The Salto and Salto-Talaris Total Ankle Arthroplasty: An Intraoperative Masterclass

Key Takeaway
This masterclass provides an immersive, step-by-step guide to Salto and Salto-Talaris Total Ankle Arthroplasty. Fellows will gain granular insights into preoperative planning, meticulous surgical execution, critical anatomical considerations, and advanced complication management. Emphasis is placed on restoring natural kinematics and achieving robust implant fixation for superior patient outcomes in end-stage ankle arthritis.
Comprehensive Introduction and Patho-Epidemiology
The advent and continuous refinement of total ankle arthroplasty (TAA) have revolutionized the management of end-stage tibiotalar arthritis, transitioning the paradigm from joint-sacrificing arthrodesis to joint-preserving arthroplasty. The Salto Total Ankle Prosthesis and its fixed-bearing counterpart, the Salto-Talaris, represent a pinnacle in this evolutionary trajectory. Developed conceptually between 1994 and 1996 and introduced into clinical practice in 1997, the Salto system was meticulously engineered to address the high failure rates of first- and second-generation implants. By prioritizing the restoration of near-normal joint kinematics and robust secondary biological fixation, these third-generation, cementless designs have demonstrated exceptional long-term survivorship and functional outcomes, making them a cornerstone in the armamentarium of the modern foot and ankle surgeon.

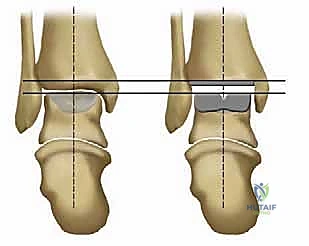
The fundamental philosophy underlying the Salto system is the anatomical resurfacing of the tibiotalar joint. Unlike earlier constrained or highly conforming designs that transmitted excessive shear forces to the bone-implant interface, the Salto system utilizes a semi-constrained approach. The original Salto prosthesis employs a mobile-bearing ultra-high-molecular-weight polyethylene (UHMWPE) insert, which allows for multi-directional self-alignment and reduces edge loading. However, extensive clinical and fluoroscopic evaluation revealed that the highly anatomical design of the talar component—specifically its "cone of revolution" geometry—inherently guides the kinematics of the ankle. This realization led to the development of the Salto-Talaris, a fixed-bearing variant that captures the polyethylene insert within the tibial tray. Dynamic standing views have confirmed that the precise bone cuts and anatomic talar design of the Salto-Talaris negate the absolute necessity for a mobile bearing, effectively minimizing postoperative polyethylene motion during flexion-extension while retaining excellent clinical function.

Understanding the pathogenesis of ankle arthritis is critical for appropriate patient selection and preoperative planning. Osteoarthritis (OA) of the ankle is predominantly post-traumatic, distinct from the primary degenerative etiology typically seen in the hip and knee. Sequelae of malleolar fractures, tibial pilon fractures, and chronic lateral ankle instability account for the vast majority of cases. These traumatic events alter the articular congruity and ligamentous stability of the ankle mortise, leading to asymmetrical loading, focal cartilage degradation, and the eventual development of diffuse osteoarthritis. Less commonly, we encounter end-stage erosive changes secondary to conditions such as synovial osteochondromatosis, pigmented villonodular synovitis (PVNS), hemochromatosis, or untreated osteochondritis dissecans.

Conversely, rheumatoid arthritis (RA) presents a systemic, inflammatory destruction of the joint. Ankle involvement in RA is typically a late manifestation, often presenting after a mean disease duration of nearly two decades. The tibiotalar joint is rarely affected in isolation; concurrent subtalar, transverse tarsal, and forefoot deformities are the norm. The inflammatory pannus erodes cartilage and subchondral bone, leading to profound joint space narrowing, periarticular osteopenia, and severe ligamentous attenuation. The natural history of progressive ankle arthritis, regardless of etiology, involves increasing stiffness, loss of dorsiflexion due to anterior osteophyte formation, and compensatory alterations in gait. As the disease progresses, patients frequently develop an equinus contracture, posterior capsular adhesions, and profound functional disability, necessitating definitive surgical intervention when conservative measures fail.

Detailed Surgical Anatomy and Biomechanics
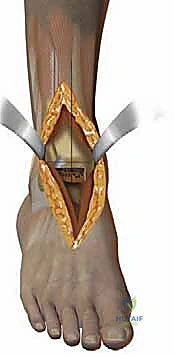
A profound mastery of the surgical anatomy of the anterior ankle is non-negotiable for the safe and effective execution of a Salto or Salto-Talaris total ankle arthroplasty. The operative corridor is densely packed with critical neurovascular structures that must be meticulously identified and protected. The anterior approach utilizes the internervous and intermuscular plane between the tibialis anterior (TA) tendon medially and the extensor hallucis longus (EHL) tendon laterally. This specific interval provides direct, extensile access to the anterior capsule of the tibiotalar joint while minimizing the risk of denervation to the anterior compartment musculature.

The primary neurovascular bundle at risk during this approach is the deep peroneal nerve and the anterior tibial artery. These structures course deep to the extensor retinaculum, typically lying lateral to the anterior tibial artery and medial to the EHL tendon in the proximal aspect of the exposure, before crossing to lie between the EHL and the extensor digitorum longus (EDL) distally. Iatrogenic injury to the deep peroneal nerve can result in a devastating foot drop or localized sensory deficits in the first dorsal web space. Similarly, compromise of the anterior tibial artery, which continues distally as the dorsalis pedis artery, can threaten the vascularity of the dorsal foot, particularly in patients with pre-existing peripheral arterial disease. Retraction must be precise, utilizing blunt Hohmann retractors placed carefully within the joint capsule to shield these anterior structures from the oscillating saw and other instrumentation.

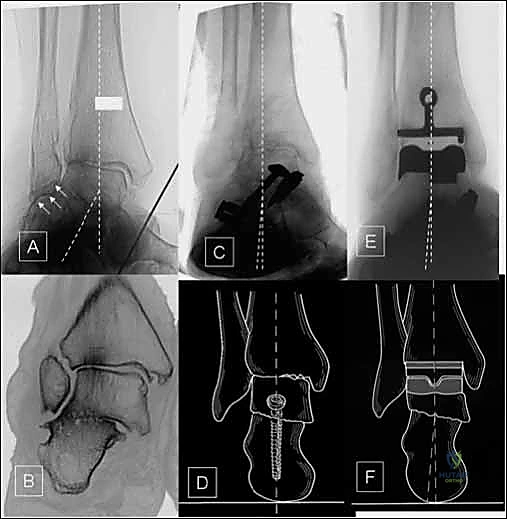
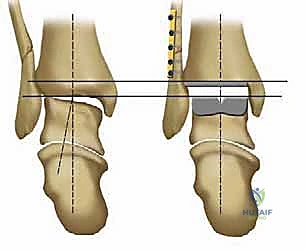
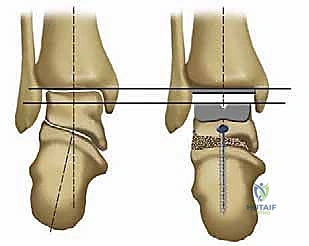
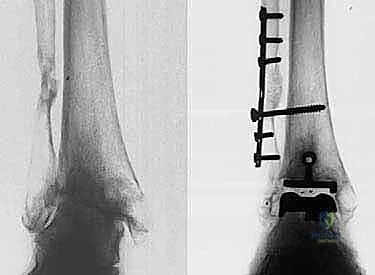
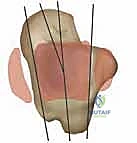
Osteologically, the success of the Salto system relies heavily on its biomechanical interaction with the distal tibia and the talus. The tibial component is designed to resurface the distal tibial plafond while preserving the integrity of the medial and lateral malleoli, which are essential for maintaining the stability of the ankle mortise. A critical design feature of the Salto tibial component is its 3-mm medial rim. This rim acts as a physical barrier, preventing the UHMWPE insert from impinging against the articular surface of the medial malleolus, thereby reducing the risk of edge loading, accelerated polyethylene wear, and secondary osteolysis. Primary fixation of the tibial tray is achieved through a precise interference fit, augmented by an anterior-posterior (AP) keel and a tapered cylindrical plug that engages the dense cancellous bone of the distal tibial metaphysis.

The biomechanical brilliance of the Salto system is most evident in its talar component. Rather than a simple cylinder, the talar implant is modeled as a segment of a "cone of revolution." This geometry faithfully replicates the complex, asymmetrical anatomy of the native talar dome, which is broader anteriorly than posteriorly and features a lateral condyle with a larger radius of curvature than the medial condyle. This conical design ensures that the axis of flexion and extension remains anatomically correct, minimizing shear forces at the bone-implant interface. The lateral aspect of the talar component is also anatomically resurfaced to articulate seamlessly with the lateral malleolus. Stability of this component is secured via three precise, multi-planar bone cuts and the insertion of a robust, 11-mm-diameter hollow fixation peg deep into the vascularized body of the talus, promoting rapid secondary osseointegration.
Ligamentous Balancing and Kinematics
The ankle is not a simple hinge joint; its kinematics are dictated by the complex interplay between the articular geometry and the surrounding ligamentous envelope. The anterior tibiofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the robust medial deltoid ligament complex must be carefully evaluated. In the arthritic ankle, these structures are often contracted, scarred, or attenuated due to chronic deformity. Achieving a balanced ankle mortise intraoperatively is paramount. The Salto system's ability to accommodate up to 4 degrees of varus and valgus tilt within the coronal plane provides a degree of forgiveness, but it does not obviate the need for meticulous soft-tissue balancing. Failure to achieve a plantigrade, balanced foot will inevitably lead to asymmetrical loading, accelerated polyethylene wear, and premature catastrophic failure of the arthroplasty.

Exhaustive Indications and Contraindications
Patient selection is arguably the most critical determinant of long-term success in total ankle arthroplasty. The ideal candidate for a Salto or Salto-Talaris TAA is an older, lower-demand patient with end-stage osteoarthritis, post-traumatic arthritis, or inflammatory arthropathy who experiences severe, daily pain that is refractory to comprehensive non-operative management. Patients must have adequate bone stock to support the implants, a functional soft-tissue envelope, and an intact neurovascular status. We frequently encounter patients who have exhausted conservative modalities, including custom ankle-foot orthoses (AFOs), rocker-bottom shoe modifications, intra-articular corticosteroid or hyaluronic acid injections, and activity modification.
Contraindications to TAA must be strictly respected to avoid devastating complications. Absolute contraindications include active or recent deep infection of the ankle joint, severe peripheral neuropathy (such as Charcot neuroarthropathy), inadequate vascular supply, and massive avascular necrosis (AVN) involving more than 50% of the talar body. In cases of extensive talar AVN, the structural integrity of the bone is insufficient to support the talar component's fixation peg, leading to inevitable subsidence and catastrophic failure. Furthermore, absent or non-functional motor control of the foot and ankle, which cannot be reconstructed via tendon transfers, precludes the use of a mobile or semi-constrained prosthesis.
Relative contraindications require careful, individualized assessment. Young age (typically under 50 years) and high physical demand (e.g., heavy manual labor, high-impact sports) are significant relative contraindications, as the increased cyclical loading will accelerate polyethylene wear and aseptic loosening. Severe coronal plane malalignment (varus or valgus deformity greater than 15-20 degrees) is also a relative contraindication unless it can be definitively corrected either via concurrent or staged extra-articular osteotomies and ligamentous reconstructions. Osteoporosis, while challenging, is not an absolute contraindication but necessitates meticulous surgical technique to prevent intraoperative fractures and may delay the onset of full weight-bearing postoperatively.
| Category | Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Pathology | End-stage primary OA, Post-traumatic OA, Rheumatoid Arthritis, PVNS, Hemochromatosis | Active/recent joint infection, Charcot neuroarthropathy, AVN > 50% of talar body | Severe osteoporosis, AVN < 50% of talar body |
| Patient Factors | Refractory daily pain, failed conservative management, low-to-moderate physical demand | Inadequate vascularity, absent motor function, severe non-correctable malalignment | Age < 50 years, heavy manual laborer, high-impact athletic participation |
| Deformity | Neutral alignment, or correctable varus/valgus < 15 degrees | Rigid, uncorrectable hindfoot or midfoot deformity | Varus/valgus deformity > 15 degrees requiring extensive concurrent osteotomies |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the foundation of a flawlessly executed Salto TAA. The clinical assessment must extend beyond the ankle joint to include a comprehensive evaluation of the entire ipsilateral lower extremity. We must meticulously assess the alignment of the hip and knee, as proximal malalignment will inevitably alter the mechanical axis passing through the ankle, potentially leading to premature implant failure. Gait analysis is crucial; observing the patient for an equinus thrust, external rotation compensation, or dynamic instability provides vital clues regarding soft-tissue contractures that must be addressed intraoperatively. Furthermore, the vascular status must be confirmed via palpable pulses or non-invasive arterial studies, and the integrity of the soft-tissue envelope must be scrutinized for prior surgical scars that might dictate our incisional approach.

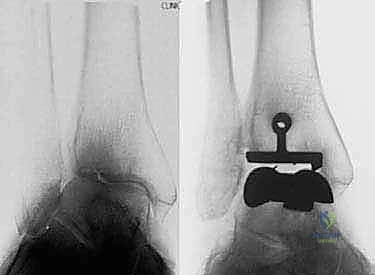
Radiographic evaluation requires high-quality, weight-bearing imaging. Standard weight-bearing anteroposterior (AP), lateral, and mortise views of the ankle are mandatory. A weight-bearing hindfoot alignment view (Saltzman view) is indispensable for quantifying coronal plane deformities of the subtalar joint and hindfoot complex. In cases of significant post-traumatic deformity, previous hardware, or suspected talar avascular necrosis, a fine-cut computed tomography (CT) scan is highly recommended to assess bone stock, delineate cystic changes, and plan for potential bone grafting. The CT scan is particularly useful for evaluating the true volume of the talar body available for the fixation peg of the Salto talar component.

Digital or acetate templating is a critical step that should never be bypassed. Templating on the lateral radiograph allows us to estimate the appropriate size of the talar component, aiming to restore the anatomic center of rotation without overstuffing the anterior or posterior gutters. The tibial component is templated on the AP radiograph to ensure maximal cortical coverage without overhang, which could impinge upon the medial or lateral malleolus. A strict rule of the Salto system must be adhered to: the mobile bearing or fixed insert size must precisely match the talar component, and the talar component should be equal to, or exactly one size smaller than, the tibial component. Reversing this size relationship will result in edge loading and catastrophic failure.

Patient positioning in the operating theater must be optimized for both surgical access and fluoroscopic visualization. The patient is placed supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the leg until the patella is pointing directly towards the ceiling, ensuring that the ankle mortise is positioned neutrally in the coronal plane. A well-padded thigh tourniquet is applied. The foot is positioned at the very edge of the table to allow for unrestricted manipulation, including hyper-plantarflexion, which is necessary for talar preparation. The fluoroscopy unit (C-arm) must be positioned to easily obtain true AP and lateral views without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
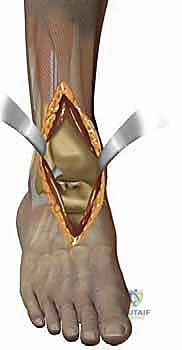
The procedure commences with a longitudinal anterior incision, typically measuring 12 to 15 centimeters, centered directly over the ankle joint. The incision extends from the distal third of the tibia to the talonavicular joint. Meticulous hemostasis is maintained using bipolar electrocautery to preserve the delicate subcutaneous vascular plexus. The superficial peroneal nerve branches, which frequently cross the surgical field distally, must be identified and gently mobilized laterally. The extensor retinaculum is incised longitudinally, and we develop the interval between the tibialis anterior (TA) tendon medially and the extensor hallucis longus (EHL) tendon laterally. The deep neurovascular bundle is identified, mobilized, and protected behind the lateral retractor alongside the EHL and EDL tendons.

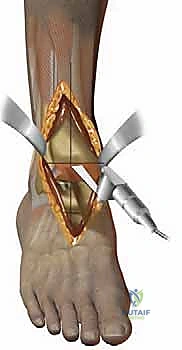
Once the anterior capsule is exposed, a generous capsulotomy is performed. Anterior osteophytes extending from the distal tibia and the talar neck are aggressively resected using a combination of rongeurs and an oscillating saw. This crucial step not only improves exposure but also begins the process of restoring dorsiflexion by removing mechanical blocks. The medial and lateral gutters are carefully cleared of osteophytes and fibrotic tissue, taking extreme care not to violate the articular cartilage of the medial or lateral malleolus. A specialized alignment guide is then pinned to the anterior crest of the tibia, referencing the mechanical axis of the tibia in both the coronal and sagittal planes.
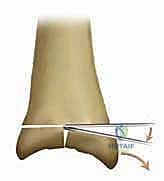
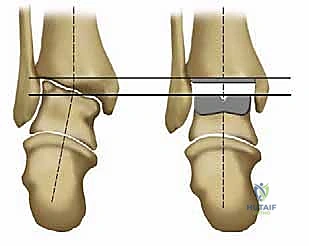
The tibial resection is a highly technically demanding step. The cutting block is positioned to resect a minimal amount of bone—typically just enough to create a flat, bleeding surface of dense cancellous bone. The cut must be strictly perpendicular to the mechanical axis in the coronal plane and incorporate a slight posterior slope (typically 3 to 4 degrees) in the sagittal plane, matching the native anatomy. The oscillating saw is used with precise, controlled strokes. It is imperative to stop the saw blade just short of the medial and lateral malleoli to prevent iatrogenic fractures. The corners of the cut are completed using small osteotomes. The resected tibial plafond is then removed en bloc.

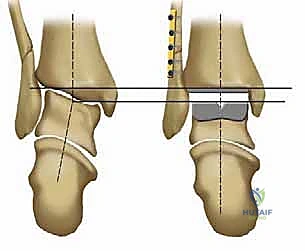
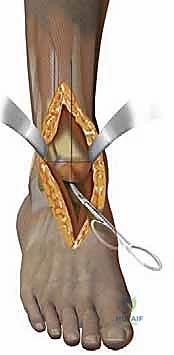
Attention is then directed to the talus. The talar preparation in the Salto system is unique due to its "cone of revolution" geometry. A specialized talar cutting guide is secured, referencing the previously cut tibial surface to ensure perfectly parallel joint spaces in extension. Three distinct cuts are made on the talar dome: a superior horizontal cut, an anterior chamfer cut, and a posterior chamfer cut. The foot is maximally plantarflexed to facilitate the posterior cut, ensuring the neurovascular structures posterior to the ankle remain safely out of harm's way. Following the planar cuts, a central hole is drilled and broached into the body of the talus to accommodate the 11-mm hollow fixation peg of the final implant.

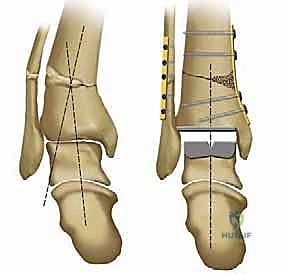
With the bone preparation complete, trial components are inserted. This is a critical phase for assessing soft-tissue balance, joint stability, and range of motion. The ankle is taken through a full arc of flexion and extension. We assess for any impingement in the gutters, ensuring the 3-mm medial rim of the tibial component adequately protects the medial malleolus. Varus or valgus instability is evaluated; if a tight Achilles tendon restricts dorsiflexion to less than 5 degrees past neutral, a percutaneous or open Achilles tendon lengthening (tendo-Achilles lengthening, TAL) or gastrocnemius recession is performed. Once optimal sizing, alignment, and balancing are confirmed both clinically and fluoroscopically, the definitive implants are impacted into place.