Masterclass: Percutaneous & Intramedullary Reduction for Pediatric Radial Neck Fractures

Key Takeaway
Welcome, fellows, to an in-depth masterclass on managing pediatric radial neck fractures using percutaneous joystick and intramedullary Metaizeau techniques. We'll meticulously cover comprehensive anatomy, precise preoperative planning, and granular intraoperative execution. This session emphasizes critical decision-making, neurovascular protection, and advanced reduction maneuvers to achieve optimal outcomes and prevent complications in these challenging injuries.
Comprehensive Introduction and Patho-Epidemiology
Welcome, esteemed colleagues, fellows, and residents, to this definitive masterclass on the surgical management of pediatric radial neck fractures. Today, we are tackling a fascinating, nuanced, and often challenging injury in pediatric orthopaedic trauma: the displaced radial neck fracture. These injuries are typically transphyseal, meaning the fracture line propagates across the delicate growth plate. Interestingly, they rarely involve the radial head epiphysis itself, distinguishing them from the intra-articular radial head fractures more commonly seen in our adult patient population. The vast majority of the fractures we encounter in this demographic are Salter-Harris type II injuries, characterized by a metaphyseal Thurston-Holland fragment. However, Salter-Harris type I fractures are also frequently observed, particularly in younger children whose physes are entirely cartilaginous and less radiographically apparent. In our older pediatric and adolescent patients approaching skeletal maturity, we transition to seeing purely metaphyseal fractures. Understanding these distinct morphological variations is not merely an academic exercise; it is the foundational prerequisite for formulating a successful, individualized surgical approach.

Exhibit: A classic Salter-Harris type II radial neck fracture. Note the distinct displacement of the proximal radial metaphysis relative to the epiphysis, a hallmark of this injury pattern.

Exhibit: A Salter-Harris type I fracture. The fracture line runs purely through the radiolucent physis, making it more subtle on initial radiographic evaluation without careful scrutiny of the radiocapitellar alignment.
Epidemiologically, radial neck fractures represent a substantial clinical burden, accounting for approximately 14% of all pediatric elbow fractures. They most frequently occur in children between the ages of 9 and 12 years, a period characterized by rapid skeletal growth and increased participation in high-energy activities. The typical mechanism of injury is a fall on an outstretched hand (FOOSH) with the elbow in full extension and the forearm in supination. This specific posture transmits a violent valgus thrust across the elbow joint, forcefully driving the radial head against the dense, ossified capitellum. Because the pediatric collateral ligaments are often stronger than the adjacent open physis, the radial neck fails under this immense compressive and shear load. The resulting displacement is typically a combination of lateral translation and valgus angulation, though complex multi-planar deformities are not uncommon.
Precision, meticulous pre-operative planning, and exceptionally gentle soft-tissue handling are paramount when managing these injuries. The pediatric proximal radius possesses a surprisingly limited capacity for spontaneous remodeling compared to the distal radius or proximal humerus. This is largely due to the complex, multi-axial kinematics of the radiocapitellar and proximal radioulnar joints. Even moderate residual angulation can lead to cam-effect impingement during forearm rotation, resulting in a permanent, debilitating loss of pronation and supination. Furthermore, aggressive open reduction techniques carry an unacceptably high risk of catastrophic complications, including avascular necrosis (AVN) of the radial head and proximal radioulnar synostosis. Therefore, mastering closed, percutaneous, and intramedullary reduction techniques—specifically the Metaizeau technique—is an absolute necessity for the modern pediatric orthopaedic surgeon.
Detailed Surgical Anatomy and Biomechanics
Before we even consider bringing a scalpel to skin or a wire to bone, a comprehensive, three-dimensional understanding of the regional anatomy is non-negotiable. The proximal radial epiphysis, which ultimately forms the articular concavity of the radial head, typically begins to ossify by 4 years of age and slowly assumes its mature, discoid shape. Crucially, the proximal radial physis—the primary longitudinal growth center for the proximal radius—remains open and active until approximately 14 years of age in girls and 17 years in boys. This physis is the epicenter of our surgical concern. Iatrogenic disruption, either from multiple aggressive passes of a Kirschner wire or from forceful open reduction, can precipitate premature physeal closure. The radial neck itself is the constricted, cylindrical portion immediately distal to the head and physis, serving as the critical lever arm connecting the articular surface to the radial diaphysis. It articulates intimately with the capitellum of the humerus and the radial notch of the ulna, forming a highly constrained joint complex essential for fluid forearm rotation.

The vascular anatomy of the proximal radius is precarious and dictates our surgical philosophy. The radial head is almost entirely intra-articular and covered by hyaline cartilage, meaning it possesses no direct soft-tissue attachments to provide collateral blood flow. Its entire vascular supply is retrograde, derived from intraosseous vessels ascending through the radial neck and from a delicate periosteal plexus fed by the recurrent radial artery. A displaced fracture of the radial neck violently disrupts the intraosseous supply. If the surgeon then performs an extensive open approach, stripping the remaining periosteal hinges in an attempt to achieve perfect anatomical reduction, the radial head is effectively rendered avascular. This profound ischemic insult is the primary genesis of post-operative avascular necrosis, a devastating complication that can lead to head collapse, severe pain, and permanent joint destruction.
The most critical neurovascular structure we must obsessively protect during any intervention on the proximal radius is the posterior interosseous nerve (PIN). As a terminal motor branch of the radial nerve, the PIN bifurcates at the level of the radiocapitellar joint. It then dives deep into the substance of the supinator muscle, winding a perilous course around the anterolateral and posterior aspects of the radial neck. It enters the supinator through a fibrous arch known as the Arcade of Frohse. The PIN is uniquely vulnerable during percutaneous pin insertion from the lateral or anterolateral approach, or during the deep dissection of a Kocher approach. To mitigate this risk, pronation of the forearm is our primary protective maneuver. When the forearm is fully pronated, the supinator muscle contracts and tightens, physically drawing the PIN medially and posteriorly, pulling it away from the anterolateral danger zone of the radial neck. This anatomical reality dictates that all percutaneous joysticks or stabilizing wires must be inserted with the forearm in maximum pronation.

Furthermore, when employing the Metaizeau intramedullary nailing technique, we must master the anatomy of the distal radius to establish a safe entry point. Here, the superficial radial nerve (SRN) is our primary concern. The SRN is a sensory nerve coursing along the radial border of the forearm, providing critical sensation to the dorsum of the hand and the radial digits. Distal radial incisions must be meticulously planned and executed with blunt dissection down to the periosteum to avoid transecting SRN branches, which can result in agonizing, recalcitrant neuromas. The muscular intervals also guide our distal approach. We typically target the interval between the first extensor compartment (abductor pollicis longus and extensor pollicis brevis) and the second compartment (extensor carpi radialis longus and brevis) for a lateral entry, or between the third and fourth compartments for a dorsal entry, ensuring we stay proximal to the distal radial physis to avoid iatrogenic growth arrest at the wrist.
Exhaustive Indications and Contraindications
The decision-making process for pediatric radial neck fractures hinges on a delicate balance between the patient's remaining growth potential, the degree of initial displacement, and the inherent risks of surgical intervention. The Judet classification system remains the most practical and widely adopted framework for categorizing these injuries and guiding our treatment algorithms. Judet Type 1 fractures are undisplaced or exhibit only a minimal horizontal shift. Type 2 fractures demonstrate angulation of less than 30 degrees. Type 3 fractures are angulated between 30 and 60 degrees. Type 4a fractures are severely angulated between 60 and 80 degrees, while Type 4b fractures are displaced greater than 80 degrees, often completely off the metaphyseal stump.

The limits of acceptable angulation are a subject of ongoing debate, but a general consensus exists. In younger children (under 10 years of age), angulation of up to 30 degrees and translation of up to 50% can generally be accepted, as the robust remodeling potential of the growing skeleton will likely correct this deformity over time without functional deficit. However, in children over 10 years of age, or in any patient with angulation exceeding 30 degrees, the risk of permanent cam-impingement and loss of forearm rotation rises exponentially. Therefore, Judet Type 3 and Type 4 fractures are absolute indications for reduction. The primary goal is to restore radiocapitellar alignment to within 20 degrees of perfect anatomical position.
It is crucial to understand that open reduction is viewed as a salvage procedure, not a primary option. The indications for open reduction are strictly limited to cases where closed manipulation, percutaneous leverage, and intramedullary techniques have completely failed, or in the rare instance of an irreducible fracture due to soft-tissue interposition (such as the annular ligament or joint capsule becoming incarcerated in the fracture site). Contraindications to percutaneous or intramedullary techniques include active local infection, severe open fractures with massive contamination (where external fixation may be preferred), or delayed presentations (greater than 7-10 days) where early callus formation renders closed manipulation impossible without excessive, damaging force.
| Surgical Technique | Primary Indications | Relative Contraindications | Absolute Contraindications |
|---|---|---|---|
| Closed Reduction | Judet Type 2 & 3 (< 45° angulation), acute presentation (< 3 days). | Swelling precluding safe manipulation, older adolescents. | Open fractures, associated vascular compromise. |
| Percutaneous Joystick | Judet Type 3 & 4 failing closed reduction, translation > 50%. | Comminuted metaphyseal beak, delayed presentation. | Active local infection, uncooperative patient (if done under local). |
| Intramedullary Nail (Metaizeau) | Judet Type 3 & 4, unstable after closed reduction, multi-trauma. | Extremely distal or diaphyseal extension of fracture. | Distal radius physis injury precluding entry point. |
| Open Reduction | Irreducible by all closed/percutaneous means, incarcerated tissue. | Any fracture amenable to closed/percutaneous methods. | High risk of AVN accepted; active joint infection. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative evaluation begins with high-quality, orthogonal radiographic imaging. Standard anteroposterior (AP) and lateral views of the elbow are mandatory. Oblique views, particularly the radiocapitellar view (obtained with the beam angled 45 degrees cephalad), can be invaluable for delineating the exact degree of angulation and translation, especially in complex, multi-planar deformities. We must meticulously scrutinize these images to confirm the orientation of the displaced radial head. In rare, high-energy injuries, the articular surface of the fragment can flip 180 degrees, a scenario that almost always necessitates open reduction.

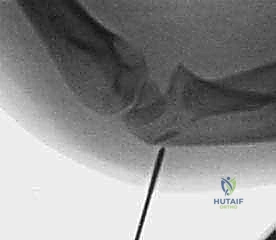
Exhibit: Initial AP radiograph demonstrating an elbow dislocation. The radial head is completely displaced from its articulation with the capitellum.

Exhibit: The corresponding lateral view of the elbow dislocation. Notice the severe posterior displacement of the radius and ulna relative to the distal humerus.
A critical aspect of pre-operative planning is identifying associated injuries, which occur in up to 30% of radial neck fractures. We must actively rule out fractures of the olecranon, proximal ulna (Monteggia variants), medial epicondyle, and lateral condyle. Furthermore, radial neck fractures are frequently associated with elbow dislocations. A posteriorly displaced radial neck fracture can occur during the spontaneous or manipulative reduction of a posterior elbow dislocation. If the elbow is flexed during the reduction maneuver, the lateral condyle can strike the radial head, shearing it off the metaphysis. This underscores the absolute necessity of obtaining post-reduction radiographs for any elbow dislocation to ensure a radial neck fracture has not been unmasked or iatrogenically displaced.

Exhibit: Post-reduction lateral view. The ulnohumeral joint appears reduced, but the radial head is conspicuously absent from its normal anatomical position.
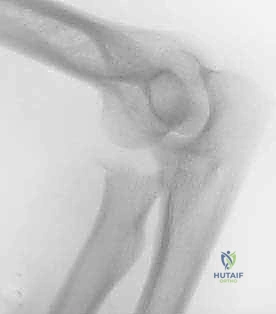
Exhibit: The post-reduction AP view reveals the catastrophic iatrogenic displacement of the radial head, highlighting the dangers of manipulative reduction without recognizing an occult radial neck fracture.
For intramedullary nailing, pre-operative templating is essential. We typically utilize Titanium Elastic Nails (TENs). The diameter of the nail should be approximately 40% to 50% of the narrowest diameter of the radial diaphysis. In most pediatric patients, a 1.5 mm or 2.0 mm nail is appropriate. The nail must be pre-bent at its distal tip (approximately 15 to 20 degrees over the terminal 10 mm) to facilitate steering through the medullary canal and to provide the necessary rotational leverage to reduce the radial head. Patient positioning is equally critical. The patient is placed supine on the operating table with the affected arm extended on a radiolucent hand table. The C-arm fluoroscope must be positioned to allow unobstructed, dynamic AP and lateral views of the entire forearm and elbow without requiring the surgeon to awkwardly manipulate the fractured extremity.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of radial neck fractures is a stepwise progression of escalating invasiveness. We begin with closed reduction maneuvers. The Patterson technique involves applying varus stress to the extended elbow while applying direct digital pressure over the displaced radial head, combined with forceful pronation. The Israeli technique involves flexing the elbow to 90 degrees, maximally supinating the forearm, and applying direct pressure to the radial head while simultaneously pronating the forearm. If these maneuvers yield an acceptable reduction (less than 30 degrees of angulation), the arm is immobilized in a long-arm cast. However, if closed reduction fails or is highly unstable, we immediately proceed to percutaneous or intramedullary techniques.

The percutaneous joystick technique is a powerful tool for manipulating the radial head. Under strict fluoroscopic guidance, a 1.5 mm or 2.0 mm Kirschner wire is introduced percutaneously. Crucially, the forearm must be in maximum pronation to protect the posterior interosseous nerve. The wire is inserted from the direct lateral or posterolateral aspect of the elbow, engaging the displaced radial head fragment. The wire is not driven across the fracture site; rather, it is used as a lever—a joystick—to physically push or rotate the radial head back into alignment with the metaphyseal stump. Once reduced, the fracture can be stabilized by advancing the wire across the fracture site into the medial cortex of the radial diaphysis, or by proceeding to intramedullary nailing.


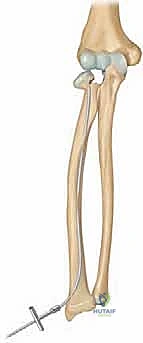
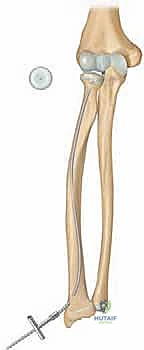
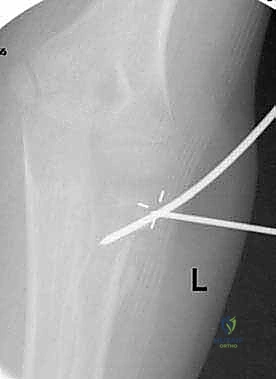
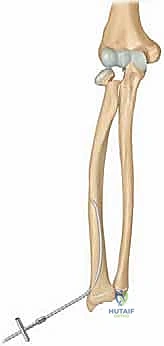
The Metaizeau technique (retrograde intramedullary nailing) is the gold standard for unstable or irreducible pediatric radial neck fractures. A 2 cm longitudinal incision is made over the lateral or dorsal aspect of the distal radius, approximately 2 to 3 cm proximal to the distal radial physis. Blunt dissection protects the superficial radial nerve. The cortex is breached using an awl or drill, creating an entry portal angled proximally. The pre-bent titanium elastic nail is inserted and advanced retrograde up the radial shaft using a T-handle. As the nail approaches the fracture site, the surgeon uses the C-arm to ensure the curved tip is oriented to engage the displaced radial head.

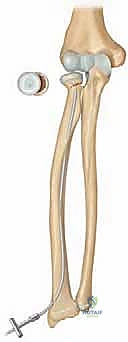
The critical maneuver of the Metaizeau technique occurs once the nail tip crosses the fracture line and purchases the subchondral bone of the radial head epiphysis. The surgeon then forcefully rotates the nail 180 degrees around its longitudinal axis. The pre-bent tip acts as an internal cam, sweeping the displaced radial head back into anatomical alignment with the metaphysis. This reduction is confirmed on orthogonal fluoroscopic views. The nail is then cut beneath the skin at the distal entry site, leaving a small segment protruding to facilitate future removal. This technique provides excellent three-point biomechanical stability, allowing for early mobilization and minimizing the risk of AVN by avoiding any direct dissection around the radial neck.

Additional intraoperative fluoroscopy demonstrating the sequence of nail passage, engagement of the head, and rotational reduction.



Complications, Incidence Rates, and Salvage Management
Despite our best efforts and meticulous surgical technique, complications following pediatric radial neck fractures remain a significant clinical challenge. The incidence of complications is directly proportional to the severity of the initial displacement, the age of the patient, and, most importantly, the invasiveness of the surgical intervention. Open reduction, while sometimes unavoidable, carries the highest complication profile and must be approached with extreme caution. The orthopaedic surgeon must be vigilant in monitoring for these adverse outcomes and be prepared to implement complex salvage procedures when necessary.

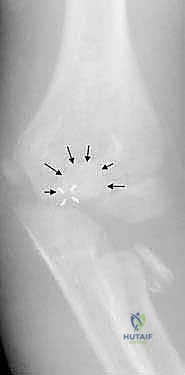
Exhibit: A lateral radiograph demonstrating a radial neck fracture complicated by an associated, minimally displaced intra-articular olecranon fracture. Such associated injuries complicate the rehabilitation protocol and increase the risk of stiffness.

Exhibit: Another example of a complex fracture pattern requiring careful assessment for associated ligamentous or osseous injuries.
Avascular necrosis (AVN) of the radial head is the most devastating complication, occurring in up to 10-20% of cases treated with open reduction, compared to less than 2% in those treated closed or percutaneously. AVN manifests radiographically as sclerosis, fragmentation, and eventual collapse of the radial head, leading to severe pain, crepitus, and profound loss of motion. Management of AVN is notoriously difficult. In the growing child, conservative management with activity modification is initially trialed, as some revascularization and remodeling can occur. However, in severe cases with joint destruction, salvage procedures such as radial head excision (delayed until skeletal maturity if possible to prevent proximal migration of the radius) or complex reconstructive osteotomies may be required.
Proximal radioulnar synostosis is another catastrophic complication, characterized by the formation of a solid bony bridge between the proximal radius and ulna, resulting in an absolute, 0-degree loss of pronation and supination. This occurs when the fracture hematoma communicates with the interosseous membrane, often exacerbated by aggressive surgical dissection or the placement of hardware across the interosseous space. The incidence approaches 10% following open reduction. Treatment requires delayed surgical excision of the synostosis (at least 6-12 months post-injury when the bone scan is cold), combined with the interposition of vascularized fat or synthetic materials to prevent recurrence, a procedure fraught with high failure rates.
| Complication | Estimated Incidence | Primary Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Avascular Necrosis (AVN) | 2% (Closed) to 20% (Open) | Open reduction, severe initial displacement, |
Clinical & Radiographic Imaging Archive