Masterclass: Operative Management of Thumb CMC Joint Fractures

Key Takeaway
Join us in the OR for a comprehensive masterclass on operative management of thumb CMC joint fractures. This guide details preoperative planning, precise surgical anatomy, step-by-step intraoperative execution for Bennett and Rolando fractures, including both closed reduction percutaneous pinning (CRPP) and open reduction internal fixation (ORIF) techniques. Learn critical pearls, potential pitfalls, and comprehensive postoperative care for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The thumb carpometacarpal (CMC) joint is the evolutionary cornerstone of human prehension, providing the unparalleled ability to position the thumb in space for forceful grasp, precision pinch, and intricate manipulation. This unique articulation accounts for approximately forty percent of overall hand function. Consequently, fractures involving the base of the first metacarpal are not merely skeletal disruptions; they are catastrophic threats to the kinematic chain of the hand. When the articular congruity or ligamentous stability of the thumb CMC joint is compromised, the resulting biomechanical cascade leads inexorably to pain, weakness, and rapid-onset post-traumatic arthrosis. As orthopedic surgeons, our mandate is clear: we must achieve anatomic reduction of the articular surface and restore absolute mechanical stability to permit early, functional rehabilitation.
Epidemiologically, fractures of the thumb metacarpal base are predominantly high-energy injuries, most frequently observed in young, active male populations. The classic mechanism of injury involves an axial load applied to a partially flexed thumb metacarpal, commonly occurring during altercations (the "fighter's fracture" variant), athletic endeavors, or motor vehicle collisions. This axial force vector is transmitted directly through the metacarpal shaft into the trapezium, creating significant shear and compressive forces across the articular surface. Depending on the exact position of the thumb at the moment of impact and the magnitude of the applied force, the resulting failure pattern may manifest as a simple extra-articular fracture, a classic two-part fracture-dislocation, or a highly comminuted articular impaction injury.
Understanding the patho-epidemiology is critical for anticipating associated injuries and formulating a comprehensive treatment strategy. Because these are often high-energy mechanisms, the surgeon must maintain a high index of suspicion for concomitant pathology within the carpus and surrounding soft tissue envelope. Injuries such as trapezial body fractures, scaphotrapezial-trapezoid (STT) joint disruptions, and severe sprains of the ulnar collateral ligament (UCL) at the metacarpophalangeal (MCP) joint can occur simultaneously. Furthermore, the robust musculotendinous forces acting upon the thumb metacarpal inevitably transform these fractures into highly unstable entities, dictating that nonoperative management is rarely successful for displaced intra-articular patterns.
Detailed Surgical Anatomy and Biomechanics
Before we even consider an incision, a profound and nuanced understanding of the anatomy and biomechanics of the thumb CMC joint is paramount. This articulation, formed by the thumb metacarpal base and the trapezium, is a true saddle joint (toroid articulation). Its reciprocally interlocking articular surfaces—concave in one plane and convex in the orthogonal plane—allow for a remarkable and complex range of motion. This geometry permits flexion-extension, abduction-adduction, and the critical composite motion of circumduction, which is the absolute prerequisite for opposition.
Osteology and Articular Kinematics
The osseous architecture of the thumb CMC joint is inherently unstable without its soft tissue envelope. The articular surface of the trapezium is saddle-shaped, articulating with the reciprocally shaped base of the first metacarpal. During palmar abduction, the metacarpal base glides dorsally on the trapezium, while during adduction, it glides volarly. Flexion and extension involve a complex rolling and gliding mechanism along the orthogonal axis. This intricate kinematic dance means that any articular step-off greater than 1 millimeter will drastically alter contact pressures, leading to point loading, accelerated cartilage wear, and inevitable early-onset osteoarthritis.


Ligamentous Stabilizers and Deforming Forces
The stability of this vital joint is maintained by a complex array of primary ligaments. Imagine them as the dynamic guy wires of a tent, meticulously balancing forces to keep the joint congruent under immense physiological loads. The Anterior-volar (Beak) Ligament is arguably the most critical stabilizer. It originates from the volar aspect of the trapezium and inserts onto the volar-ulnar aspect of the thumb metacarpal base. Its immense tensile strength is what invariably keeps the small volar-ulnar fragment of a Bennett fracture anatomically reduced to the trapezium, even as the rest of the metacarpal subluxates. Other vital ligaments include the Posterior Oblique Ligament, the Dorsal Radial Ligament (which strongly resists dorsal translation), and the Anterior and Posterior Intermetacarpal Ligaments.

The deforming forces acting upon these fractures are relentless and powerful. The thumb metacarpal serves as the attachment site for several robust tendons that, when disrupted by fracture, immediately become primary deforming vectors. The Abductor Pollicis Longus (APL) inserts at the base of the thumb metacarpal and pulls the metacarpal shaft radially and proximally. The Adductor Pollicis (AP) inserts distally on the thumb, contributing to massive ulnar angulation and a supination moment. Concurrently, the Extensor Pollicis Longus (EPL) inserts on the distal phalanx, further exacerbating the ulnar and dorsal angulation of the metacarpal shaft.
Fracture Patterns and Buchler Zones
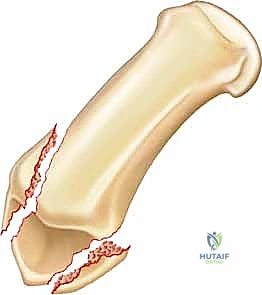
These deforming forces lead to classic intra-articular fracture-dislocation patterns. The Bennett Fracture is a two-part intra-articular fracture where the metacarpal shaft is radially and dorsally displaced by the pull of the APL. Crucially, a small, intact ulnar fragment remains at the base of the thumb metacarpal, held perfectly reduced by the strong volar beak ligament. The Rolando Fracture represents a more complex, comminuted intra-articular fracture involving the base of the thumb metacarpal, classically presenting as a T or Y-type pattern. By definition, no portion of the metacarpal shaft remains in continuity with the CMC joint, rendering it profoundly unstable.


Buchler et al. elegantly described three critical zones at the base of the thumb metacarpal, which guide our understanding of stability and operative indications. Zone 1 encompasses the volar aspect of the joint, typically involving the beak ligament avulsion. Zone 2 represents the central, normally loaded portion of the joint; involvement here is absolutely critical for load transfer and stability, almost universally mandating operative intervention. Zone 3 encompasses the dorsal aspect of the joint. Understanding these zones allows the surgeon to conceptualize the fracture in three dimensions and plan the trajectory of internal fixation devices accordingly.

Exhaustive Indications and Contraindications
The decision-making process for managing thumb CMC joint fractures hinges on a meticulous evaluation of articular congruity, overall joint stability, and the functional demands of the patient. While truly non-displaced extra-articular fractures can occasionally be managed with rigid cast immobilization, the threshold for surgical intervention in intra-articular patterns is exceedingly low. The fundamental tenet of intra-articular fracture management applies here with absolute rigidity: articular step-offs alter joint kinematics and drastically increase focal contact stresses. Therefore, any intra-articular displacement greater than 1.0 to 1.5 millimeters is an absolute indication for operative reduction.
Furthermore, subluxation or dislocation of the metacarpal shaft relative to the trapezium, regardless of the size of the articular fragment, demands surgical stabilization. In Bennett fractures, the strong pull of the APL virtually guarantees that closed reduction will be lost once swelling subsides if not mechanically stabilized. For Rolando and highly comminuted patterns, the goal shifts from simple lag screw fixation to joint-spanning stabilization or complex buttress plating to prevent axial shortening and articular collapse. The surgeon must carefully weigh the physiological age, functional requirements, and medical comorbidities of the patient against the risks of surgical intervention.
| Parameter | Operative Indications (ORIF / CRPP / Ex-Fix) | Non-Operative Indications (Cast Immobilization) | Absolute Contraindications to Surgery |
|---|---|---|---|
| Articular Step-off | > 1.0 mm displacement | < 1.0 mm, perfectly congruent | N/A |
| Joint Stability | Subluxation or dislocation present | Stable through full ROM under fluoro | N/A |
| Fracture Pattern | Bennett, Rolando, severe comminution | Extra-articular, non-displaced | N/A |
| Angulation | > 30 degrees of angular deformity | < 30 degrees, easily reducible | N/A |
| Patient Factors | High functional demand, young age | Low demand, extreme surgical risk | Active local infection, critically ill |
| Pre-existing Disease | Normal joint space pre-injury | N/A | Severe pantrapezial arthritis (consider primary fusion/arthroplasty instead) |
Contraindications to internal fixation are generally limited but must be strictly respected. Active soft tissue infection in the surgical field is an absolute contraindication to internal hardware placement. Additionally, in elderly, low-demand patients with severe, pre-existing pantrapezial osteoarthritis, attempting complex ORIF of a comminuted fracture may be an exercise in futility. In such specific scenarios, nonoperative management followed by delayed salvage procedures (such as trapeziectomy with ligament reconstruction and tendon interposition) or primary acute arthrodesis may be the more prudent and definitively successful clinical pathway.
Pre-Operative Planning, Templating, and Patient Positioning
Success in the operating room begins long before the first incision is made; it is forged in the meticulous details of preoperative planning. A comprehensive clinical and radiographic assessment is non-negotiable to prevent intraoperative surprises and ensure optimal outcomes.
Clinical Evaluation and Diagnostic Imaging
The clinical evaluation must begin with a detailed history, focusing on the mechanism of injury, occupational demands, and hand dominance. Physical examination will typically reveal profound localized tenderness, swelling, and ecchymosis around the thenar eminence. Palpable instability or a visible "shelf" deformity at the CMC joint strongly suggests dorsal subluxation of the metacarpal shaft. A rigorous neurovascular examination is mandatory, with specific attention paid to the superficial radial nerve and the palmar cutaneous branch of the median nerve, both of which are at risk during surgical approaches to this region.
Our imaging protocol must be exhaustive to provide a three-dimensional understanding of the fracture morphology. Standard hand radiographs are insufficient due to the unique 30-degree pronated position of the thumb relative to the rest of the carpus. A True AP View of the Thumb CMC Joint (Robert's view) is obtained with maximal forearm pronation, placing the dorsum of the thumb flat on the cassette. This optimizes visualization of the joint space and the critical ulnar fragment. The True Lateral View (Billing and Gedda) is achieved with the hand pronated 20 degrees and the thumb flat on the cassette, with the X-ray beam tilted 10 degrees from vertical in a distal-to-proximal direction.


For complex, multi-fragmentary Rolando fractures, a Traction View under fluoroscopy is indispensable. Distraction at the CMC joint utilizes ligamentotaxis to help delineate comminuted fragments and assess the potential for closed reduction and percutaneous pinning versus the absolute need for open plating. Furthermore, when plain films inadequately delineate the spatial orientation of fracture fragments, particularly in Zone 2, a high-resolution Computed Tomography (CT) scan is strictly indicated. 3D reconstructions are invaluable for preoperative templating, allowing the surgeon to precisely map screw trajectories and select appropriate plate morphology before entering the operating theater.

Patient Positioning and Operating Room Setup
Proper patient positioning is critical for unhindered surgical access and seamless fluoroscopic imaging. The patient is placed supine on the operating table with the affected extremity extended onto a radiolucent hand table. A well-padded upper arm tourniquet is applied to ensure a bloodless surgical field, which is absolutely essential for identifying small articular fragments and protecting delicate neurovascular structures.
The fluoroscopy unit (C-arm) should be positioned either parallel or perpendicular to the hand table, depending on the surgeon's preference, but it must be highly mobile to allow for rapid acquisition of true AP and lateral views of the thumb without physically manipulating the reduced fracture. The surgeon typically sits in the axilla, with the surgical assistant opposite. Preoperative templating should be displayed prominently on the monitors. All potential fixation modalities—including 1.5mm and 2.0mm lag screws, mini-fragment locking plates, T-plates, and K-wires—must be readily available in the room prior to induction of anesthesia.
Step-by-Step Surgical Approach and Fixation Technique
The operative management of thumb CMC fractures demands meticulous soft tissue handling, precise articular reduction, and rigid biomechanical fixation. The specific technique chosen is dictated entirely by the fracture morphology, fragment size, and degree of comminution.
Closed Reduction and Percutaneous Pinning (CRPP)
CRPP is the treatment of choice for classic Bennett fractures where the volar-ulnar fragment is too small to reliably accept a lag screw, yet the joint can be anatomically reduced closed. The reduction maneuver is highly specific, designed to counteract the deforming forces of the APL and Adductor Pollicis. Longitudinal traction is applied to the thumb, followed by palmar abduction and pronation. Direct pressure is then applied to the dorsal-radial aspect of the metacarpal base, effectively pushing the shaft back into the anatomic cradle of the intact volar-ulnar fragment.
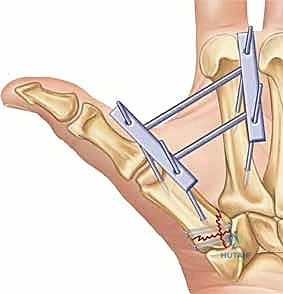
Once anatomic reduction is confirmed via multi-planar fluoroscopy, percutaneous fixation is achieved. Typically, two 0.045-inch or 0.062-inch Kirschner wires are utilized. The first wire is driven from the dorsal-radial aspect of the metacarpal shaft directly into the trapezium, effectively neutralizing the proximal pull of the APL. A second wire is often placed transversely from the first metacarpal shaft into the second metacarpal to control rotation and maintain the web space. Pins are cut outside the skin and capped to facilitate easy removal in the clinic.



Open Reduction and Internal Fixation (ORIF) - Wagner Approach
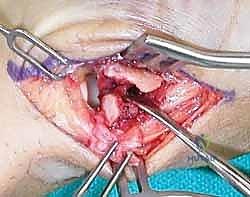
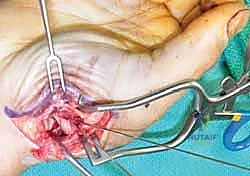
For fractures with large volar-ulnar fragments (>20% of the articular surface), displaced Rolando fractures, or cases where closed reduction fails, ORIF is unequivocally mandated. The classic Wagner approach provides unparalleled exposure to the thumb CMC joint. A curvilinear incision is made along the glabrous border of the thenar eminence, curving dorsally at the level of the CMC joint.


Meticulous superficial dissection is required to identify and protect the sensory branches of the superficial radial nerve dorsally and the palmar cutaneous branch of the median nerve volarly. The thenar musculature (abductor pollicis brevis and opponens pollicis) is sharply elevated from the metacarpal shaft and retracted volarly. The joint capsule is then incised longitudinally or in an L-shaped fashion to expose the articular surface. The hematoma is evacuated, and the fracture fragments are meticulously debrided of interposed soft tissue.


For a large fragment Bennett fracture, the shaft is reduced to the volar-ulnar fragment using a pointed reduction clamp. Provisional fixation is achieved with a K-wire. A 1.5mm or 2.0mm lag screw is then placed perpendicular to the fracture plane. The near cortex must be overdrilled (gliding hole) and the far cortex underdrilled (thread hole) to achieve true interfragmentary compression. The screw head should be countersunk to prevent hardware prominence beneath the thenar muscles.




Fixation Strategies for Rolando and Comminuted Patterns
Rolando fractures present a significantly higher degree of complexity. The classical Y or T pattern often precludes simple lag screw fixation. In these instances, mini-fragment plating is the gold standard. T-plates or specialized condylar plates are contoured to fit the complex geometry of the metacarpal base. The articular fragments are first reduced and provisionally pinned, essentially converting the complex intra-articular fracture into a simpler two-part extra-articular fracture. The plate is then applied to buttress the articular fragments and bridge the metaphyseal comminution to the diaphysis.





In cases of severe, non-reconstructable articular comminution where internal fixation is impossible, joint-spanning external fixation combined with limited internal fixation (K-wires) is utilized. The external fixator relies on the principle of ligamentotaxis to restore length and align the articular fragments. Pins are placed in the trapezium (or radius) and the thumb metacarpal shaft, distracting the joint to allow for secondary bone healing while preventing collapse.


Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following thumb CMC joint fractures are not uncommon, primarily due to the complex biomechanics and high intrinsic loads placed upon this small articulation. The surgeon must be adept at recognizing these complications early and instituting appropriate salvage pathways.
The most frequent and debilitating complication is post-traumatic osteoarthritis. Even with anatomic reduction, the initial cartilage impact injury can lead to chondrocyte apoptosis and progressive joint space narrowing. If articular step-off exceeds 1mm, the incidence of symptomatic arthrosis approaches 100% within a decade. Patients typically present with progressive pain, weakness in pinch grip, and a positive grind test.
Iatrogenic complications, particularly sensory nerve injuries, are also prevalent. The superficial radial nerve is highly susceptible to traction neurapraxia or direct laceration during the Wagner approach or percutaneous pin placement. Pin tract infections are common with CRPP but usually resolve with oral antibiotics and pin removal. Nonunion is exceedingly rare due to the robust vascular supply of the metaphyseal bone, but malunion—specifically dorsal and radial angulation—can occur if fixation is inadequate or fails prematurely.
| Complication | Estimated Incidence | Etiology / Risk Factors | Management / Salvage Strategy |
|---|---|---|---|
| Post-Traumatic Arthritis | 20% - 50% (Long-term) | Articular step-off >1mm, initial cartilage impaction | NSAIDs, injections; ultimately Trapeziectomy with LRTI or CMC Arthrodesis |
| Superficial Radial Nerve Neuritis | 5% - 15% | Traction during Wagner approach, direct pin injury | Gabapentinoids, desensitization; surgical neurolysis if refractory |
| Pin Tract Infection | 10% - 20% (if CRPP used) | Prolonged pin retention, poor local hygiene | Oral antibiotics, early pin removal if purulent |
| Malunion / Loss of Reduction | 5% - 10% | Inadequate fixation, premature hardware removal | Corrective osteotomy (if extra-articular) or salvage arthroplasty |
| First Web Space Contracture | < 5% | Prolonged immobilization in adduction | Aggressive therapy, Z-plasty release if severe |



For end-stage post-traumatic arthritis or severe, symptomatic malunions, salvage procedures are highly effective. In younger, high-demand laborers, CMC joint arthrodesis provides a stable, painless thumb, albeit at the cost of circumduction. In older or lower-demand patients, trapeziectomy with ligament reconstruction and tendon interposition (LRTI) yields excellent pain relief while preserving functional mobility.
Phased Post-Operative Rehabilitation Protocols
The ultimate functional outcome of a surgically managed thumb CMC fracture is as dependent on the postoperative rehabilitation protocol as it is on the surgical fixation itself. The delicate balance between protecting the healing osteosynthesis and preventing debilitating stiffness requires a phased, highly supervised approach in conjunction with a certified hand therapist.
Phase 1: Maximum Protection (Weeks 0-4)
Immediately postoperatively, the thumb is immobilized in a bulky, well-padded thumb spica splint. The thumb must be positioned in palmar abduction and slight extension to maintain the first web space and neutralize the pull of the adductor pollicis. During this phase, the primary goals are edema control and protection of the fixation. Active range of motion (AROM) of the interphalangeal (IP) joint of the thumb, as well as all uninvolved digits, is initiated immediately to prevent tendon adhesions and promote venous return. If percutaneous pins were
