Mobility Total Ankle Arthroplasty: An Intraoperative Masterclass
Key Takeaway
Join us in the OR for a comprehensive masterclass on Mobility Total Ankle Arthroplasty. We'll meticulously cover patient selection, detailed surgical anatomy, critical preoperative planning, and a granular, real-time breakdown of every intraoperative step. Learn essential pearls, pitfalls, and post-operative management strategies to optimize patient outcomes in end-stage ankle arthritis.
Comprehensive Introduction and Patho-Epidemiology
The evolution of Total Ankle Arthroplasty (TAA) represents one of the most dynamic and challenging frontiers in modern orthopedic surgery. Historically, the treatment algorithm for end-stage ankle arthritis was dominated by ankle arthrodesis. While fusion provides reliable pain relief, it fundamentally alters the biomechanics of the lower extremity, inevitably leading to accelerated adjacent-joint arthrosis—particularly within the subtalar, talonavicular, and transverse tarsal joints. The Mobility Total Ankle System emerged as a sophisticated, three-component, mobile-bearing prosthesis designed to mitigate these kinematic conflicts. By uncoupling rotational and translational forces, this system aims to restore physiological kinematics to a complex, mitered hinge joint that serves as the critical distal link in the lower extremity kinetic chain.
Unlike osteoarthritis of the hip and knee, which is predominantly primary and age-related, tibiotalar arthrosis is overwhelmingly post-traumatic in etiology. Epidemiological data suggest that up to eighty percent of ankle arthritis cases stem from previous trauma, including rotational ankle fractures, pilon fractures, recurrent ligamentous instability, and chronic microtrauma. This post-traumatic cohort presents unique surgical challenges: patients are typically younger, possess higher functional demands, and frequently exhibit complex multi-planar deformities, retained hardware, and compromised soft-tissue envelopes. Consequently, the surgical approach demands not only precise bony resection but also meticulous soft-tissue balancing and comprehensive deformity correction to ensure survivorship of the implant.




The biomechanical philosophy underpinning the Mobility TAA relies on a highly congruent articulation between the ultra-high-molecular-weight polyethylene (UHMWPE) meniscal bearing and the metallic talar and tibial components. This design maximizes contact area, thereby reducing peak contact stresses that contribute to polyethylene wear and subsequent osteolysis. Furthermore, the unconstrained nature of the mobile bearing allows the talus to seek its native axis of rotation, which is not a fixed transverse cylinder but rather a continuously changing instantaneous center of rotation during the arc of dorsiflexion and plantarflexion. Recognizing this dynamic axis is paramount; forcing the ankle into a single-axis constrained hinge leads to catastrophic early failure through aseptic loosening or component subsidence.
As orthopedic surgeons, our objective during this procedure is not merely the interposition of metal and plastic, but the holistic reconstruction of the ankle-hindfoot complex. This intraoperative masterclass will delineate the rigorous surgical technique required to implant the Mobility TAA. We will explore the nuanced decision-making processes regarding soft-tissue management, the critical importance of coronal and sagittal plane alignment, and the execution of precise osteotomies. Mastery of these elements is essential to reproducible, excellent clinical outcomes and the avoidance of devastating complications in this highly demanding patient population.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy surrounding the ankle joint is the absolute prerequisite for successful TAA. The tibiotalar joint is a highly congruent, inherently stable mortise-and-tenon structure. The tibial plafond, forming the roof of the mortise, exhibits a slight posterior slope in the sagittal plane—typically between 3 to 7 degrees. In the coronal plane, the articular surface is oriented approximately 88 to 92 degrees relative to the mechanical axis of the tibia. Preserving or restoring this spatial orientation during our initial tibial resection is critical; excessive varus or valgus cuts will lead to asymmetric edge-loading of the polyethylene bearing, accelerating wear and promoting early component failure.


The talus is a unique osseous structure, devoid of direct tendinous insertions, relying entirely on capsuloligamentous attachments for its vascular supply. Approximately sixty percent of its surface area is covered by hyaline cartilage. The talar dome (trochlea) is characterized by a dual radius of curvature, being wider anteriorly than posteriorly. This trapezoidal geometry dictates that the ankle mortise must splay slightly during maximal dorsiflexion, a movement accommodated by the elasticity of the distal tibiofibular syndesmosis. When preparing the talus for the Mobility implant, our chamfer cuts must respect the vascular watershed zones, particularly the artery of the tarsal canal and the deltoid branches, to prevent iatrogenic avascular necrosis and subsequent talar component subsidence.
The distal tibiofibular syndesmosis is the linchpin of mortise stability. Comprising the anterior inferior tibiofibular ligament (AITFL), the posterior inferior tibiofibular ligament (PITFL), the transverse ligament, and the interosseous membrane, this complex resists the lateral thrust of the talus. During the anterior approach and subsequent bony resections, meticulous care must be taken to avoid violating the syndesmotic recess. Over-resection of the lateral distal tibia can compromise the AITFL, leading to subtle syndesmotic diastasis, lateral talar shift, and catastrophic failure of the arthroplasty. If the syndesmosis is inadvertently compromised, it must be recognized and rigidly stabilized prior to closure.




Navigating the anterior muscular intervals requires precise identification of neurovascular structures. The anterior extensile approach exploits the internervous plane between the tibialis anterior (TA), innervated by the deep peroneal nerve (DPN), and the extensor hallucis longus (EHL), also innervated by the DPN. The crucial structure at risk during the superficial dissection is the superficial peroneal nerve (SPN). The SPN transitions from a deep to a subcutaneous position in the distal third of the leg, arborizing into the medial and intermediate dorsal cutaneous nerves. Its course is highly variable, and iatrogenic transection or traction neuropraxia results in debilitating neuromas and dorsal foot numbness. Deep to the extensor retinaculum, the anterior tibial artery and DPN course together. Retraction of these structures must be gentle and continuous, utilizing blunt retractors to avoid vascular intimal injury or ischemic neuropraxia.
Exhaustive Indications and Contraindications
Patient selection is arguably the most critical determinant of success in Total Ankle Arthroplasty. The primary indication for the Mobility TAA is end-stage ankle arthritis that has proven recalcitrant to exhaustive non-operative management, including activity modification, specialized orthoses (such as Arizona braces or AFOs), non-steroidal anti-inflammatory drugs, and intra-articular corticosteroid or biologic injections. The ideal candidate is an older, lower-demand individual with preserved bone stock, an intact soft-tissue envelope, and a well-aligned hindfoot. However, with advancements in implant design and surgical technique, the indications have cautiously expanded to include younger patients with post-traumatic arthrosis who wish to preserve a more physiological gait pattern than an arthrodesis would allow.



Inflammatory arthropathies, such as rheumatoid arthritis, represent an excellent indication for TAA. These patients frequently suffer from polyarticular disease; preserving motion at the ankle joint significantly reduces the compensatory burden placed on already compromised adjacent joints in the foot and knee. In this cohort, however, the surgeon must be acutely aware of osteopenic bone quality and the potential for delayed wound healing secondary to chronic immunosuppressive therapies. Perioperative management of disease-modifying antirheumatic drugs (DMARDs) and biologics must be carefully coordinated with the patient's rheumatologist to balance the risk of disease flare against the risk of periprosthetic joint infection.
Conversely, absolute contraindications must be strictly respected to prevent catastrophic complications. Active or recent deep infection of the ankle joint is an absolute barrier to primary arthroplasty. Neuropathic arthropathy, classically Charcot neuroarthropathy secondary to diabetes mellitus, is a definitive contraindication due to the loss of protective sensation, which inevitably leads to rapid implant loosening, severe bone loss, and potential amputation. Avascular necrosis (AVN) of the talus involving more than 50% of the talar body precludes the use of a standard TAA, as the necrotic bone will not support the talar component, leading to massive subsidence. In such cases of severe AVN, a custom talar replacement or a tibiotalocalcaneal (TTC) arthrodesis is the appropriate salvage pathway.
| Category | Clinical Conditions | Rationale / Surgical Implication |
|---|---|---|
| Primary Indications | End-stage osteoarthritis, Post-traumatic arthritis, Rheumatoid arthritis | Failed conservative care; desire for motion preservation and protection of adjacent joints. |
| Relative Contraindications | Severe coronal plane deformity (>15 degrees), Prior history of infection, Osteoporosis, Young age/high physical demand | Deformity requires concurrent osteotomies/fusions. High demand increases wear rates. Osteoporosis risks subsidence. |
| Absolute Contraindications | Active joint infection, Charcot neuroarthropathy, Severe talar AVN (>50%), Absent motor function (e.g., drop foot), Severe peripheral vascular disease | Guaranteed failure of implant fixation, catastrophic soft tissue breakdown, or rapid progressive loosening. |
Significant coronal plane deformities—varus or valgus angulation exceeding 15 degrees—were historically considered absolute contraindications. Today, they are viewed as relative contraindications that require concurrent or staged corrective procedures. A TAA placed in a malaligned limb will experience eccentric loading, leading to rapid polyethylene wear and edge-loading. Therefore, any varus or valgus deformity must be meticulously corrected via ligamentous balancing (e.g., deltoid release, lateral ligament reconstruction) or extra-articular osteotomies (e.g., calcaneal osteotomy, supramalleolar osteotomy) to ensure the mechanical axis passes centrally through the implanted prosthesis.
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for a Mobility TAA is a rigorous, multi-modal process that begins long before the patient enters the operating theater. The foundation of this planning rests on high-quality, weight-bearing radiographic imaging. We mandate weight-bearing anteroposterior (AP), lateral, and mortise views of the affected ankle. These images allow for the assessment of joint space narrowing, the presence and location of osteophytes, and the quality of the subchondral bone. Crucially, we must also obtain weight-bearing mechanical axis views (hip-to-ankle radiographs) to evaluate the overall alignment of the lower extremity. A subtle genu varum or valgum can significantly alter the load vectors across the ankle joint, predisposing the implant to eccentric failure if not accounted for.


Advanced cross-sectional imaging is frequently indispensable. A non-contrast Computed Tomography (CT) scan provides a three-dimensional understanding of bone stock, cystic changes, and complex post-traumatic anatomy. It is particularly useful for identifying the true center of rotation in deformed ankles and for mapping the extent of subchondral cysts that may require bone grafting during component implantation. If avascular necrosis of the talus is suspected, Magnetic Resonance Imaging (MRI) is the gold standard to quantify the volume of necrotic bone and determine if sufficient viable bone remains to support the talar component. Furthermore, a thorough vascular assessment, including Ankle-Brachial Indices (ABI) and potentially Doppler ultrasonography, is mandatory for any patient with diminished palpable pulses, as the anterior ankle incision is notoriously unforgiving in the presence of peripheral arterial disease.
Digital templating is a critical step in the preoperative workflow. Using calibrated radiographs, we overlay the digital templates of the Mobility TAA components to estimate the optimal size and position. On the lateral view, the goal is to size the talar component such that it covers the anterior-to-posterior dimension of the talus without overhanging, which could cause soft-tissue impingement. The tibial component is sized to maximize cortical bone contact on the resected plafond while avoiding impingement on the medial or lateral gutters. Templating also helps anticipate the required depth of the bony resections and identifies whether structural allograft or specialized augments will be necessary to manage large subchondral cysts or bone defects.



Patient positioning and anesthesia are optimized to facilitate a seamless surgical workflow and enhance postoperative recovery. The patient is placed in the supine position on a radiolucent operating table. It is imperative that the foot is positioned at the extreme distal edge of the table; this allows the surgeon to freely manipulate the ankle through a full arc of dorsiflexion and plantarflexion, and provides unobstructed access for the introduction of intramedullary alignment guides and cutting jigs. A well-padded bump is placed under the ipsilateral hip to internally rotate the leg, ensuring the patella and the foot are pointing directly towards the ceiling, thus neutralizing the natural external rotation of the lower limb. A proximal thigh tourniquet is applied to ensure a bloodless surgical field. Anesthesia is typically achieved via a continuous popliteal sciatic nerve block combined with a saphenous nerve block, providing profound intraoperative anesthesia and excellent postoperative analgesia while avoiding the systemic side effects of general anesthesia.
Step-by-Step Surgical Approach and Fixation Technique
The Anterior Extensile Approach
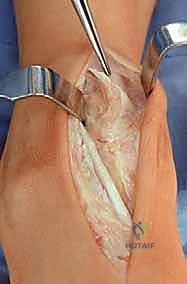
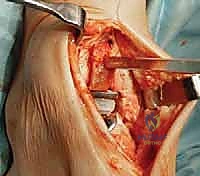
The surgical execution begins with the classic anterior extensile approach. A longitudinal incision, approximately 10 to 12 centimeters in length, is centered over the anterior joint line, coursing between the crest of the tibia and the lateral malleolus, and extending distally to the talonavicular joint. Meticulous soft-tissue handling is paramount; full-thickness fasciocutaneous flaps must be developed to preserve the delicate angiosomes supplying the anterior ankle skin. Skin edges are protected with moist lap sponges, and self-retaining retractors are placed deep to the extensor retinaculum to minimize tension on the dermal margins.

Superficial dissection requires immediate identification and protection of the superficial peroneal nerve (SPN), which frequently crosses the operative field from lateral to medial. Once the SPN is safely retracted, the superior extensor retinaculum is incised longitudinally. The deep dissection exploits the interval between the tibialis anterior (TA) tendon medially and the extensor hallucis longus (EHL) tendon laterally. The deep neurovascular bundle—comprising the anterior tibial artery and the deep peroneal nerve—lies immediately lateral to the EHL and must be identified, mobilized, and gently retracted laterally. An anterior capsulotomy is then performed, exposing the tibiotalar joint.
Joint Preparation and Osteophyte Resection
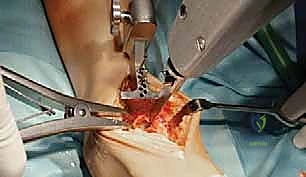
Upon entering the joint, the surgeon is typically confronted with significant anterior tibiotalar osteophytosis, which acts as a mechanical block to dorsiflexion. A thorough anterior exostectomy is performed using a combination of rongeurs and an oscillating saw. It is crucial to restore the native anterior contour of the distal tibia and the talar neck. Failure to adequately resect these osteophytes will result in impingement of the components during dorsiflexion, leading to restricted range of motion and potential lift-off of the tibial tray.




Following osteophyte resection, medial and lateral gutter releases are meticulously performed. The medial gutter is cleared of fibrotic tissue and osteophytes to expose the medial malleolar articular facet. Similarly, the lateral gutter is addressed, taking immense care not to violate the syndesmosis or the lateral ligamentous complex. A complete release of the contracted posterior capsule may also be necessary to restore physiological dorsiflexion. This extensive soft-tissue release is a critical step; the Mobility TAA relies on balanced ligaments for stability, and any residual contracture will manifest as asymmetric kinematics and premature wear.
Tibial and Talar Resections
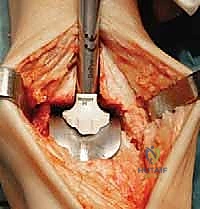
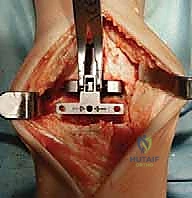
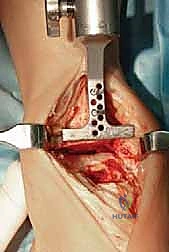
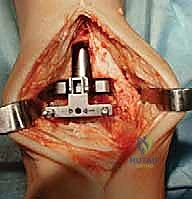
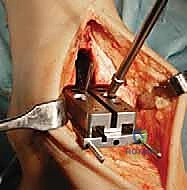
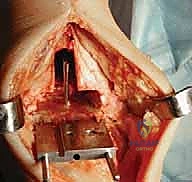
With the joint fully exposed and balanced, attention turns to the bony resections. The Mobility system utilizes an extramedullary alignment guide for the tibia, referenced off the tibial crest and the center of the ankle mortise. The tibial cutting block is pinned in place, aiming for a resection that is exactly perpendicular to the mechanical axis of the tibia in the coronal plane, and matching the native posterior slope in the sagittal plane. The tibial resection is typically conservative, removing only 3 to 4 millimeters of bone from the deepest part of the plafond to preserve the dense subchondral bone plate, which is essential for preventing component subsidence.




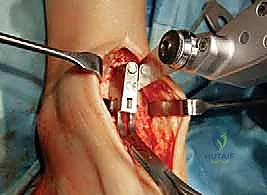
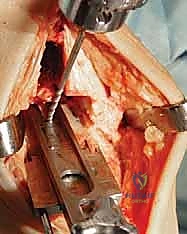
The talar preparation is highly complex and specific to the Mobility design. Utilizing custom jigs referenced off the prepared tibial surface, a series of chamfer cuts are executed on the talar dome. These cuts must perfectly match the internal geometry of the talar component to ensure rigid press-fit fixation. During the lateral and medial talar cuts, the surgeon must remain hyper-vigilant to protect the medial and lateral malleoli. Iatrogenic malleolar fractures are a known complication during this step, often caused by the oscillating saw blade breaching the narrow gutters. Retractor placement and the use of narrow saw blades are critical to mitigating this risk.
Trialing, Soft Tissue Balancing, and Implant Insertion
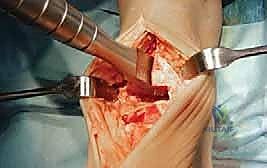
Once the bony preparation is complete, trial components are inserted. The appropriate thickness of the mobile-bearing polyethylene insert is selected to achieve optimal soft-tissue tension. The ankle is taken through a full range of motion under fluoroscopic guidance to assess kinematics, stability, and the absence of impingement. The bearing should glide smoothly without liftoff or subluxation. If the joint remains too tight in dorsiflexion, a fractional lengthening of the Achilles tendon or a gastrocnemius recession may be indicated. If there is coronal plane instability, further ligamentous balancing or a thicker polyethylene insert may be required.



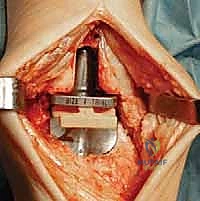
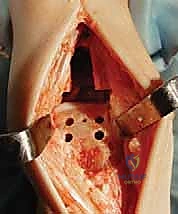
After satisfactory trialing, the definitive components are implanted. The Mobility TAA components are typically designed for uncemented, biological fixation, relying on a porous titanium coating to promote osteointegration. The tibial tray is impacted into place, ensuring flush seating against the resected plafond. The talar component is similarly impacted, achieving a rigid interference fit. Finally, the definitive highly cross-linked polyethylene mobile bearing is inserted. A final fluoroscopic check confirms component seating and alignment. The wound is then closed in multiple layers over a closed-suction drain, paying fastidious attention to the extensor retinaculum and the subcutaneous tissue to ensure a watertight, tension-free closure.



Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, Total Ankle Arthroplasty carries a distinct and challenging complication profile. Intraoperative complications are predominantly mechanical. Iatrogenic fractures of the medial or lateral malleolus occur in approximately 2% to 5% of cases, usually during the execution of the tibial or talar saw cuts within the narrow mortise. If recognized intraoperatively, these fractures must be immediately stabilized with lag screws or tension band constructs to prevent postoperative displacement and mortise widening. Syndesmotic injury is another critical intraoperative risk; over-resection of the lateral tibia can compromise the AITFL. If syndesmotic instability is detected, rigid fixation with syndesmotic screws or suture-button constructs is mandatory prior to closure.