Masterclass: Precision Tibial Sesamoidectomy for Refractory Hallux Pain

Key Takeaway
This masterclass provides a comprehensive guide to tibial sesamoidectomy. Fellows will learn intricate surgical anatomy, patient positioning, and a step-by-step intraoperative technique from incision to closure. We'll cover critical neurovascular protection, meticulous dissection, and pearls for optimal outcomes in managing refractory hallux sesamoiditis and fractures.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows and colleagues, to the operating theater. Today, we are undertaking a masterclass on a surgical procedure that, while seemingly diminutive in its anatomical scale, demands immense surgical precision and a profound, nuanced understanding of forefoot biomechanics: the precision tibial sesamoidectomy. This intervention is never merely about the extirpation of an offending ossicle; it is fundamentally about restoring dynamic function, alleviating debilitating chronic pain, and meticulously preserving the delicate, unforgiving biomechanical balance of the first ray. The first metatarsophalangeal (MTP) joint is a marvel of evolutionary engineering, and any surgical alteration to its plantar apparatus must be approached with the utmost respect for its immense load-bearing responsibilities.
Patients presenting with refractory sesamoid pain typically harbor a complex clinical history characterized by either a distinct, high-energy acute traumatic event or, far more insidiously, a protracted course of repetitive microtrauma. Acute injuries frequently mimic the classic "turf toe" paradigm, involving an acute, forceful hyperextension of the hallux MTP joint under extreme axial load, or alternatively, a direct, blunt contusion to the plantar forefoot. Such high-velocity mechanisms can precipitate a frank transverse or comminuted fracture of the sesamoid. Furthermore, these forces can induce a traumatic disruption of the synchondrosis in a pre-existing congenital bipartite sesamoid, rendering the structural complex acutely unstable, mechanically incompetent, and profoundly painful.
Conversely, chronic injuries present a formidable diagnostic challenge, as patients rarely recall a singular inciting incident. Instead, they describe a gradual, unrelenting onset of activity-related discomfort that progressively limits their functional capacity and athletic performance. This insidious presentation is the hallmark of repetitive stress injuries, stress fractures, osteochondritis dissecans, and advanced sesamoid-metatarsal arthrosis. Avascular necrosis (AVN) of the sesamoid, historically referred to as Treves disease or Renander's disease, represents another critical etiology in this chronic cohort. It is characterized by subchondral collapse, cystic degeneration, and fragmentation secondary to compromised osseous perfusion, often exacerbated by the tenuous, watershed vascular supply of the sesamoid bones.
Epidemiologically, tibial sesamoid pathology exhibits a strong, well-documented predilection for specific athletic and occupational demographics. Dancers, particularly ballet dancers performing en pointe or demi-pointe, long-distance runners, gymnasts, and athletes engaged in court sports with frequent acceleration-deceleration forces are disproportionately affected. The pain is typically localized to the plantar medial aspect of the great toe, exacerbated unequivocally by weight-bearing and activities necessitating extreme hallux dorsiflexion. Consequently, patients often adopt a compensatory, antalgic gait characterized by external rotation of the lower extremity and lateral forefoot off-loading. If left unaddressed, this altered gait mechanic can subsequently precipitate secondary, recalcitrant kinetic chain pathologies extending proximally to the ankle, knee, hip, and lumbar spine.
Detailed Surgical Anatomy and Biomechanics
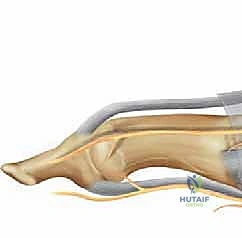
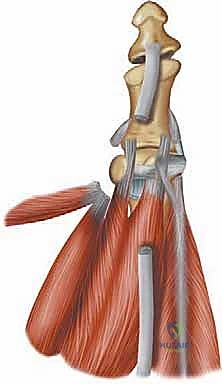
Before a scalpel ever touches the skin, an absolute mastery of the regional anatomy and biomechanics is non-negotiable. The sesamoid complex is an intricate, highly specialized anatomical pulley system integral to the functional integrity of the great toe. We possess two sesamoid bones—the medial (tibial) and lateral (fibular)—nestled securely plantar to the head of the first metatarsal. These ossicles are not merely floating bones; they are intimately embedded within the conjoined tendon of the flexor hallucis brevis (FHB) muscle. Biomechanically, they function as a crucial fulcrum, displacing the FHB tendon away from the joint center of rotation, thereby exponentially enhancing its mechanical advantage and moment arm during MTP joint plantarflexion.
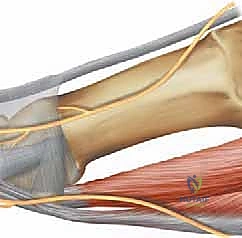
During the stance phase of the human gait cycle, and particularly during the critical toe-off phase, these sesamoids are subjected to extraordinary physiological stress, bearing up to three times the total body weight. The tibial sesamoid, being anatomically slightly larger, positioned more distally, and located directly under the primary medial weight-bearing column of the foot, typically absorbs a significantly higher proportion of this stress compared to its fibular counterpart. This asymmetrical load distribution elegantly explains the markedly increased incidence of traumatic and degenerative injuries we observe clinically in the tibial sesamoid. Any surgical disruption to this load-bearing column must account for the transfer of these immense forces to adjacent structures.
The articular relationships of the sesamoids are equally sophisticated and demand careful intraoperative consideration. The dorsal surfaces of both sesamoids articulate with highly specific, cartilage-covered facets on the plantar aspect of the first metatarsal head. These facets are anatomically separated by a prominent bony ridge known as the crista. This precise congruency is critical for smooth, frictionless gliding during the vast arc of hallux movement. Furthermore, the sesamoids serve a vital protective role; they act as a physiological tunnel, shielding the flexor hallucis longus (FHL) tendon, which passes directly between them, from the crushing forces of weight-bearing against the metatarsal head. They are tethered together by the robust intersesamoid ligament and are firmly integrated into the plantar plate complex, providing essential dynamic and static stability to the MTP joint.

Developmentally, ossification of the sesamoids typically occurs from multiple independent centers between the ages of seven and ten. This multifocal developmental process accounts for the relatively common incidental finding of bipartite (two distinct segments) or tripartite (three distinct segments) sesamoids. The tibial sesamoid is bipartite in approximately 19% to 30% of the general population, and this variation is bilateral in roughly 25% to 85% of those individuals. This anatomical idiosyncrasy frequently complicates the clinical picture, as radiographically differentiating a congenital, asymptomatic bipartite sesamoid from an acute, un-united fracture requires a highly discerning eye, an understanding of fracture morphology, and careful clinical correlation.
Exhaustive Indications and Contraindications
The decision to proceed with a tibial sesamoidectomy must be arrived at after a rigorous, exhaustive trial of conservative management. Surgical intervention is rarely a first-line treatment and should be reserved for definitive, refractory pathology that has failed to improve despite comprehensive non-operative measures. A comprehensive understanding of the precise indications and absolute contraindications is paramount to avoid disastrous postoperative complications, such as iatrogenic hallux valgus, progressive transfer metatarsalgia, or profound loss of push-off strength.
| Parameter | Clinical Details and Considerations |
|---|---|
| Primary Indications | - Refractory Sesamoiditis: Chronic, debilitating inflammation failing 6+ months of conservative care (custom orthotics, NSAIDs, off-loading boots, localized corticosteroid or PRP injections). - Fracture Non-union: Symptomatic non-union of a tibial sesamoid fracture with persistent pain upon weight-bearing and failure of bone stimulator therapy. - Avascular Necrosis (AVN): Advanced osteonecrosis with subchondral collapse, fragmentation, and secondary degenerative joint disease (Treves disease). - Osteomyelitis: Deep infection of the sesamoid, often secondary to a penetrating injury or chronic diabetic foot ulceration requiring source control. - Intractable Plantar Keratosis (IPK): Severe, painful IPK directly underlying a hypertrophic or plantar-flexed tibial sesamoid that is unresponsive to aggressive paring, off-loading, and footwear modification. |
| Absolute Contraindications | - Asymptomatic Bipartite Sesamoid: Incidental radiographic findings without correlating focal clinical tenderness or marrow edema on MRI. - Active Soft Tissue Infection: Unless the surgery is specifically indicated for radical debridement and excision of an infected sesamoid (osteomyelitis). - Severe Vascular Compromise: Peripheral arterial disease (PAD) precluding adequate wound healing without prior endovascular or surgical revascularization. - Neuropathic Arthropathy (Charcot): Active Charcot neuroarthropathy of the forefoot, which requires stabilization rather than destabilizing excision. |
| Relative Contraindications | - Pre-existing Hallux Valgus: Excision of the tibial sesamoid removes the medial stabilizing force of the FHB, risking rapid, severe progression of the valgus deformity. Concomitant corrective osteotomy or soft tissue balancing is mandatory. - Prior Fibular Sesamoidectomy: Excision of both sesamoids severely destabilizes the MTP joint, leading to a profound "cock-up" deformity and loss of push-off power. If both must be addressed, primary MTP arthrodesis is the preferred salvage. - High-Demand Athletes: Extreme caution must be exercised in elite sprinters or jumpers, as the loss of the FHB lever arm can result in a measurable decrease in peak push-off strength and athletic performance. |
The evaluation of a patient for this procedure requires a holistic view of foot biomechanics, extending beyond the isolated pathology of the sesamoid. If a patient presents with a symptomatic tibial sesamoid but also demonstrates clinical and radiographic evidence of a hypermobile first ray or a pre-existing hallux valgus deformity, isolated sesamoidectomy is a biomechanical trap. The tibial sesamoid and its attachment to the medial head of the FHB and the abductor hallucis provide essential varus restraint. Removing this restraint in the presence of an uncorrected valgus moment will inevitably result in a catastrophic, progressive hallux valgus deformity that is notoriously difficult to salvage. In such cases, a concomitant chevron or scarf osteotomy must be strongly considered.
Conversely, if the patient has a rigid, cavus foot type with a plantarflexed first ray, the tibial sesamoid is subjected to exponentially higher sheer and compressive forces. In these scenarios, while the sesamoidectomy will successfully remove the primary pain generator, the underlying biomechanical driver remains entirely unaddressed. The surgeon must strongly consider a concomitant dorsiflexory wedge osteotomy of the first metatarsal to elevate the ray and prevent subsequent, inevitable transfer lesions to the lesser metatarsal heads or the remaining, highly vulnerable fibular sesamoid.
In cases of chronic, severe osteonecrosis where the sesamoid is entirely fragmented, the bone essentially acts as loose intra-articular bodies within the plantar tendon sheath. In these definitive cases, the indication for excision is absolute, as no amount of conservative off-loading will reconstitute the necrotic bone or reverse the secondary arthrosis occurring at the sesamoid-metatarsal articulation. The goal here shifts from preservation to meticulous debridement and reconstruction of the plantar soft tissue envelope to restore a smooth gliding surface for the MTP joint.
Pre-Operative Planning, Templating, and Patient Positioning
A meticulous pre-operative workup is the absolute foundation of a successful surgical outcome. The physical examination must be exhaustive and highly specific. Inspection should seek out subtle, localized swelling, erythema, or hyperkeratosis over the plantar-medial aspect of the hallux MTP joint. Direct, pinpoint palpation under the tibial sesamoid will elicit exquisite tenderness. This pain is characteristically exacerbated with forced, passive dorsiflexion of the hallux MTP joint, a maneuver which stretches the FHB complex tightly against the metatarsal head, compressing the inflamed sesamoid. The surgeon must also perform a Tinel sign directly over the tibial sesamoid; a positive sign, manifesting as radiating paresthesia distally into the medial hallux, strongly suggests concomitant compression or irritation of the medial plantar proper digital nerve.

Range of motion (ROM) assessment is critical for baseline documentation and surgical planning. The surgeon must isolate the MTP joint by stabilizing the metatarsal head with one hand and manipulating the proximal phalanx with the other, carefully noting any crepitus, loss of ROM, or asymmetry compared to the contralateral, asymptomatic foot. For suspected acute injuries or bipartite sesamoid disruptions, a careful drawer test of the hallux MTP joint is performed by applying dorsal-to-plantar stress. Detectable laxity or a palpable "clunk" can indicate a profound structural failure of the plantar plate or a catastrophic synchondrosis disruption requiring more extensive soft tissue repair.
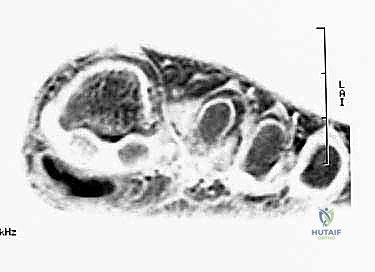
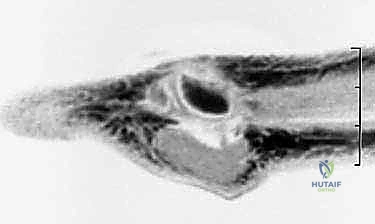
Appropriate imaging is essential for diagnostic accuracy and precise surgical planning. Routine radiographs must include weight-bearing anteroposterior (AP), lateral, oblique, and specialized axial sesamoid views. The axial view is particularly invaluable, offering a tangential perspective of the sesamoid-metatarsal articulation, often revealing subtle joint space narrowing, subchondral sclerosis, or crista erosion diagnostic of advanced arthrosis. Differentiating a congenital bipartite sesamoid from a true fracture remains a classic radiologic challenge. A fracture line is typically sharp, irregular, and lacks sclerotic margins, whereas a bipartite sesamoid generally exhibits smooth, well-corticated, rounded edges at the synchondrosis.

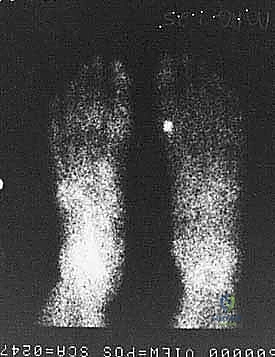
When standard radiography is equivocal, advanced imaging becomes mandatory. A triple-phase Technetium-99m bone scan is highly sensitive and can demonstrate intensely increased focal uptake in the tibial sesamoid region long before gross radiographic changes manifest, indicating acute metabolic activity consistent with a stress fracture or early AVN. Collimated, pinhole views of the MTP joint are crucial for precise anatomical localization. Alternatively, Magnetic Resonance Imaging (MRI) is the gold standard for assessing soft tissue integrity, evaluating the articular cartilage, and definitively diagnosing bone marrow edema patterns characteristic of early osteonecrosis, occult stress responses, or flexor tenosynovitis.


In the operating room, meticulous patient positioning sets the stage for a smooth, uncomplicated procedure. The patient is placed in the supine position on a standard radiolucent operating table to facilitate intraoperative fluoroscopy. A small bump is often placed under the ipsilateral hip to internally rotate the leg slightly, bringing the medial aspect of the foot into a more accessible, direct line of sight for the surgeon. A well-padded thigh or calf tourniquet is applied to ensure a pristine, bloodless surgical field, which is absolutely critical when dissecting around the delicate plantar digital nerves. Intravenous prophylactic antibiotics are administered prior to tourniquet inflation, and the extremity is prepped and draped in standard sterile fashion.
Step-by-Step Surgical Approach and Fixation Technique
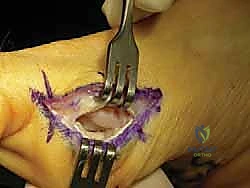
The surgical approach to the tibial sesamoid requires a delicate balance between achieving adequate exposure and minimizing iatrogenic soft tissue trauma. A medial plantar approach is the gold standard, favored over a direct plantar approach to avoid creating a painful, weight-bearing scar. The incision is carefully planned, typically measuring 3 to 4 centimeters in length. It is centered directly over the palpable tibial sesamoid, positioned just plantar to the medial midline of the first MTP joint, traversing the junction of the dorsal and plantar skin. This placement ensures the resulting scar lies safely above the primary weight-bearing surface of the forefoot.



Superficial dissection is carried out with meticulous hemostasis. The immediate, critical anatomical hazard in this layer is the medial plantar proper digital nerve to the hallux. This nerve courses longitudinally just plantar to the incision line and is highly susceptible to traction injury or inadvertent transection. Using blunt dissection and fine retractors, the nerve must be identified, gently mobilized, and protected throughout the entirety of the procedure. Retraction should be gentle to avoid neuropraxia. Once the nerve is secured, the deep fascia is incised, exposing the medial capsule of the first MTP joint and the robust medial band of the flexor hallucis brevis (FHB) tendon enveloping the tibial sesamoid.
The capsulotomy is performed longitudinally, directly in line with the FHB fibers. The surgeon must now execute the most technically demanding portion of the procedure: shelling the sesamoid out of its tendinous bed without compromising the continuity of the FHB tendon or the plantar plate. This is achieved using a combination of sharp dissection with a #15 blade and careful periosteal elevation. The dissection must remain strictly extra-articular to the FHL tendon, which lies immediately lateral to the tibial sesamoid. Inadvertent violation of the FHL sheath can lead to devastating postoperative adhesions, severely limiting hallux plantarflexion.



As the sesamoid is mobilized, the robust intersesamoid ligament attaching it to the fibular sesamoid must be sharply divided. In cases of severe fragmentation or AVN, the bone must be removed piecemeal, ensuring no osseous debris is left behind within the joint space or tendon sheath. Following complete extirpation, the surgical site is copiously irrigated. The critical reconstructive step follows: the resulting defect in the medial FHB tendon and plantar capsule must be meticulously repaired. Failure to reapproximate these tissues results in unopposed pull from the adductor hallucis and the lateral head of the FHB, virtually guaranteeing a rapid, severe iatrogenic hallux valgus deformity.

The repair is typically executed using non-absorbable or slow-absorbing heavy sutures (e.g., 2-0 or 0 Vicryl/FiberWire) in a figure-of-eight or horizontal mattress configuration, tightly imbricating the medial capsular structures. The surgeon should manually stress the MTP joint intraoperatively to confirm stability and ensure the hallux rests in neutral alignment. Subcutaneous tissues are closed with absorbable sutures, and the skin is approximated with non-absorbable monofilament or a subcuticular stitch. A bulky, compressive forefoot dressing is applied, splinting the hallux in slight plantarflexion and neutral adduction/abduction to protect the capsular repair.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, tibial sesamoidectomy carries a distinct profile of potential complications. A comprehensive understanding of these risks is essential for informed patient consent and prompt postoperative management. The most feared complication is the disruption of the first ray's biomechanical balance, leading to progressive deformity.
| Complication | Incidence Rate | Pathophysiology and Salvage Management |
|---|---|---|
| Iatrogenic Hallux Valgus | 5% - 10% | Caused by failure to adequately repair the medial FHB/capsular defect, leading to unopposed lateral pull. Salvage: Requires revision surgery, often necessitating a lateral soft tissue release, medial capsulorrhaphy, and potentially a first metatarsal corrective osteotomy. |
| Nerve Injury / Neuroma | 2% - 8% | Direct transection or traction neuropraxia of the medial plantar proper digital nerve. Presents as intractable localized pain, paresthesia, and a positive Tinel sign. Salvage: Initial treatment involves gabapentinoids and localized steroid injections. Refractory cases require surgical exploration, |
Clinical & Radiographic Imaging Archive


