Masterclass: Precision Internal Fixation of Hallux Sesamoid Fractures
Key Takeaway
This masterclass guides fellows through internal fixation of hallux sesamoid fractures. We cover detailed anatomy, preoperative planning, and step-by-step intraoperative execution using both open grafting/suture and percutaneous screw techniques. Emphasis is placed on meticulous dissection, fluoroscopic guidance, and managing potential complications for successful outcomes in these challenging foot injuries.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater. Today, we are undertaking a rigorous masterclass on a fascinating, complex, and often vexing pathology: the precision internal fixation of hallux sesamoid fractures. These small, specialized ossicles are absolutely critical to the biomechanics of the first ray. When fractured, they become a source of profound pain and devastating disability, particularly in the high-demand athletic population. Historically, the orthopedic community leaned heavily toward sesamoid excision; however, our contemporary goal is the meticulous anatomical restoration of their integrity and function to preserve the biomechanical fulcrum of the forefoot.
The pathogenesis of sesamoid fractures dictates our surgical decision-making and is broadly categorized into acute traumatic events and chronic stress phenomena. Acute trauma is frequently observed in "turf toe" variants, typically involving a violent, excessive hyperextension of the first metatarsophalangeal (MTP) joint under an axial load. This mechanism can precipitate a trans-sesamoidal fracture-dislocation of the first MTP joint, often accompanied by catastrophic disruption of the plantar joint capsule and the intersesamoid ligamentous complex. These injuries demand immediate recognition, as the displacement of the fracture fragments severely compromises the flexor hallucis brevis (FHB) mechanism.
Conversely, chronic overuse resulting in stress fractures presents a more insidious clinical picture. This etiology is overwhelmingly more common and often manifests with pain and localized edema that gradually escalates over weeks, months, or even years. Patients, typically endurance athletes, ballet dancers, or gymnasts, frequently cannot pinpoint a singular traumatic event. The persistent microtrauma exceeds the bone's remodeling capacity, leading to structural failure. The challenge of healing in these chronic scenarios is immense; they often fail to unite without surgical intervention due to the relentless shear forces between fracture fragments and the insidious accumulation of avascular, necrotic fibrous tissue at the nonunion site, which acts as a biologic barrier to osteogenesis.
Furthermore, we must critically evaluate underlying foot deformities as potent predisposing factors. A rigid cavus foot deformity, characterized by a steep, plantar-flexed first ray, inevitably concentrates immense ground reaction forces directly onto the sesamoid pedestal, exponentially increasing the risk of stress fractures. Similarly, in the presence of hallux valgus, the varus subluxation of the first metatarsal shifts the weight-bearing axis, concentrating pressure almost exclusively on the medial sesamoid. 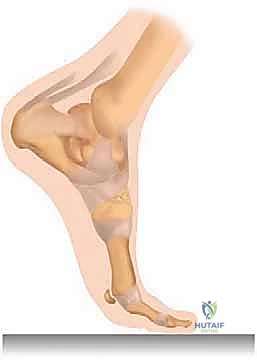 This persistent eccentric loading and fragment displacement in the setting of hallux deviation can thwart healing even with rigid immobilization.
This persistent eccentric loading and fragment displacement in the setting of hallux deviation can thwart healing even with rigid immobilization. 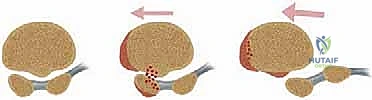 If the encompassing hallux valgus deformity is not concurrently addressed, isolated sesamoid excision or even fixation may fail, or worse, exacerbate the coronal plane deformity by further destabilizing the intrinsic muscular balance.
If the encompassing hallux valgus deformity is not concurrently addressed, isolated sesamoid excision or even fixation may fail, or worse, exacerbate the coronal plane deformity by further destabilizing the intrinsic muscular balance.
Detailed Surgical Anatomy and Biomechanics
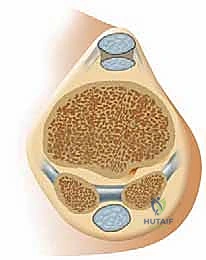
Before a scalpel ever touches the skin, a profound, three-dimensional understanding of the hallux sesamoid complex is paramount for any foot and ankle surgeon. The hallux sesamoids typically measure 13.5 ± 3 mm in longitudinal length, with men generally exhibiting larger ossicles than women. Morphologically, the medial (tibial) sesamoid is larger and elliptically shaped, whereas the lateral (fibular) sesamoid tends to be smaller and more circular. It is imperative to distinguish a true fracture from a bipartite sesamoid—a congenital failure of complete ossification resulting in two or more distinct bony segments connected by robust, radiolucent fibrocartilaginous tissue. Bipartite sesamoids are overwhelmingly more common than tripartite variants and are bilateral in only 25% of cases. Crucially, stress fractures frequently occur directly through this vulnerable fibrocartilaginous synchondrosis in a bipartite sesamoid, creating a diagnostic conundrum that mimics the native bipartite morphology.
The tendinous investment of these ossicles is intricate. The sesamoids are intimately embedded within the tendinous slips of the flexor hallucis brevis (FHB) muscle. The medial and lateral heads of the FHB encapsulate their respective sesamoids before inserting into the plantar base of the proximal phalanx. Spanning the void between them is the robust intersesamoid ligament, which, along with the plantar plate, forms a stable, dynamic hammock—the sesamoid pedestal. This complex acts as a critical biomechanical fulcrum for both the FHB and the flexor hallucis longus (FHL) tendon, which glides smoothly between them.
Biomechanically, the sesamoids function analogously to the patella in the knee. By elevating the first metatarsal head and displacing the flexor tendons away from the joint center of rotation, they significantly increase the mechanical lever arm and the push-off power of the hallux during the terminal stance phase of gait. They are shock absorbers of the highest order, managing the transfer of 50% or more of total body weight over the first ray during normal ambulation, a figure that multiplies exponentially during running or jumping. Total or even partial excision of a sesamoid effectively decreases the preloading of the metatarsal, shifting the mechanical burden laterally to the lesser metatarsals (risking transfer metatarsalgia) and precipitously reducing the plantarflexion power of the first ray.
The vascular anatomy of the sesamoids is notoriously tenuous and highly variable, dictating their propensity for delayed union and avascular necrosis (AVN). The primary arterial supply typically arises from the posterior tibial artery, which branches into the medial plantar artery. This vessel yields a major branch that pierces the plantar cortex of the proximal pole of the sesamoid. However, significant anatomical redundancy and variation exist; the lateral plantar artery or the dorsal arterial arch can contribute substantially. Small accessory vessels also penetrate the non-articular plantar surface and the capsular attachments. Because the proximal pole relies heavily on a single retrograde intraosseous vessel in many individuals, transverse fractures critically disrupt this supply, rendering the proximal fragment highly susceptible to ischemic necrosis.
Exhaustive Indications and Contraindications
A meticulous clinical assessment is the cornerstone of differentiating sesamoid fractures from a myriad of other first ray pathologies. The patient history must rigorously detail the onset of pain, specific athletic activities, and prior conservative modalities attempted. Physical examination requires precise palpation of the plantar aspect of the first MTP joint to isolate tenderness over the medial or lateral sesamoid.  Passive hyperextension of the hallux will classically elicit sharp pain as the sesamoids are drawn distally under the metatarsal head. Furthermore, a comprehensive evaluation for underlying foot deformities—such as hallux valgus, metatarsus primus varus, or a rigid cavus foot—is non-negotiable, as these biomechanical faults must be corrected to prevent hardware failure or recurrent fracture.
Passive hyperextension of the hallux will classically elicit sharp pain as the sesamoids are drawn distally under the metatarsal head. Furthermore, a comprehensive evaluation for underlying foot deformities—such as hallux valgus, metatarsus primus varus, or a rigid cavus foot—is non-negotiable, as these biomechanical faults must be corrected to prevent hardware failure or recurrent fracture. 

The decision to proceed with internal fixation rather than excision or continued non-operative management rests on strict criteria. Internal fixation is primarily indicated for acute, displaced transverse or oblique fractures in young, active patients, and for chronic stress fractures or symptomatic nonunions that have definitively failed a minimum of 3 to 6 months of rigorous conservative management (including strict offloading, boot immobilization, and orthotics). The goal is joint preservation and maintenance of the FHB lever arm. Joint-preserving fixation is particularly favored in high-level athletes where the loss of push-off strength associated with sesamoidectomy would be career-altering.
Conversely, there are definitive contraindications to internal fixation. Severe comminution where the sesamoid is shattered into non-reconstructable fragments necessitates partial or total excision. Advanced avascular necrosis of the entire sesamoid, evidenced by fragmentation and sclerosis on imaging, renders fixation futile. Furthermore, severe localized osteopenia, active soft tissue or bone infection, and patients with profound peripheral neuropathy (e.g., Charcot arthropathy) are absolute contraindications. In cases of severe osteoarthritis of the sesamoid-metatarsal articulation, fixation alone will not relieve pain, and excision or arthrodesis may be required.
Indications and Contraindications for Sesamoid Fixation
| Category | Specific Clinical Scenarios | Rationale / Considerations |
|---|---|---|
| Absolute Indications | Displaced acute transverse fractures in athletes; Symptomatic nonunions failing >6 months conservative care. | Preserves biomechanical fulcrum; prevents loss of push-off power and transfer metatarsalgia. |
| Relative Indications | Minimally displaced fractures in highly demanding patients; Fractures through a bipartite synchondrosis. | Fixation accelerates return to play compared to prolonged immobilization. |
| Relative Contraindications | Moderate osteopenia; Concomitant uncorrected severe hallux valgus. | Poor screw purchase; eccentric loading will lead to fixation failure if deformity is ignored. |
| Absolute Contraindications | Severe comminution; Advanced AVN with fragmentation; Active infection; Severe MTP joint osteoarthritis. | Bone cannot hold hardware; dead bone will not heal; pain source is arthritic, not just mechanical instability. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced imaging is our critical window into the complex bony architecture of the sesamoid and is foundational for pre-operative templating. Standard weight-bearing dorsoplantar and lateral radiographs are mandatory for assessing overall foot alignment, hallux valgus angles, and the talo-first metatarsal angle. However, specialized oblique and tangential ("skyline") views are essential for evaluating the articular surface and the degree of fracture displacement in the coronal plane. 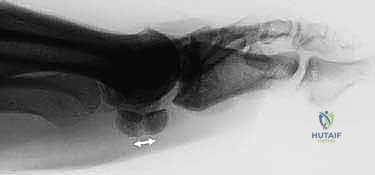 While contralateral films can provide a baseline for suspected bipartite sesamoids, a unilateral bipartite appearance does not preclude a fracture on the symptomatic side.
While contralateral films can provide a baseline for suspected bipartite sesamoids, a unilateral bipartite appearance does not preclude a fracture on the symptomatic side.
When standard radiography is equivocal, Computed Tomography (CT) is the gold standard for defining fracture morphology. High-resolution, fine-cut (0.5mm) longitudinal and coronal CT scans of the forefoot exquisitely demonstrate stress fracture lines, the extent of sclerosis at a nonunion site, and the presence of cystic changes or fragmentation that might alter the surgical plan from fixation to excision. 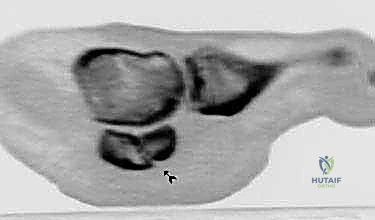 Magnetic Resonance Imaging (MRI) is utilized primarily to assess the viability of the bone marrow (ruling out advanced AVN), to detect early stress reactions before fracture lines are visible on CT, and to evaluate the integrity of the plantar plate and intersesamoid ligament.
Magnetic Resonance Imaging (MRI) is utilized primarily to assess the viability of the bone marrow (ruling out advanced AVN), to detect early stress reactions before fracture lines are visible on CT, and to evaluate the integrity of the plantar plate and intersesamoid ligament. 

Pre-operative templating involves selecting the appropriate fixation modality based on the CT findings. For transverse fractures with adequate bone stock, 1.5 mm to 2.0 mm headless compression screws are typically templated. The surgeon must measure the anticipated screw length to ensure it engages the distal cortex without protruding into the articular surface or the distal soft tissues. In cases of smaller proximal fragments or osteopenic bone, templating for a suture cerclage or tension band construct using high-tensile strength non-absorbable tape is planned.
Patient positioning is critical for optimal surgical access and fluoroscopic visualization. The patient is positioned supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the lower extremity, bringing the medial aspect of the foot directly toward the surgeon. A well-padded thigh or calf tourniquet is applied to ensure a bloodless field, which is vital given the intricate neurovascular anatomy of the plantar forefoot. The mini-C-arm fluoroscopy unit is brought in from the contralateral side, positioned to allow seamless transition between AP, lateral, and axial skyline views without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach to the hallux sesamoids requires meticulous soft tissue handling. For the medial sesamoid, a medial longitudinal incision is preferred over a direct plantar approach to avoid a painful, weight-bearing plantar cicatrix. The incision is centered over the medial eminence, extending from the mid-diaphysis of the first metatarsal to the mid-diaphysis of the proximal phalanx.  Careful blunt dissection is utilized to identify and protect the medial proper plantar digital nerve, which frequently courses dangerously close to the plantar-medial border of the sesamoid. Retraction of this nerve is performed with silastic loops, avoiding excessive tension that could induce a neuropraxia.
Careful blunt dissection is utilized to identify and protect the medial proper plantar digital nerve, which frequently courses dangerously close to the plantar-medial border of the sesamoid. Retraction of this nerve is performed with silastic loops, avoiding excessive tension that could induce a neuropraxia.
Once the neurovascular structures are protected, a longitudinal arthrotomy is performed through the medial capsule and the medial head of the FHB. The capsule is sharply elevated off the medial aspect of the sesamoid to expose the fracture site. In chronic nonunions, the fracture gap is typically filled with dense, avascular fibrous tissue. 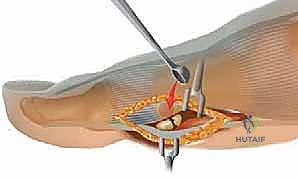 This fibrous interface must be aggressively debrided using fine curettes and a surgical scalpel until healthy, punctate bleeding bone is encountered on both the proximal and distal fragments.
This fibrous interface must be aggressively debrided using fine curettes and a surgical scalpel until healthy, punctate bleeding bone is encountered on both the proximal and distal fragments. 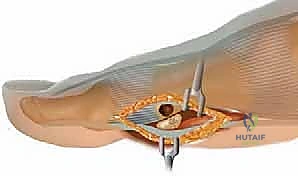 A 1.0mm drill bit or K-wire can be used to perform multiple micro-drill holes (osteostixis) into the sclerotic bone ends to stimulate local angiogenesis and osteoprogenitor cell migration.
A 1.0mm drill bit or K-wire can be used to perform multiple micro-drill holes (osteostixis) into the sclerotic bone ends to stimulate local angiogenesis and osteoprogenitor cell migration.  If a significant bone void is created during debridement, autologous cancellous bone graft, typically harvested from the distal tibia or calcaneus, is packed into the defect.
If a significant bone void is created during debridement, autologous cancellous bone graft, typically harvested from the distal tibia or calcaneus, is packed into the defect. 
Anatomical reduction is achieved using a specialized, small pointed reduction clamp. The clamp tines are placed on the proximal and distal poles of the sesamoid, and gentle compression is applied.  The reduction is provisionally held with a 1.0 mm or 1.2 mm Kirschner wire driven from distal to proximal. Fluoroscopy in the AP, lateral, and skyline planes is mandatory at this stage to confirm absolute anatomic reduction of the articular surface. Step-offs here will inevitably lead to rapid, debilitating sesamoid-metatarsal osteoarthritis.
The reduction is provisionally held with a 1.0 mm or 1.2 mm Kirschner wire driven from distal to proximal. Fluoroscopy in the AP, lateral, and skyline planes is mandatory at this stage to confirm absolute anatomic reduction of the articular surface. Step-offs here will inevitably lead to rapid, debilitating sesamoid-metatarsal osteoarthritis.
For definitive fixation, a headless compression screw technique is most frequently employed. A guide wire for a 1.5 mm, 1.7 mm, or 2.0 mm headless screw is introduced parallel to the provisional K-wire.  The screw length is measured, and the near cortex is over-drilled if required by the specific system. The headless compression screw is then advanced under fluoroscopic guidance until the trailing threads are completely buried beneath the chondral surface of the distal pole, ensuring robust interfragmentary compression.
The screw length is measured, and the near cortex is over-drilled if required by the specific system. The headless compression screw is then advanced under fluoroscopic guidance until the trailing threads are completely buried beneath the chondral surface of the distal pole, ensuring robust interfragmentary compression.  Alternatively, in cases of extreme comminution or poor bone quality where a screw might toggle or split the fragment, a figure-of-eight tension band construct using high-strength suture tape passed through drill holes in the proximal and distal fragments provides excellent, low-profile compression.
Alternatively, in cases of extreme comminution or poor bone quality where a screw might toggle or split the fragment, a figure-of-eight tension band construct using high-strength suture tape passed through drill holes in the proximal and distal fragments provides excellent, low-profile compression. 

 Following fixation, the capsule and FHB expansion are meticulously repaired with absorbable sutures to restore the soft tissue envelope.
Following fixation, the capsule and FHB expansion are meticulously repaired with absorbable sutures to restore the soft tissue envelope.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, internal fixation of hallux sesamoid fractures carries a distinct complication profile due to the challenging biological and biomechanical environment of the first ray. Nonunion or delayed union remains the most formidable complication, occurring in approximately 10-15% of cases. This is primarily attributed to inadequate resection of the fibrous nonunion site, failure to achieve rigid interfragmentary compression, or the inherently precarious blood supply to the proximal pole. When a symptomatic nonunion persists despite prolonged immobilization and bone stimulator use, revision surgery is mandated.
Avascular necrosis (AVN) of the proximal fragment is another devastating complication, often interlinked with nonunion. The surgical approach itself, if overly aggressive in stripping the plantar capsular attachments, can inadvertently devascularize the bone. If AVN progresses to structural collapse and fragmentation, the hardware will inevitably fail. Iatrogenic nerve injury to the proper plantar digital nerve can result in a painful neuroma, which is often more debilitating than the original fracture. Careful retraction and avoidance of aggressive electrocautery near the nerve are preventative imperatives.
Hardware complications, including screw back-out, breakage, or prominence causing localized plantar irritation, occur in up to 5% of patients. Because the sesamoid is subjected to massive cyclic loading, even headless screws can migrate if union is delayed. Finally, failure to address concomitant foot deformities, or iatrogenic disruption of the intrinsic musculature during surgery, can lead to progressive hallux valgus or hallux varus. Salvage management for failed fixation, advanced AVN, or intractable nonunion invariably involves progression to a partial or total sesamoidectomy. While sesamoidectomy resolves the osseous pain, the surgeon must meticulously repair the FHB tendon defect to prevent devastating iatrogenic toe deformities.
Complications in Sesamoid Fixation and Salvage Strategies
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Nonunion / Delayed Union | 10% - 15% | Inadequate debridement; Poor compression; Smoking; Poor vascularity. | Revision fixation with autologous bone grafting; Bone stimulator; Partial excision. |
| Avascular Necrosis (AVN) | 5% - 10% | Disruption of retrograde proximal pole blood supply; Excessive soft tissue stripping. | Total or partial sesamoidectomy with rigorous FHB tendon repair. |
| Plantar Digital Neuroma | 2% - 5% | Iatrogenic traction injury; Entrapment in scar tissue; Direct laceration. | Conservative (injections, orthotics); Surgical neurolysis or neurectomy and burying into muscle. |
| Hardware Failure / Prominence | 3% - 5% | Osteopenic bone; Premature weight-bearing; Screw too long. | Hardware removal after union; Revision to suture tape construct if nonunion is present. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following sesamoid internal fixation must be strictly phased to protect the fragile osteosynthesis while mitigating the stiffness inherent to first MTP joint surgery. Phase 1 (Weeks 0-2) is focused entirely on wound healing, edema control, and absolute protection of the fixation. The patient is placed in a well-padded, rigid short-leg cast or a locked controlled-ankle-motion (CAM) boot and remains strictly non-weight-bearing on crutches. Elevation and cryotherapy are aggressively employed to minimize swelling, which can compromise the surgical incision.
Phase 2 (Weeks 2-6) transitions the patient into protected, partial weight-bearing. Sutures are typically removed at the two-week mark. The patient remains in the rigid CAM boot but is allowed to begin heel-touch to partial weight-bearing with crutches, strictly avoiding any roll-off or push-off through the forefoot. During this phase, gentle, passive range of motion exercises for the first MTP joint are initiated to prevent capsular adhesions, keeping the motion strictly within a pain-free arc. Active plantarflexion is generally restricted to prevent excessive pull by the FHB on the healing fracture.
Phase 3 (Weeks 6-12) marks the progression to full weight-bearing and active rehabilitation. Radiographic confirmation of bridging trabecular bone across the fracture site is required before advancing. The patient is transitioned from the boot to a stiff-soled athletic shoe, often modified with a carbon fiber footplate or a custom orthotic featuring a sesamoid cutout (dancer's pad) to offload the surgical site. Physical therapy escalates to include active MTP joint range of motion, intrinsic foot muscle strengthening (e.g., towel curls, marble pickups), and progressive proprioceptive training.
Phase 4 (Months 3-6) is the return-to-sport phase. This is highly individualized and depends heavily on the patient's athletic demands. Running, jumping, and pivoting activities are gradually reintroduced under the supervision of a physical therapist. High-impact athletes may require 4 to 6 months before achieving maximal medical improvement and a full, unrestricted return to play. Long-term maintenance often involves the continued use of custom orthotics to permanently alter the biomechanical load distribution across the first ray, thereby protecting the reconstructed sesamoid from future stress failure.
Summary of Landmark Literature and Clinical Guidelines
The evolution of treatment for hallux sesamoid fractures represents a significant paradigm shift in orthopedic foot and ankle surgery, moving away from the historic default of excision toward joint-preserving internal fixation. Early landmark literature, notably the foundational work by Anderson and colleagues, highlighted the significant biomechanical detriments of sesamoidectomy, documenting unacceptably high rates of post-operative hallux valgus, hallux varus, and devastating loss of push-off strength in elite athletes. This catalyzed the pursuit of osteosynthesis techniques.
Subsequent anatomical studies by Biedert and others definitively mapped the precarious vascular supply of the sesamoid complex. Their research underscored the vulnerability of the proximal pole to avascular necrosis following transverse fractures, providing the biological rationale for why prolonged conservative management of stress fractures so frequently fails. This literature established the modern clinical guideline that early surgical intervention—specifically meticulous debridement and rigid compression—is biologically necessary to overcome the avascular fibrous nonunion that plagues these injuries.
More recent systematic reviews and cohort studies focusing on athletic populations have demonstrated superior clinical outcomes with internal fixation compared to excision. Modern techniques utilizing headless compression screws or high-tensile suture constructs yield union rates exceeding 85-90% in properly selected patients. Notably, the return-to-play rates at the pre-injury level of competition are significantly higher in the fixation cohorts. Current clinical guidelines advocate that while sesamoidectomy remains a viable salvage procedure for severely comminuted or necrotic bones, anatomical reduction and internal fixation should be considered the gold standard and first-line surgical treatment for displaced acute fractures and recalcitrant stress fractures in the active patient population, preserving the indispensable biomechanical engine of the first ray.
