Masterclass: Open Reduction and Internal Fixation of Tibial Tuberosity Fractures

Key Takeaway
This masterclass guides fellows through open reduction and internal fixation of tibial tuberosity fractures. We cover essential anatomy, preoperative planning, precise intraoperative steps, instrument use, and critical decision-making. Learn to manage neurovascular risks, achieve anatomical reduction, and select appropriate hardware. We also discuss pearls, pitfalls, and comprehensive postoperative rehabilitation protocols for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Tibial tuberosity avulsion fractures represent a relatively rare but highly significant orthopedic injury, accounting for less than 3% of all epiphyseal tract injuries and approximately 1% of all physeal injuries in the pediatric and adolescent populations. Despite their statistical infrequency, these fractures demand meticulous surgical attention due to their potential for severe functional impairment, disruption of the extensor mechanism, and devastating acute complications such as anterior compartment syndrome. Occurring predominantly in adolescent males between the ages of 12 and 16, this injury profile directly correlates with the final stages of skeletal maturation, a period during which the apophyseal physis undergoes a critical transition from a cartilaginous structure to a fully ossified bony union. The vulnerability of the tibial tubercle during this specific developmental window is the defining pathophysiological feature of this fracture pattern.
The classic mechanism of injury involves a massive, sudden, and forceful eccentric contraction of the quadriceps muscle complex against a fixed lower extremity. This is most frequently observed during athletic endeavors that require explosive jumping, sprinting, or rapid deceleration—such as basketball, gymnastics, and track and field events. Alternatively, the injury can be precipitated by a sudden, violent passive flexion of the knee joint while the quadriceps is maximally contracted, essentially overpowering the tensile strength of the developing apophysis. The immense forces generated by the extensor mechanism are transmitted directly through the patellar ligament, culminating in a catastrophic tensile failure at the weakest link: the partially fused tibial tuberosity apophysis and its surrounding periosteal sleeve.
It is widely hypothesized within the orthopedic literature that adolescents who sustain these injuries often possess quadriceps muscle strength that disproportionately exceeds the tensile strength of their maturing physes. Furthermore, a well-documented predisposing factor is a preceding clinical history of Osgood-Schlatter disease. This chronic traction apophysitis induces microtrauma, structural weakening, and subsequent disorganized healing of the apophyseal cartilage, effectively priming the anatomical site for an acute avulsion event under peak loading conditions. Clinically, patients present in acute distress, demonstrating profound swelling, ecchymosis, and exquisite point tenderness over the anterior proximal tibia.
A hallmark diagnostic indicator, particularly in displaced Ogden Type II and III fractures, is the complete inability to actively extend the knee against gravity, signifying a functional discontinuity of the extensor mechanism. Secondary clinical signs often include a palpable defect at the tibial tubercle and the presence of patella alta, resulting from the unresisted proximal migration of the avulsed bony fragment and the attached patellar ligament. Given the high-energy nature of the avulsion and the proximity of vital vascular structures, a comprehensive and continuously monitored neurovascular examination is absolutely paramount. The rapid accumulation of hematoma within the tight fascial confines of the anterior leg places these patients at an exceptionally high risk for acute anterior compartment syndrome, a limb-threatening surgical emergency that supersedes all other immediate management priorities.
Detailed Surgical Anatomy and Biomechanics
To execute a flawless open reduction and internal fixation, the operating surgeon must possess an intimate understanding of the proximal tibial osteology, its developmental stages, and the complex interplay of the surrounding soft tissue envelope. The tibial tubercle is not a static anatomical entity; rather, it evolves through four distinct developmental stages that dictate its biomechanical vulnerability. The first is the Cartilaginous Stage, present from birth, where the tubercle is entirely composed of hyaline cartilage. The second is the Apophyseal Stage (typically ages 8-12 in girls, 9-14 in boys), characterized by the appearance of a secondary center of ossification within the cartilage, remaining distinct from the main proximal tibial epiphysis. This stage is the classic anatomical substrate for Osgood-Schlatter disease and Ogden Type I fractures.
The third stage, the Epiphyseal Stage (ages 10-15 in girls, 11-17 in boys), is the most critical for the injuries discussed in this masterclass. During this phase, the ossific nucleus of the apophysis coalesces with the main proximal tibial epiphysis, forming a continuous "tongue" of bone, yet the underlying physis remains open and mechanically susceptible to shear and tensile forces. It is during this transitional period that Ogden Type II and III fractures typically occur. Finally, the Bony Fusion Stage marks the complete obliteration of the physis, integrating the tubercle fully into the proximal tibial metaphysis, after which avulsion fractures become exceedingly rare, typically replaced by patellar tendon ruptures in adults. The patellar ligament inserts into the proximal aspect of this apophysis, with its fibers fanning out into a broad, robust insertion into the periosteum distal to the tubercle. Crucially, the functional center of this insertion is slightly lateral to the anatomical midline, a detail that dictates the lateral rotational tendency of the avulsed fragment and directly influences our choice of surgical approach.
The vascular anatomy surrounding the proximal tibia is of critical surgical importance, primarily due to the anterior tibial recurrent artery. This vessel originates from the anterior tibial artery shortly after it passes through the interosseous membrane, ascending anteriorly to supply the proximal anterior compartment and the anterolateral knee joint capsule. During a violent avulsion of the tibial tuberosity, the proximal displacement of the bony fragment and the tearing of the thick periosteal sleeve frequently lacerate this artery or its major branches. The resulting high-pressure arterial hemorrhage bleeds directly into the unyielding anterior compartment of the lower leg. This specific anatomical relationship is the primary anatomical driver for the high incidence of acute anterior compartment syndrome associated with this fracture pattern, necessitating extreme vigilance and often prophylactic surgical intervention.
Neurologically, the anterior aspect of the knee is innervated by the infrapatellar branch of the saphenous nerve. This purely sensory nerve branches from the saphenous nerve at the medial aspect of the knee, piercing the sartorius fascia and traversing transversely or inferolaterally across the anterior knee joint capsule and patellar tendon to supply sensation to the anteromedial and anterolateral proximal lower leg. Because of its superficial and transverse course, it is highly susceptible to iatrogenic transection during standard midline anterior surgical incisions. Injury to this nerve can result in a painful postoperative neuroma, persistent dysesthesia, or a frustrating area of numbness for the young athlete. Therefore, surgical approaches must be meticulously planned to either identify and protect this nerve or, preferably, utilize an incision trajectory that inherently minimizes the risk of encountering it.
Exhaustive Indications and Contraindications
The overarching philosophy in the management of tibial tuberosity fractures is the anatomical restoration of the extensor mechanism, the preservation of the articular surface (in Type III injuries), and the prevention of both acute and chronic complications. While certain minimally displaced fractures can be managed conservatively, the threshold for surgical intervention is low due to the high functional demands of the affected patient demographic.
| Category | Specific Criteria | Clinical Rationale |
|---|---|---|
| Absolute Indications | Displacement > 2mm | Prevents extensor lag, restores biomechanical advantage, and prevents nonunion/malunion. |
| Absolute Indications | Extensor Mechanism Incompetence | Inability to perform a straight leg raise indicates functional discontinuity requiring mechanical repair. |
| Absolute Indications | Intra-articular Extension (Type III) | Requires anatomical reduction of the joint surface to prevent early-onset post-traumatic osteoarthritis. |
| Absolute Indications | Meniscal Entrapment | Interposed meniscal tissue prevents reduction and requires open extraction and potential repair. |
| Absolute Indications | Acute Compartment Syndrome | Requires immediate four-compartment fasciotomy; fracture fixation is performed concomitantly. |
| Relative Indications | Severe Periosteal Stripping | Significant soft tissue disruption may require open repair to ensure adequate healing and prevent fragment migration. |
| Absolute Contraindications | Active Local Infection | Cellulitis or active joint infection precludes internal fixation until the infection is eradicated. |
| Relative Contraindications | Minimally Displaced (<2mm) Type I | Can often be managed with long-leg cast immobilization in extension if the extensor mechanism is intact. |
| Relative Contraindications | Severe Medical Comorbidities | Rare in this adolescent demographic, but prohibitive anesthetic risks may necessitate non-operative management. |
Non-operative management is strictly reserved for Ogden Type I or carefully selected Type II fractures demonstrating less than 2 millimeters of displacement, provided the patient can perform a straight leg raise against gravity, confirming an intact extensor mechanism. These rare cases are managed with a long-leg cast or a locked hinged knee brace in full extension for 4 to 6 weeks, accompanied by serial radiographic monitoring to ensure no secondary displacement occurs as swelling subsides.
Conversely, open reduction and internal fixation (ORIF) is the gold standard for the vast majority of presenting cases. Any fracture exhibiting greater than 2 millimeters of displacement, any fracture with intra-articular extension (Ogden Type III), or any clinical presentation featuring an extensor lag demands surgical correction. Furthermore, if advanced imaging or clinical suspicion suggests the interposition of soft tissue—most notably the anterior horn of the lateral meniscus or a massive periosteal flap—closed reduction is impossible, making open surgery mandatory. The goal of surgery is not merely bony union, but the absolute anatomical restoration of the tibial plateau articular surface, the re-establishment of the precise resting length of the patellar tendon, and the rigid stabilization of the fragment to allow for early, aggressive rehabilitation.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of a successful surgical outcome. The initial evaluation relies heavily on high-quality orthogonal plain radiographs of the affected knee. While the anteroposterior (AP) view may show subtle widening of the physis or a lateralized fragment, it is the true lateral radiograph that is the workhorse of diagnostic imaging for this injury. The lateral view clearly delineates the fracture pattern, the degree of proximal and anterior displacement, the extent of comminution, and the presence of patella alta.

Observe this lateral radiograph of a 13-year-old girl with a Type III fracture. The fracture line clearly propagates proximally through the epiphysis and into the articular surface of the anterior tibial plateau. Note the proximal migration of the tubercle.

In this lateral view of a 14-year-old boy, we see a significantly displaced Type III fracture. The profound proximal migration indicates complete disruption of the medial and lateral retinacular supports alongside the primary apophyseal failure.
For all Ogden Type III fractures, or any fracture pattern exhibiting complex comminution or suspected soft tissue entrapment, a preoperative Computed Tomography (CT) scan with 3D reconstructions is considered the standard of care. The CT scan provides invaluable, high-resolution detail regarding the exact topography of the intra-articular fracture lines, guiding the surgeon in planning the trajectory of fixation screws to avoid the joint space while maximizing bone purchase. Furthermore, MRI may occasionally be indicated if there is a high suspicion of concomitant ligamentous injury or complex meniscal pathology, though it is not routinely required for standard presentations.
Patient positioning must facilitate unhindered access to the anterior knee, allow for full dynamic range of motion during the procedure, and permit seamless fluoroscopic imaging. The patient is positioned supine on a radiolucent operating table. A small bump may be placed under the ipsilateral hip to correct for natural external rotation of the lower extremity, ensuring the patella points directly toward the ceiling. The entire lower extremity, from the proximal thigh to the toes, is prepped and draped free using a sterile extremity drape. This free-draping is absolutely critical; the surgeon must be able to freely flex and extend the knee joint, as dynamic manipulation of the extensor mechanism is the primary maneuver required to achieve anatomical reduction.
A pneumatic tourniquet is applied to the proximal thigh. While the tourniquet ensures a bloodless surgical field—which is vital for identifying interposed soft tissues and achieving precise articular reduction—the surgeon must remain acutely aware of its mechanical effects. Tourniquet inflation can tether the quadriceps muscle belly, slightly increasing the tension on the extensor mechanism and making the distal translation of the avulsed fragment more challenging. Therefore, the tourniquet is typically inflated to a standard pediatric or adolescent pressure (e.g., 250 mmHg) only after the leg has been elevated and exsanguinated, and the surgeon must be prepared to temporarily deflate it if extreme difficulty is encountered during the reduction phase. The fluoroscopic C-arm is positioned on the contralateral side of the table, draped sterilely, and brought in perpendicular to the operative field to provide rapid, orthogonal AP and lateral views without requiring repositioning of the patient's leg.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution requires a blend of precise soft tissue handling, strategic mechanical maneuvering, and rigid biomechanical fixation.
Incision and Deep Dissection
We utilize a lateral parapatellar approach rather than a direct midline incision. The incision begins at the level of the mid-patella, approximately 1-2 centimeters lateral to the lateral border of the patellar tendon, and extends distally to a point 2-3 centimeters distal to the anticipated distal extent of the fracture bed on the anterior tibial crest. This lateralized approach offers two distinct advantages: first, it provides direct, orthogonal access to the typically laterally displaced tubercle fragment; second, and most importantly, it significantly minimizes the risk of iatrogenic transection of the infrapatellar branch of the saphenous nerve, which predominantly crosses the midline from medial to lateral.
Deep dissection is carried sharply through the subcutaneous fat to the level of the deep fascia. The deep fascia is incised longitudinally, directly in line with the skin incision. Upon breaching the fascia, the surgeon will immediately encounter a substantial, often organized fracture hematoma.

Intraoperative view demonstrating the initial exposure. The fascial layer has been incised, revealing the underlying hemorrhagic bursitis and the proximal extent of the avulsed tibial tuberosity.
This hematoma must be meticulously evacuated using suction and lap sponges. Clearing this field is paramount not only for visualization but also to decompress the anterior compartment locally. As the hematoma is cleared, the surgeon will identify the avulsed bony fragment, the attached patellar tendon, and typically, a massive, thick flap of torn periosteum that has been stripped from the anterior tibia.
Prophylactic Fasciotomy and Joint Inspection
Given the high incidence of acute anterior compartment syndrome secondary to bleeding from the anterior tibial recurrent artery, a prophylactic anterior compartment fasciotomy is strongly recommended. Using a scalpel or electrocautery, the deep investing fascia of the anterior compartment is released longitudinally from the level of the fracture bed extending distally for several centimeters. This simple, rapid step drastically reduces the risk of postoperative compartment syndrome and adds negligible morbidity to the procedure.
For Ogden Type III fractures, direct inspection of the knee joint is mandatory. The fracture gap itself often provides a window into the anterior compartment of the knee.
Here, the fracture fragment is gently retracted anteriorly and proximally. This allows direct visualization into the joint space to inspect for meniscal entrapment, a common block to anatomical reduction in Type III injuries.
The surgeon must meticulously probe the anterior horn of the lateral and medial menisci. If the meniscus is found to be avulsed or interposed within the fracture site, it must be gently extracted using a blunt nerve hook or dental pick. Failure to recognize and clear meniscal interposition will absolutely preclude an anatomical reduction and lead to catastrophic joint incongruity.
Fracture Reduction
Reduction of the tibial tuberosity is a dynamic process. The primary deforming force is the proximal pull of the quadriceps. Therefore, the first step in reduction is to fully extend the knee joint, which maximally relaxes the extensor mechanism.

This image represents a critical teaching point. This is an initial attempt at reduction visualized on fluoroscopy. While the fragment appears grossly approximated, closer inspection reveals a persistent gap and slight step-off, indicative of interposed periosteum or inadequate distal translation. This is an unacceptable reduction.
With the knee in full extension, a pointed reduction forceps (Weber clamp) is applied. One tine is placed on the proximal, superior pole of the avulsed tuberosity fragment (often requiring a small stab incision through the patellar tendon insertion), and the other tine is anchored into the intact tibial metaphysis distal to the fracture bed. Gentle, progressive compression is applied to translate the fragment distally and posteriorly into its anatomical bed.

Following the removal of interposed periosteum and the application of a pointed reduction clamp with the knee in extension, anatomical reduction is achieved. The clamp holds the fragment rigidly in place, preparing the site for provisional and definitive fixation.
The reduction must be confirmed visually, ensuring the cortical interdigitations match perfectly, and fluoroscopically, confirming the restoration of the articular surface (in Type III) and the correction of patella alta.
Internal Fixation
Once anatomical reduction is achieved and provisionally held with the reduction clamp or K-wires, definitive internal fixation is performed. The gold standard for fixation is the use of large-fragment partially threaded cancellous screws (typically 4.0mm or 4.5mm, depending on patient size).
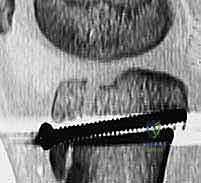
Guide wires for cannulated screws are advanced from anterior to posterior. Note the trajectory: they are directed slightly proximal to distal to remain perpendicular to the primary fracture plane and to avoid converging on the posterior neurovascular structures.
Two screws are generally utilized to provide rotational stability. The trajectory of the screws is critical; they should be directed from anterior to posterior, and slightly proximal to distal. This trajectory ensures the screws cross the physis at an angle that maximizes compression across the fracture site while minimizing the risk of the screw threads crossing into the posterior joint space or jeopardizing the popliteal artery.

The cannulated screws are advanced over the guide wires. Washers may be used if the anterior cortex of the apophysis is comminuted or soft, preventing the screw head from burying into the cartilage and losing compression.
Bicortical purchase is generally preferred for maximum biomechanical pull-out strength, but the surgeon must use a depth gauge meticulously and confirm screw length on a true lateral fluoroscopic view to ensure the screw tips do not protrude excessively past the posterior tibial cortex.
Final Verification and Closure
Following screw placement, the reduction clamp is removed. The knee is then taken through a full, dynamic range of motion under direct visualization and fluoroscopy.

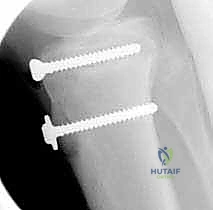
Final lateral fluoroscopic view demonstrating absolute anatomical reduction. The articular surface is perfectly congruent, the screws are of appropriate length with excellent purchase, and the patellar height is restored.
The surgeon must confirm that the fracture site remains rigidly stable during deep flexion (up to 90-120 degrees) and that there is no gapping at the anterior cortex.
Intraoperative photograph of the final construct. The screw heads are seated flush, and the massive periosteal flap is now being prepared for repair.
The final, crucial step of the deep procedure is the meticulous repair of the medial and lateral retinaculum and the torn periosteal sleeve. This is typically performed using heavy, absorbable sutures (e.g., #1 or #2 Vicryl).

The periosteum and retinaculum have been meticulously repaired over the fracture site and hardware. This biological envelope is critical for fracture healing and provides secondary stability to the extensor mechanism.
Repairing this periosteal sleeve not only aids in biological healing but acts as a tension band, neutralizing anterior tensile forces and providing significant supplementary biomechanical stability to the screw construct. The wound is then irrigated copiously, and the subcutaneous tissues and skin are closed in a standard layered fashion.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following the operative management of tibial tuberosity fractures can and do occur. The surgeon must be hyper-vigilant in the immediate postoperative period and maintain long-term follow-up to monitor for growth disturbances.
| Complication | Estimated Incidence | Pathophysiology & Clinical Presentation | Salvage & Management Strategy |
|---|---|---|---|
| Acute Compartment Syndrome | 10 - 20% | Laceration of the anterior tibial recurrent artery causes rapid hemorrhage into the anterior compartment. Presents as disproportionate pain, pain on passive toe flexion, and tense compartments. | Immediate surgical emergency. Requires emergent four-compartment fasciotomy. Prophylactic anterior release during initial ORIF is highly recommended to prevent this. |
| Genu Recurvatum | 2 - 5% | Premature closure of the anterior aspect of the proximal tibial physis while the posterior physis continues to grow. Results in a progressive hyperextension deformity of the knee. | Mild cases are observed. Severe progressive deformity requires corrective proximal tibial opening-wedge osteotomy after skeletal maturity. |
| Symptomatic Hardware | 30 - 50% | The anterior proximal tibia has minimal subcutaneous fat. Screw heads frequently become prominent, causing localized bursitis and pain when kneeling. | Hardware removal (HWR) after complete radiographic union (typically 6-12 months post-op). HWR is the most common secondary procedure. |
| Loss of Reduction / Fixation Failure | < 2% | Occurs due to inadequate initial fixation, premature weight-bearing, or unrecognized extreme comminution. Presents as recurrent extensor lag. | Revision ORIF. May require augmentation with tension band wiring or heavy suture anchors if bone stock is heavily compromised. |
| Infrapatellar Neuroma | 5 - 10% | Iatrogenic transection of the infrapatellar branch of the saphenous nerve during the surgical approach. Presents as localized neuropathic pain, Tinel's sign, or numbness. | Initial management with gabapentinoids and localized steroid injections. Refractory cases may require surgical exploration, neuroma excision, and burying the nerve stump into muscle. |
