Chronic Ankle Arthritis: A Detailed Clinical Case Study & Diagnostic Approach
Key Takeaway
Severe chronic ankle arthritis diagnosis involves patient history noting chronic pain and painful plantarflexion. Clinical exam reveals restricted range of motion. Weight-bearing radiographs confirm significant tibiotalar joint space narrowing, subchondral sclerosis, and prominent osteophytes, particularly posterior, which correlate with symptoms and guide treatment.
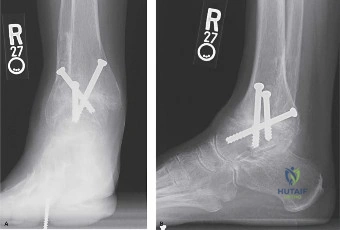
A 62-year-old male presents with chronic, progressive left ankle pain. He has a history of a severe sprain 15 years ago. He now suffers from constant pain, inability to negotiate stairs, and night pain. On examination, he has a rigid ankle with minimal ROM and a mechanical block to dorsiflexion. Please interpret the provided weight-bearing radiographs.

Candidate: These radiographs show end-stage ankle osteoarthritis. There is significant joint space narrowing, subchondral sclerosis, and large marginal osteophytes, particularly at the anterior tibial lip and talar neck. There is no major coronal plane deformity visible on the mortise view.
Describing findings randomly without a system. Failing to correlate the radiographic findings (like the anterior osteophytes) with the patient's clinical complaint of limited dorsiflexion. Forgetting to mention the integrity of the mortise or the status of the subtalar joint space.
Start with a summary statement: "These are weight-bearing radiographs of the left ankle demonstrating end-stage post-traumatic tibiotalar osteoarthritis." Follow a structured approach: 1. Joint Space: Global narrowing with subchondral sclerosis. 2. Osseous morphology: Large anterior and posterior osteophytes causing a mechanical block to ROM. 3. Alignment: Mortise is congruent with no significant coronal deformity (e.g., Takakura Stage 3B). 4. Adjacent joints: Apparent maintenance of the subtalar joint space, which requires confirmation on CT.
The patient's CT scan is shown below. Given the findings, discuss your surgical decision-making process for this 62-year-old patient. Would you offer him an arthroplasty or an arthrodesis?

Candidate: While the patient is 62, his high functional demand and the presence of significant subchondral cysts make arthrodesis the preferred option. Arthroplasty might struggle with bone stock deficiency. I would perform an isolated tibiotalar arthrodesis as the subtalar joint is clinically and radiologically spared.
Being dogmatic. Simply saying "I would do a fusion" without justifying it through the patient's demand, bone stock (cysts), and the status of the subtalar joint. Forgetting that a "failed" arthroplasty is far more difficult to revise than a primary arthrodesis.
Structured decision-making: 1. Patient Factors: High-demand supervisory role/recreational goals. 2. Morphological Factors: Significant subchondral cysts visible on CT, complicating implant fixation. 3. Joint Factors: Isolated tibiotalar pathology, as confirmed by diagnostic injection. Conclusion: Proceed with an anterior tibiotalar arthrodesis, noting that while TAA is an option for older patients, the bone stock and activity requirements in this case favor the durability of fusion.
You are in theater performing the arthrodesis. Describe your technical goals for the position of the fusion to ensure a functional gait.
Candidate: The goal is to fuse in neutral dorsiflexion, 5 degrees of hindfoot valgus, and 5-10 degrees of external rotation. I would also aim for slight posterior translation of the talus to shorten the lever arm.
Missing the sagittal plane alignment. Candidates often forget to mention that fusion in plantarflexion (equinus) is a major complication that leads to a "vaulting" gait and subsequent knee recurvatum.
Clearly state the targets: Sagittal: Neutral to 2° dorsiflexion (avoid equinus at all costs). Coronal: 5° valgus. Axial: 5–10° external rotation to match the patient's normal tibial torsion. Translation: Posterior translation of the talus to decrease the anterior lever arm. Emphasize that these are confirmed fluoroscopically and are essential to avoid adjacent joint overload in the midfoot.
