-epidemiology of end-stage ankle arthritis differs markedly from that of the hip and knee. While primary osteoarthritis dominates the latter, ankle arthrosis is overwhelmingly post-traumatic, accounting for approximately 70% to 80% of all cases. These patients are uniquely challenging; they are typically younger, possess higher functional demands, and often present with compromised soft tissue envelopes, retained hardware, and complex multi-planar deformities resulting from prior malleolar or tibial pilon fractures. Inflammatory arthropathies, such as rheumatoid arthritis, represent another distinct demographic, characterized by symmetric joint space narrowing, profound osteopenia, and multi-joint involvement that makes the preservation of motion via TAA highly desirable.
The BOX philosophy is predicated on the understanding that the ankle is not a simple hinge joint. Instead, the talus undergoes a complex combination of rolling and sliding within the mortise, dictated by the articular geometry and the isometric fibers of the collateral ligaments. The BOX prosthesis utilizes a unique three-component, mobile-bearing design. By matching the articulating geometry of the implant to the preserved calcaneofibular and tibiocalcaneal ligaments, the system allows these native structures to guide the prosthesis through a physiologic range of motion. Unlike earlier, highly constrained designs that transmitted excessive shear forces to the bone-implant interface—leading to catastrophic aseptic loosening—the BOX system aims for full congruence across the articulating surfaces throughout the entire arc of motion, thereby minimizing polyethylene wear and maximizing survivorship.
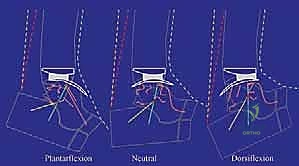
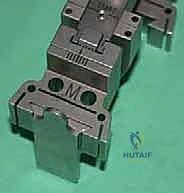
Observe the kinematic model above. It perfectly illustrates the interaction of the BOX Ankle components. In dorsiflexion, the meniscal bearing translates anteriorly on the tibial baseplate; in plantarflexion, it translates posteriorly. This coupled motion is the hallmark of the BOX system, confirming the restoration of physiologic kinematics and ensuring that the soft tissue envelope, rather than the implant geometry alone, dictates the limits of excursion.
Detailed Surgical Anatomy and Biomechanics
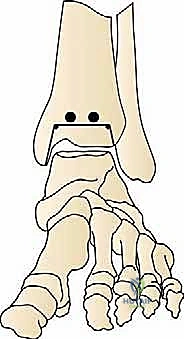
A profound understanding of the surgical anatomy and biomechanics of the tibiotalar joint is an absolute prerequisite for any surgeon undertaking total ankle arthroplasty. The ankle mortise is an inherently stable, highly congruent osseous configuration formed by the distal tibia, the medial malleolus, and the lateral malleolus. The talus, a unique bone devoid of direct muscular attachments, acts as an intercalary segment, distributing tremendous compressive and shear forces from the leg to the foot. The morphology of the talar dome is wider anteriorly than posteriorly, a critical anatomical feature that imparts stability in dorsiflexion but requires meticulous attention during bone resection to avoid iatrogenic fracture of the malleoli.
The ligamentous apparatus is the primary restraint to abnormal translation and rotation. For the BOX TAA, the integrity of the deep deltoid ligament medially and the calcaneofibular ligament (CFL) laterally is paramount. The BOX system's biomechanical foundation is the "four-bar linkage" model, which posits that normal ankle motion is governed by the interaction of the articular surfaces and the isometric fibers of the tibiocalcaneal (part of the deltoid) and calcaneofibular ligaments. During our surgical approach and subsequent balancing, we must assiduously preserve these structures. Inadvertent transection or failure to properly tension these ligaments will result in catastrophic kinematic failure of the mobile-bearing construct, leading to edge-loading, accelerated polyethylene wear, and early implant subsidence.
Navigating the neurovascular anatomy during the anterolateral approach requires surgical precision. The superficial peroneal nerve (SPN), a branch of the common peroneal nerve, pierces the deep fascia in the distal third of the leg and courses subcutaneously over the anterolateral aspect of the ankle. It is highly variable in its branching pattern and is exceptionally vulnerable during the initial skin incision and superficial dissection. Iatrogenic injury to the SPN results in debilitating neuromas and sensory deficits over the dorsum of the foot. Deeper, the anterior neurovascular bundle—comprising the deep peroneal nerve and the anterior tibial artery—lies between the extensor hallucis longus (EHL) and the extensor digitorum communis (EDC). This bundle must be identified, mobilized, and protected during the capsulotomy and subsequent placement of the tibial alignment guides.
Biomechanically, the native ankle transmits forces that can exceed five times body weight during normal walking, and up to ten times during vigorous activities. The BOX TAA mitigates these forces at the bone-implant interface through its unconstrained, mobile-bearing design. The meniscal bearing is free to translate and rotate, effectively decoupling shear forces from the tibial and talar baseplates. However, this design necessitates perfect osseous alignment. If the tibial or talar cuts are made in varus or valgus, the meniscal bearing will subluxate or edge-load. Therefore, the biomechanical success of the BOX system is entirely dependent on the surgeon's ability to execute orthogonal bone cuts relative to the mechanical axis of the tibia, while perfectly balancing the soft tissue envelope.
Exhaustive Indications and Contraindications
Patient selection is the single most critical determinant of long-term success in total ankle arthroplasty. The ideal candidate for a BOX TAA is an older patient (typically >50 years of age) with low-to-moderate functional demands, a normal body mass index (BMI), and well-aligned, end-stage tibiotalar arthrosis. Post-traumatic osteoarthritis is our most frequent indication. These patients often present with debilitating pain, stiffness, and a significant decline in their quality of life. Inflammatory arthropathies, specifically rheumatoid arthritis, represent another excellent indication. These patients frequently have multi-joint involvement; preserving motion at the ankle can protect adjacent, often already compromised, joints from accelerated degeneration.
Conversely, absolute contraindications must be strictly respected to prevent disastrous outcomes. Active or recent deep infection of the foot and ankle precludes any arthroplasty. Severe, uncorrectable malalignment (typically >15 degrees of varus or valgus) is a contraindication, as the mobile-bearing BOX system will inevitably fail under asymmetric loading. Inadequate bone stock, whether due to massive cystic degeneration, severe osteoporosis, or avascular necrosis (AVN) involving more than 50% of the talar body, prevents rigid initial fixation and will lead to early subsidence. Neuropathic joint disease (Charcot arthropathy) and severe lower extremity vascular insufficiency are also absolute contraindications due to the unacceptably high risks of catastrophic failure and wound necrosis, respectively.
Relative contraindications require nuanced clinical judgment. Younger patients (<50 years) with high physical demands are generally steered toward arthrodesis due to the finite lifespan of the polyethylene bearing and the risk of aseptic loosening over time. However, advancements in implant design and highly cross-linked polyethylene are slowly expanding this indication in carefully selected, compliant young patients. Significant obesity (BMI >35) exponentially increases the mechanical stresses on the implant and correlates with higher rates of failure. Prior adjacent joint fusions (e.g., subtalar or triple arthrodesis) increase the stress transferred to the ankle; while TAA can be performed in these scenarios to preserve remaining motion, the surgeon must counsel the patient on the potentially reduced longevity of the implant.
| Category | Specific Conditions | Rationale for Inclusion / Exclusion |
|---|---|---|
| Primary Indications | Post-traumatic OA, Rheumatoid Arthritis, Primary OA | End-stage joint destruction requiring pain relief while preserving physiologic motion to protect adjacent joints. |
| Absolute Contraindications | Active/Recent Infection, Charcot Arthropathy, Severe AVN of Talus (>50%), Uncorrectable Malalignment (>15°), Severe Vascular Insufficiency | High probability of catastrophic failure, lack of bone integration, wound necrosis, or recurrent instability. |
| Relative Contraindications | Age < 50 years, High Functional Demands, BMI > 35, Severe Osteoporosis, Correctable Malalignment | Increased risk of early mechanical failure, accelerated polyethylene wear, or subsidence. Requires extensive preoperative counseling. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the blueprint for intraoperative success; it is non-negotiable. The evaluation begins with high-quality, fully weight-bearing radiographs of the affected ankle, including anteroposterior (AP), lateral, and mortise views. Weight-bearing images are critical, as they reveal the true dynamic deformity, joint space narrowing, and subluxation that non-weight-bearing films often obscure. Furthermore, full-length weight-bearing tibial alignment films are frequently obtained to assess the mechanical axis of the lower extremity, ensuring that any extra-articular deformity is identified and accounted for. In cases of post-traumatic arthritis or suspected cystic changes, a computed tomography (CT) scan is indispensable. The CT scan allows for precise volumetric assessment of subchondral cysts and evaluation of the talar bone stock, directly influencing component sizing and the potential need for bone grafting.
Digital templating is a meticulous process that dictates our surgical strategy. We must first calibrate the digital radiographs using a known radiographic marker to correct for magnification. The BOX prosthesis system provides templates ranging from 100% to 120%. On the lateral radiograph, the tibial component is sized to maximize anteroposterior coverage without overhanging the anterior or posterior cortices, which could cause soft tissue impingement. The talar component is similarly sized to cover the talar dome. Crucially, the BOX system requires that the tibial and talar components be matched within one size of each other (e.g., a Size 3 Tibia with a Size 2, 3, or 4 Talus) to ensure appropriate kinematic interaction with the meniscal bearing. Mismatches beyond this parameter can lead to bearing spin-out or severe edge-loading.
Patient optimization prior to surgery is as important as the templating process. The soft tissue envelope must be critically evaluated. Previous surgical incisions, skin grafts, or areas of compromised vascularity dictate our surgical approach and may necessitate plastic surgery consultation for flap coverage if wound breakdown occurs. Medical comorbidities, particularly diabetes mellitus and peripheral vascular disease, must be strictly controlled. Hemoglobin A1c should ideally be below 7.0%, and non-invasive arterial studies should confirm adequate perfusion (ABI > 0.45, toe pressures > 40 mmHg) to support surgical wound healing.
In the operating theater, precise patient positioning ensures optimal access and intraoperative fluoroscopic visualization. The patient is placed supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the leg until the patella is pointing directly toward the ceiling; this neutralizes the natural external tibial torsion and presents the ankle mortise squarely to the surgeon. A well-padded thigh tourniquet is applied. The foot is positioned at the very edge of the table to allow for unhindered manipulation of the ankle and placement of the tibial alignment guides. The C-arm fluoroscopy unit is positioned on the contralateral side of the table, draped sterilely, and must be capable of obtaining perfect AP and lateral views without requiring the surgeon to alter the leg's position.
Step-by-Step Surgical Approach and Fixation Technique
The Anterolateral Approach and Deep Dissection
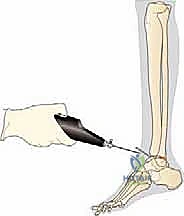
The surgical approach sets the stage for the entire procedure. After exsanguination and tourniquet inflation, an 8 to 10 cm longitudinal anterolateral incision is made. The incision is centered over the joint line, lateral to the tibialis anterior tendon, utilizing the internervous and intertendinous plane between the extensor digitorum communis (EDC) and the peroneus tertius.
Superficial dissection must be meticulous to identify and protect the superficial peroneal nerve (SPN), which often crosses the surgical field from medial to lateral. Once the SPN is safely retracted laterally, the superior and inferior extensor retinacula are incised.
We then identify the deep neurovascular bundle (anterior tibial artery and deep peroneal nerve) lying between the EHL and EDC. This bundle is carefully mobilized and retracted medially. A longitudinal capsulotomy is performed, exposing the tibiotalar joint.

Deep retractors (such as Gelpi or Weitlaner retractors) are placed directly on the osseous structures of the malleoli.
It is a critical surgical tenet to place retraction forces on the bone rather than the fragile skin edges to prevent postoperative wound necrosis.
Joint Preparation and Jig Assembly
Initial joint preparation involves a thorough anterior synovectomy and the removal of all obstructing osteophytes. A sharp chisel or rongeur is used to resect the anterior tibial exostosis and any talar neck spurs.

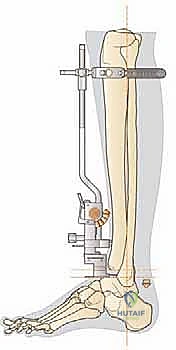
This step is vital; failure to clear the anterior gutters will limit dorsiflexion and prevent the proper seating of the cutting blocks. Once the joint is prepared, the extramedullary tibial alignment guide is assembled.
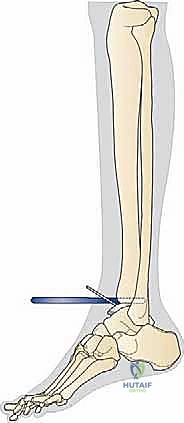
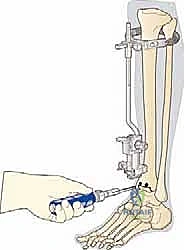
The proximal clamp is secured just distal to the tibial tubercle, and the distal assembly is aligned with the mechanical axis of the tibia. Perfect alignment in both the coronal and sagittal planes is verified via fluoroscopy.
The cutting block is pinned to the distal tibia, ensuring the resection level will remove approximately 5 to 10 mm of bone, preserving the strong subchondral plate while providing adequate space for the implant.


Osseous Resection and Joint Tensioning
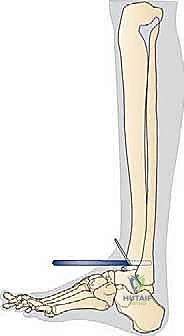
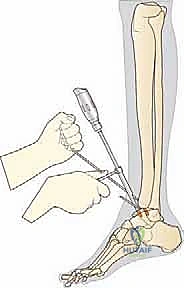
With the tibial block securely pinned, the tibial resection is performed using an oscillating saw. The saw blade must be kept perfectly flat against the cutting block. Extreme caution is exercised to protect the medial and lateral malleoli; we often use malleable retractors placed in the gutters to shield these structures from the saw blade.

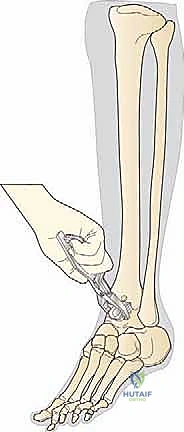
Following the tibial cut, the talar preparation begins. The BOX system employs a unique joint tensioning device that is inserted into the joint space.

This device distracts the joint, tensioning the native collateral ligaments to their physiologic state. This is the crux of the BOX philosophy: the soft tissues dictate the final position of the talar component.

Once appropriate tension is achieved and verified fluoroscopically, the talar cutting guide is pinned in place.
The talar dome is resected, typically removing about 4 mm of bone.
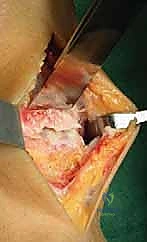
Trialing and Final Implantation
After the osseous resections are complete, trial components are inserted.
We assess the range of motion, stability, and absence of impingement. The ankle should demonstrate smooth, unconstrained dorsiflexion and plantarflexion without liftoff of the trial meniscal bearing. If the joint is too tight, further soft tissue release or a thinner bearing is required; if too loose, a thicker bearing is selected. Once the sizing is perfected, the true components are introduced.


The tibial and talar baseplates are impacted onto the prepared bone surfaces. In the cementless BOX system, initial press-fit stability is paramount for long-term biologic fixation.

Finally, the ultra-high-molecular-weight polyethylene (UHMWPE) meniscal bearing is carefully inserted between the baseplates.

We take the ankle through a final, rigorous range of motion under direct visualization and fluoroscopy to confirm absolute stability, perfect tracking of the bearing, and complete restoration of the mechanical axis.


The capsule is closed meticulously, followed by the extensor retinaculum, subcutaneous tissues, and skin, ensuring a watertight seal to protect the arthroplasty from superficial contamination.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, total ankle arthroplasty carries a distinct complication profile that the operative surgeon must be prepared to manage. Intraoperative complications are primarily mechanical. Iatrogenic fracture of the medial or lateral malleolus occurs in approximately 2% to 5% of cases, usually during the tibial resection or component impaction. If recognized intraoperatively, these must be immediately stabilized with rigid internal fixation (e.g., lag screws or tension band wiring) to allow for early rehabilitation without compromising the mortise stability. Neurovascular injuries, particularly to the superficial peroneal nerve, are devastating but highly preventable with careful superficial dissection and atraumatic retraction.
Early postoperative complications are dominated by wound healing issues. The anterior ankle skin is notoriously thin and possesses a tenuous blood supply. Superficial wound dehiscence or marginal necrosis occurs in up to 10% of cases. These are managed aggressively with local wound care, oral antibiotics, and occasionally negative pressure wound therapy. Deep periprosthetic joint infection (PJI) is less common (1% to 2%) but represents a catastrophic failure. Acute PJI may be managed with irrigation, debridement, and bearing exchange (DAIR) coupled with targeted intravenous antibiotics. Chronic PJI mandates a two-stage revision: removal of all implants, placement of an antibiotic-impregnated cement spacer, and delayed reimplantation or conversion to arthrodesis once the infection is eradicated.
Late complications are typically related to the mechanical longevity of the implant. Aseptic loosening and component subsidence are the most common reasons for revision surgery, historically occurring in 5% to 15% of patients at ten years. Periprosthetic osteolysis, driven by macrophage response to polyethylene wear debris, can lead to massive bone loss and cyst formation, destabilizing the implant. Heterotopic ossification, particularly in the posterior gutter, can progressively restrict range of motion, though it is often asymptomatic.
Salvage of a failed total ankle arthroplasty is a complex reconstructive challenge. If bone stock is adequate and the failure is isolated to bearing wear or focal loosening, a single-stage revision TAA utilizing larger, stemmed revision components may be viable. However, in cases of massive osteolysis, severe subsidence, or intractable infection, conversion to a tibiotalocalcaneal (TTC) arthrodesis is the salvage procedure of choice. This often requires the use of structural allograft (e.g., femoral head) or custom titanium cages to restore leg length, stabilized with a retrograde intramedullary nail or robust plating constructs. In extremely rare cases of unsalvageable chronic infection or catastrophic vascular
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding the-box-total-ankle-arthroplasty