Masterclass: Open Reduction and Internal Fixation of Lateral Tibial Plateau Fractures

Key Takeaway
Welcome, fellows, to an immersive intraoperative masterclass on lateral tibial plateau fracture ORIF. We'll meticulously cover comprehensive anatomy, preoperative planning, and precise, real-time surgical execution. Learn critical techniques for reduction, bone grafting, meniscal repair, and optimal hardware placement. Understand potential pitfalls and strategies for effective postoperative rehabilitation and complication management to ensure superior patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Lateral tibial plateau fractures represent a highly complex and frequently encountered intra-articular injury pattern in orthopedic trauma surgery. These fractures, which fundamentally disrupt the critical weight-bearing surface of the proximal tibia, demand meticulous attention to detail to restore articular congruity, re-establish the mechanical axis of the lower extremity, and ensure enduring knee stability. The overarching objective of operative intervention is not merely fracture union, but rather the prevention or significant delay of post-traumatic osteoarthritis. Because the articular cartilage possesses a remarkably limited intrinsic healing capacity, any residual step-off or gap alters joint contact mechanics, exponentially increasing focal peak stresses and precipitating accelerated chondral degradation.
The patho-epidemiology of lateral tibial plateau fractures is distinctly bimodal, reflecting two divergent mechanisms of injury and patient demographics. In the younger, physiologically robust population, these injuries are typically the consequence of high-energy trauma, such as motor vehicle collisions or falls from significant heights. The application of a massive axial load combined with a valgus vector drives the lateral femoral condyle into the lateral tibial plateau, yielding pure cleavage (split) fractures or complex split-depression patterns (Schatzker Types I and II). Conversely, in the elderly population with diminished bone mineral density, low-energy trauma—such as a simple fall from a standing height—frequently results in pure depression fractures (Schatzker Type III). In these osteoporotic individuals, the relatively dense subchondral bone of the lateral femoral condyle acts as a biological tamp, crushing the weakened cancellous metaphyseal bone of the lateral plateau without necessarily fracturing the robust lateral cortical rim.
The natural history and ultimate prognosis of lateral tibial plateau fractures are inextricably linked to the degree of initial articular depression, the presence of coronal or sagittal plane instability, and the integrity of the surrounding soft tissue envelope. Undisplaced or minimally displaced fractures, particularly those demonstrating clinical stability under varus and valgus stress testing, generally portend a favorable prognosis with conservative management. However, any significant displacement—historically defined as an articular step-off exceeding 2 to 3 millimeters, or condylar widening greater than 5 millimeters—profoundly disrupts normal joint kinematics. When this osseous disruption is compounded by concomitant ligamentous or meniscal insufficiency, the risk of rapid-onset, debilitating post-traumatic arthritis becomes a near certainty without anatomical surgical restoration.
The evolution of treatment for these complex injuries has transitioned significantly over the past few decades. Historically managed with traction and cast bracing, which frequently resulted in stiffness, malunion, and varus/valgus collapse, the contemporary gold standard relies heavily on precise open reduction and internal fixation (ORIF). Modern surgical paradigms emphasize the preservation of the delicate soft tissue envelope through meticulous surgical approaches, the utilization of subchondral rafting techniques to support elevated articular fragments, and the application of anatomically pre-contoured locking plate technology to secure the metadiaphyseal region, thereby allowing for early, aggressive rehabilitation.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the proximal tibial and knee joint anatomy is the absolute prerequisite for successful surgical planning, safe exposure, and optimal implant placement. The tibial plateau is a complex, asymmetric osseous structure comprising the larger, slightly concave medial plateau; the smaller, distinctly convex lateral plateau; and the central, non-articular intercondylar eminence. This eminence is of paramount biomechanical importance, serving as the robust attachment site for the anterior and posterior cruciate ligaments. Clinically and radiographically, it is crucial to recognize that the lateral plateau sits slightly proximal to the medial joint surface, creating a subtle 3-degree varus angle relative to the anatomical axis of the tibial shaft. Furthermore, the entire plateau exhibits a posterior slope averaging approximately 10 degrees, a critical spatial parameter that must be respected and restored during fracture reduction to prevent iatrogenic sagittal plane malalignment.
The biomechanical load distribution across the human knee joint is inherently asymmetric, a physiological reality that dictates the morphological characteristics of the proximal tibia. During the normal gait cycle, the mechanical axis passes slightly medial to the center of the knee. Consequently, the medial plateau bears approximately 60% of the joint's axial load, while the lateral plateau bears only 40%. This chronic eccentric loading stimulates increased trabecular bone formation medially, rendering the medial plateau inherently stronger, denser, and more resistant to fracture. The relative osteopenia of the lateral subchondral bone, coupled with the lower extremity's physiological valgus alignment and its inherent susceptibility to medially directed (valgus-producing) forces, explains the significantly higher incidence of lateral plateau fractures compared to their medial counterparts.
The osseous structures of the plateau are intimately associated with a complex network of soft tissues that are frequently compromised during trauma. Both plateaus are covered by their respective menisci—vital, C-shaped fibrocartilaginous structures that function as primary shock absorbers, distribute axial loads over a broader surface area, and dramatically improve femorotibial joint congruency. The lateral meniscus covers a larger percentage of its respective plateau than the medial meniscus and is more mobile. High-resolution MRI and arthroscopic studies have demonstrated that meniscal tears or peripheral detachments occur in up to 50% of operative tibial plateau fractures. Failure to identify, repair, or appropriately manage these meniscal injuries during ORIF severely compromises joint stability and acts as an independent predictor of poor long-term functional outcomes.
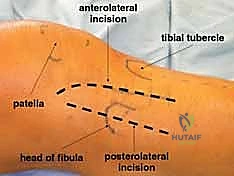
Surgical navigation of the proximal tibia requires precise identification of key bony landmarks and an acute awareness of adjacent neurovascular structures. Gerdy's tubercle, located on the anterolateral aspect of the proximal tibia, serves as the robust insertion point for the iliotibial band and is a primary landmark for the anterolateral surgical approach. Slightly medial and distal lies the tibial tuberosity, the insertion site of the patellar tendon. Posterolaterally, the fibular head provides attachment for the biceps femoris tendon and the lateral collateral ligament. Most critically, the common peroneal nerve courses directly posterior to the biceps tendon, wrapping around the fibular neck before arborizing into its deep and superficial branches. Any surgical dissection, retractor placement, or implant positioning in this posterolateral quadrant demands meticulous, direct visualization and protection of the peroneal nerve to avert devastating iatrogenic foot drop.
Exhaustive Indications and Contraindications
The decision-making algorithm for the operative management of lateral tibial plateau fractures requires a nuanced synthesis of patient-specific factors, local soft tissue conditions, and precise radiographic parameters. While historical thresholds dictated operative intervention for any articular step-off exceeding 2 millimeters, contemporary orthopedic thought recognizes that absolute numerical values must be contextualized within the broader clinical picture, particularly regarding dynamic joint stability.
Operative indications are broadly categorized into absolute and relative parameters. Absolute indications for immediate or staged surgical intervention include open fractures requiring urgent irrigation and debridement, fractures associated with acute compartment syndrome necessitating emergent fasciotomy, and fractures presenting with an associated vascular injury (typically the popliteal artery or its trifurcation branches). Relative, yet strongly compelling, indications for ORIF include articular depression or step-off exceeding 3 millimeters in a healthy, active patient; condylar widening greater than 5 millimeters, which alters the mechanical axis and increases patellofemoral contact pressures; and clinical or fluoroscopic evidence of varus/valgus instability greater than 10 degrees in near-full extension compared to the uninjured contralateral knee. Furthermore, any fracture pattern resulting in a functionally unacceptable mechanical axis deviation mandates surgical realignment.
Conversely, non-operative management is reserved for a highly specific subset of patients and fracture patterns. Truly non-displaced or minimally displaced fractures that demonstrate absolute stability under varus/valgus stress testing can be successfully managed with a hinged knee brace and protected weight-bearing. Additionally, non-operative management may be the most prudent course for non-ambulatory patients, individuals with severe medical comorbidities precluding safe anesthesia, or patients with advanced pre-existing tricompartmental osteoarthritis where a total knee arthroplasty may be the more appropriate definitive, albeit delayed, intervention.
The most critical contraindication to immediate internal fixation is a severely compromised soft tissue envelope. The proximal tibia possesses a notoriously thin and tenuous anteromedial and anterolateral soft tissue covering. Operating through severe fracture blisters, profound edema, or impending tissue necrosis exponentially increases the risk of catastrophic wound dehiscence and deep surgical site infection. In these scenarios, the standard of care dictates a "damage control" approach: immediate application of a joint-spanning external fixator to restore length, alignment, and stability, allowing the soft tissues to declare themselves and recover over 10 to 21 days before definitive ORIF is attempted.
| Clinical Parameter | Operative Indications (ORIF) | Non-Operative / Delayed Indications |
|---|---|---|
| Articular Displacement | Step-off > 3mm; Condylar widening > 5mm | Non-displaced; Step-off < 2mm (stable) |
| Joint Stability | Varus/Valgus instability > 10 degrees | Stable under dynamic stress testing |
| Soft Tissue Status | Intact envelope; Resolved edema (wrinkle sign) | Severe edema; Fracture blisters (Tscherne III); Active infection |
| Associated Injuries | Open fractures; Compartment syndrome; Vascular injury | Isolated injury with acceptable alignment |
| Patient Factors | Young, active, high functional demands | Non-ambulatory; Severe comorbidities; Advanced baseline osteoarthritis |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful tibial plateau fracture management. The process begins with a meticulous clinical assessment, prioritizing the neurovascular examination. The proximity of the popliteal artery and the common peroneal nerve to the proximal tibia makes them highly vulnerable to traction or direct trauma during the initial injury. A baseline Ankle-Brachial Index (ABI) should be obtained; an ABI of less than 0.9 mandates further vascular investigation, typically a CT angiogram. Furthermore, the surgeon must maintain a high index of suspicion for acute compartment syndrome. The rigid fascial compartments of the leg can rapidly accumulate hemorrhage and edema from the highly vascular metaphyseal bone. Clinical signs such as pain out of proportion to the injury, pain with passive stretch of the toes, and a tense, "wood-like" feeling of the compartments are ominous. A differential pressure (diastolic blood pressure minus compartment pressure) of less than 30 mm Hg is an absolute indication for emergent four-compartment fasciotomies.
Radiographic evaluation must be exhaustive. Standard plain radiographs, including an anteroposterior (AP) view centered on the knee, a true lateral view, and internal/external oblique views, are mandatory. Crucially, the AP view should be obtained with a 10-degree caudal tilt of the X-ray beam to parallel the native posterior slope of the tibial plateau, thereby providing a true tangential projection of the articular surface. However, plain radiographs notoriously underestimate the degree of articular comminution and depression. Therefore, a fine-cut, three-dimensional Computed Tomography (CT) scan with sagittal and coronal reformats is the absolute gold standard and is considered mandatory for all operative plateau fractures. The CT scan allows the surgeon to precisely map the fracture lines, identify the location and depth of articular depression, and formulate a definitive surgical tactic regarding approach, implant selection, and the necessity for bone graft.
Preoperative templating utilizes the CT data to select the optimal hardware and anticipate intraoperative challenges. The surgeon must determine the trajectory of the subchondral rafting screws required to support the elevated articular fragments. The volume of the metaphyseal void created after articular elevation must be estimated to ensure adequate availability of autograft (typically harvested from the ipsilateral iliac crest), allograft, or synthetic bone substitutes (such as calcium phosphate cement). Templating also dictates the length and contour of the lateral locking plate, ensuring adequate diaphyseal fixation distal to the fracture extent while avoiding impingement on the joint capsule proximally.
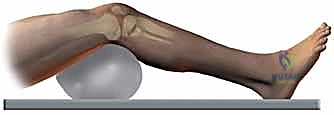
Patient positioning in the operating theater must facilitate unrestricted surgical access and unimpeded fluoroscopic imaging. The patient is placed supine on a completely radiolucent operating table. The contralateral, uninjured leg is typically placed in a well-padded leg carrier or hemilithotomy position; this is critical as it allows the C-arm fluoroscopy unit to be brought in from the contralateral side, providing orthogonal views of the injured knee without requiring awkward manipulation of the fractured extremity. A bump is placed under the ipsilateral hip to correct the natural external rotation of the lower limb, bringing the patella to a perfectly anterior-facing position.
A sterile, radiolucent bolster or triangle is placed beneath the injured knee to maintain approximately 30 degrees of flexion. This specific degree of flexion is highly advantageous; it relaxes the gastrocnemius muscle posteriorly, reduces tension on the iliotibial band and lateral collateral ligament, and significantly facilitates the mobilization and reduction of the lateral plateau fracture fragments. A pneumatic tourniquet is applied to the proximal thigh to ensure a bloodless surgical field, which is essential for the meticulous inspection of the intra-articular pathology. Finally, if autologous bone grafting is anticipated, the ipsilateral anterior superior iliac spine and iliac crest are prepped and draped into the sterile field simultaneously.
Step-by-Step Surgical Approach and Fixation Technique
The Anterolateral Approach and Intra-Articular Exposure
The standard workhorse for the vast majority of lateral tibial plateau fractures is the anterolateral approach. This trajectory provides expansive exposure of the lateral articular surface and the proximal anterolateral metaphysis while allowing for excellent soft tissue coverage over the definitive hardware. The incision is typically a "hockey-stick" or gently curved longitudinal incision. It originates 2 to 3 centimeters proximal to the joint line, just anterior to the lateral femoral epicondyle, curves distally over Gerdy's tubercle, and extends longitudinally down the anterolateral aspect of the tibial crest. This specific placement ensures that the surgical incision does not lie directly over the eventual plate, thereby minimizing the risk of wound breakdown and hardware exposure.
Following sharp dissection through the skin and subcutaneous tissues, full-thickness fasciocutaneous flaps are meticulously developed to preserve the precarious blood supply to the skin. The deep fascia is encountered, and the iliotibial band is split longitudinally in line with its fibers. Distal to Gerdy's tubercle, the fascia overlying the anterior compartment is incised. Utilizing a Cobb elevator, the tibialis anterior muscle is sharply elevated off the proximal lateral tibia in a strict subperiosteal plane, working from anterior to posterior.
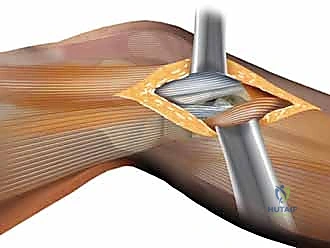
This elevation exposes the lateral joint capsule and the metaphyseal fracture lines. To gain access to the articular surface, a submeniscal arthrotomy is performed. The coronary ligament—the peripheral attachment of the lateral meniscus to the tibial plateau—is carefully incised. Non-absorbable traction sutures (e.g., #2 or 2-0 Ethibond) are placed through the peripheral rim of the lateral meniscus.

By applying superior traction on these sutures, the meniscus is elevated, effectively opening a "book" to reveal the underlying lateral tibial plateau. A thorough joint inspection is then conducted to assess the extent of the articular comminution, clear fracture hematoma and loose chondral debris, and evaluate the integrity of the meniscus itself. Any peripheral meniscal tears identified at this stage must be repaired at the conclusion of the osseous fixation to restore joint stability and hoop stresses.

Fracture Reduction and Void Management
The crux of the procedure is the anatomical reduction of the articular surface. In cases of pure depression or split-depression fractures, the lateral cortical split is gently hinged open like a trapdoor. If the lateral cortex is intact (pure depression), a cortical window is created in the anterolateral metaphysis using a drill and osteotomes. Through this window, or through the open fracture line, specialized bone tamps are introduced inferior to the depressed articular fragments.

Under direct visual control (looking into the joint) and orthogonal fluoroscopic guidance, the depressed articular segments are carefully and progressively elevated until they are perfectly flush with the intact surrounding cartilage and the native joint line. Once anatomical reduction is achieved, it is provisionally stabilized using multiple smooth Kirschner wires (K-wires) placed subchondrally from lateral to medial, ensuring they do not violate the joint space.
The elevation of these osteoporotic articular fragments inevitably creates a substantial cavitary void within the metaphyseal bone. If left unsupported, the articular surface will almost certainly subside under the physiological loads of early rehabilitation. Therefore, this void must be meticulously filled.
Autologous cancellous bone graft from the iliac crest remains the biological gold standard due to its osteoconductive, osteoinductive, and osteogenic properties. However, structural allograft (e.g., crushed cancellous chips) or injectable calcium phosphate cements are increasingly utilized. Calcium phosphate is particularly advantageous in osteoporotic bone as it hardens in situ, providing immediate, high-compressive-strength structural support to the elevated articular fragments, thereby minimizing the risk of secondary subsidence.
Definitive Fixation Strategy
With the articular surface reduced and the metaphyseal void structurally supported, definitive internal fixation is applied. The modern standard of care involves the use of anatomically pre-contoured lateral proximal tibial locking plates. These plates are designed to match the complex flare of the lateral metaphysis and provide a fixed-angle construct that is mechanically superior in osteoporotic bone. The plate is slid submuscularly along the lateral tibial shaft and positioned optimally under fluoroscopy.
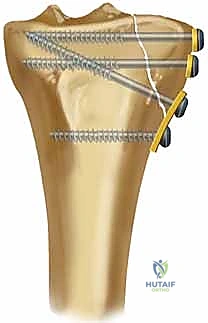
The critical step in fixation is the placement of subchondral "rafting" screws. These 3.5mm or 4.5mm locking screws are directed through the proximal holes of the plate, traversing the tibia from lateral to medial, immediately inferior to the subchondral bone plate.

This "raft" of screws acts as a rigid, weight-bearing scaffold, directly supporting the elevated articular fragments and the underlying bone graft/cement. Following the placement of the proximal articular screws, the diaphyseal portion of the plate is secured to the tibial shaft using a combination of non-locking screws (to pull the bone to the plate and restore the mechanical axis) and locking screws (to create a rigid, fixed-angle construct). Cortical lag screws may be utilized outside the plate or through the plate to compress the primary lateral split fragment against the intact medial plateau.
The Posterolateral Approach: An Alternative Strategy
While the anterolateral approach is sufficient for most patterns, fractures involving significant displacement of the posterior-lateral quadrant (often resulting from a knee flexion injury mechanism) may require a dedicated posterolateral approach. The anterolateral approach struggles to provide adequate visualization and orthogonal fixation for posterior shear fragments. The posterolateral approach involves a longitudinal incision centered over the posterior aspect of the fibular head.
The absolute critical step in this approach is the immediate identification, neurolysis, and protection of the common peroneal nerve. Once the nerve is safeguarded, access to the posterolateral tibia can be achieved either via a fibular head osteotomy (reflecting the fibular head and attached collateral ligament superiorly) or by dissecting anterior or posterior to the intact fibula. This approach allows for the placement of an anti-glide plate directly on the posterior aspect of the lateral plateau, effectively buttressing the posterior shear fragment against the deforming forces of the femoral condyle. If a fibular osteotomy is performed, it must be rigidly repaired at the conclusion of the case, typically with a tension band wire construct or a lag screw.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the operative management of lateral tibial plateau fractures is fraught with potential complications, largely due to the severe energy imparted to the soft tissue envelope and the complex intra-articular nature of the injury. Anticipation, early recognition, and aggressive management of these complications are critical to preserving limb function.
Soft tissue complications are the most frequently encountered and potentially devastating adverse events. Superficial wound dehiscence and deep surgical site infections (SSI) occur in approximately 5% to 15% of high-energy plateau fractures. The thin anteromedial soft tissue envelope is particularly vulnerable to necrosis if surgical incisions are poorly planned or if surgery is undertaken before the resolution of acute fracture edema. The implementation of staged protocols—utilizing temporary spanning external fixation until the "wrinkle sign" appears—has significantly reduced the incidence of catastrophic soft tissue failure. If a deep SSI occurs, it demands aggressive, emergent surgical irrigation and debridement. If the internal fixation remains rigidly stable, the hardware is generally retained while the patient undergoes a prolonged course of culture-directed intravenous antibiotics. However, if the hardware is loose or the infection is recalcitrant, hardware removal, aggressive bone debridement, and conversion to a circular external fixator (e.g., Ilizarov frame) may be required as a salvage procedure.
Loss of articular reduction and secondary subsidence of the lateral plateau is a major mechanical complication, particularly prevalent in the elderly, osteoporotic population. Premature weight-bearing, inadequate filling of the metaphyseal void, or failure to utilize fixed-angle locking technology can lead to the collapse of the elevated articular fragments.

This subsidence inevitably leads to a progressive valgus deformity of the mechanical axis and incongruity
Clinical & Radiographic Imaging Archive

