Masterclass: Surgical Correction of Equinocavovarus Foot Deformity

Key Takeaway
This masterclass provides an exhaustive, real-time walkthrough of equinocavovarus foot deformity correction. We cover precise patient positioning, detailed surgical anatomy, step-by-step intraoperative execution, and critical pearls for managing cavus, varus, and equinus components. Fellows will gain insights into soft tissue releases, Achilles lengthening, and foundational principles for bony correction, ensuring optimal outcomes and complication avoidance.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to this masterclass on one of the most structurally complex and functionally debilitating conditions encountered in reconstructive foot and ankle surgery: the pes equinocavovarus deformity. This chapter serves as a definitive guide to understanding, deconstructing, and surgically correcting a pathology that has challenged orthopedic surgeons for over a century. Far from being a mere cosmetic anomaly, the equinocavovarus foot represents a profound biomechanical collapse driven by insidious neuromuscular imbalances. As historical luminaries like Tubby and Jones eloquently described, patients typically present with a constellation of symptoms including recurrent lateral ankle instability, a rigidly hollowed medial longitudinal arch, an inverted heel, and a taut, overactive tibialis anterior tendon.

The epidemiology of pes equinocavovarus is inextricably linked to its underlying etiology, which is predominantly neuromuscular. Charcot-Marie-Tooth (CMT) disease, particularly Type 1A involving the PMP22 gene duplication, remains the most common culprit, accounting for a vast majority of bilateral, progressive cavovarus deformities. However, the differential diagnosis must remain broad. Orthopedic surgeons must maintain a high index of suspicion for other neurological drivers such as poliomyelitis, spinal dysraphism (tethered cord, spina bifida), cerebral palsy, cerebrovascular accidents, and post-traumatic sciatic or peroneal nerve injuries. Idiopathic presentations do occur, but they are increasingly rare as our diagnostic modalities, particularly genetic testing and electromyography, become more sophisticated.

Understanding the basic pathogenesis is paramount to achieving successful, long-lasting surgical correction. The deformity is fundamentally a manifestation of muscle imbalance—a relentless tug-of-war between the intrinsic and extrinsic musculature of the foot and ankle. When agonist-antagonist pairings lose their equilibrium, the foot morphs into a rigid, non-shock-absorbing lever. This leads to profound functional deficits, including devastating lateral column overload, recurrent stress fractures, and debilitating plantar ulcerations. Our goal as reconstructive surgeons is not merely to create a plantigrade foot, but to restore dynamic balance, preserve joint longevity, and optimize the patient’s ambulatory capacity.
To effectively demystify the cavovarus foot, we must abandon a monolithic view of the deformity and instead approach it as a multi-planar, multi-apical structural failure. The surgical management of equinocavovarus is an exercise in meticulous, staged reconstruction. It is an "a la carte" endeavor where soft tissue releases, tendon transfers, corrective osteotomies, and selective arthrodeses are combined in a highly individualized manner. In the subsequent sections, we will dissect the anatomy, biomechanics, and step-by-operative-step surgical techniques required to master this formidable orthopedic challenge.
Detailed Surgical Anatomy and Biomechanics
Structural Deformity and Joint Kinematics
The pes equinocavovarus foot is a complex, three-dimensional deformity that requires a thorough understanding of normal and pathologic foot kinematics. The deformity can be broken down into distinct anatomical components, beginning with the equinus contracture of the ankle. This limited dorsiflexion is typically driven by a contracted Achilles tendon—involving either the gastrocnemius alone or the entire triceps surae complex—or by an acquired horizontal orientation of the talus within the ankle mortise. This equinus forces the patient into obligate toe-walking or induces compensatory genu recurvatum during the stance phase of gait.

Moving distally, the hindfoot varus is a hallmark of the deformity. The calcaneus is rigidly or flexibly inverted beneath the talus. Biomechanically, when the subtalar joint is locked in varus, the transverse tarsal joints (talonavicular and calcaneocuboid) become non-parallel and rigidly locked. This prevents the normal shock-absorbing pronation that should occur during early stance phase. Over time, this chronic varus positioning leads to external rotation of the talus, retraction of the lateral malleolus, and asymmetric wear of the ankle joint, predisposing the patient to varus ankle osteoarthritis.

The midfoot and forefoot exhibit equally profound alterations. The Chopart joint often demonstrates a medial subluxation of the navicular and cuboid, contributing to the adducted and supinated appearance of the midfoot. The hallmark of the medial column deformity is the rigidly plantarflexed first metatarsal. This plantarflexed first ray acts as a "kickstand," prematurely striking the ground and driving the hindfoot into a compensatory varus position. Concurrently, the lesser toes often develop clawing—hyperextension at the metatarsophalangeal (MTP) joints and flexion at the interphalangeal (IP) joints—further depressing the metatarsal heads and exacerbating the cavus arch.
The Muscle Imbalance Theory
The structural deformities detailed above do not occur in a vacuum; they are the direct consequence of specific, predictable muscle imbalances. The classic paradigm, particularly in CMT, involves the selective weakness of the tibialis anterior and the peroneus brevis muscles. The tibialis anterior is the primary dorsiflexor of the ankle and the first ray. When it weakens, its antagonist, the peroneus longus, acts unopposed. The peroneus longus forcefully plantarflexes the first metatarsal, creating the primary forefoot-driven cavus deformity.

Simultaneously, the weakness of the peroneus brevis—the primary evertor of the hindfoot—leaves the tibialis posterior acting without opposition. The overactive tibialis posterior relentlessly pulls the hindfoot into a varus alignment. While the peroneus longus is a strong muscle, its insertion on the base of the first metatarsal and medial cuneiform means its primary vector is forefoot plantarflexion; it has insufficient leverage to counteract the hindfoot varus driven by the tibialis posterior.

This extrinsic imbalance is further compounded by intrinsic muscle failure. As the intrinsic muscles (lumbricals and interossei) weaken, they fail to flex the MTP joints and extend the IP joints. The long toe extensors (extensor digitorum longus and extensor hallucis longus) are recruited to assist the failing tibialis anterior in ankle dorsiflexion. This overactivity of the extrinsic extensors hyperextends the MTP joints, while the unresisted extrinsic flexors (flexor digitorum longus) curl the IP joints, resulting in rigid claw toes. This dynamic interplay creates a vicious cycle of progressive structural collapse.
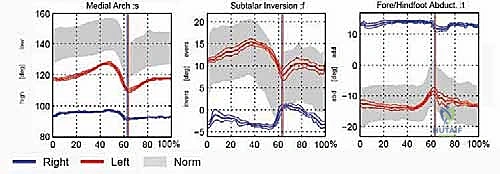
Dynamic Gait Implications
The static deformities of equinocavovarus translate into severe dynamic dysfunction during the gait cycle. During the stance phase, initial contact is frequently made with the forefoot or lateral border rather than the heel, owing to the equinus contracture. The locked transverse tarsal joint prevents normal pronation, meaning the foot cannot absorb the impact of heel strike. Consequently, ground reaction forces are abnormally transmitted up the kinetic chain, leading to stress fractures of the fifth metatarsal, lateral ankle instability, and compensatory knee and hip pathology.
The progression of the stance phase is severely hampered. The main load is concentrated on the first and fifth metatarsal heads, frequently resulting in intractable, painful callosities or neurotrophic ulcerations. Roll-off movement is limited due to the rigid midfoot and equinus ankle, creating an internal rotation moment as the patient rolls over the lateral border of the foot. Furthermore, the clawed toes fail to participate in load-bearing, depriving the foot of its normal push-off mechanics.

During the swing phase, the primary issue is foot drop resulting from tibialis anterior weakness. The patient struggles with foot clearance, leading to a compensatory "steppage gait" characterized by exaggerated hip and knee flexion. The inhibited subtalar pronation and varus tilt can cause medial impingement between the talus and the medial malleolus. Over time, the medially migrating navicular can impinge on the talar neck, leading to dorsal osteophyte formation that further mechanically blocks ankle dorsiflexion.
Exhaustive Indications and Contraindications
Surgical Decision Making
The decision to proceed with surgical reconstruction of an equinocavovarus foot is rarely straightforward and requires a nuanced understanding of the patient's functional demands, the flexibility of the deformity, and the natural history of the underlying disease. Surgery is universally indicated when conservative measures—such as custom ankle-foot orthoses (AFOs), lateral wedge insoles, and physical therapy—fail to provide a stable, plantigrade, and pain-free foot. Progressive lateral ankle instability, recurrent sprains, and the development of painful callosities or ulcerations beneath the first or fifth metatarsal heads are absolute indications for intervention.

A critical factor in surgical planning is determining whether the deformity is flexible or rigid. Flexible deformities, often seen in the earlier stages of neuromuscular disease, can typically be managed with joint-sparing procedures. These include soft-tissue releases (e.g., plantar fascia release), tendon transfers to restore dynamic balance, and extra-articular osteotomies (e.g., first metatarsal dorsiflexion osteotomy, calcaneal sliding osteotomy). The goal here is to preserve joint motion while realigning the mechanical axis of the foot.

Conversely, rigid deformities, where the joints have become fixed and arthritic changes have developed, necessitate joint-sacrificing procedures. In these advanced cases, triple arthrodesis (fusion of the subtalar, talonavicular, and calcaneocuboid joints) becomes the workhorse procedure to establish a stable, plantigrade foot. However, even in rigid cases, arthrodesis is frequently combined with tendon transfers to prevent the recurrence of deformity caused by ongoing muscle imbalance.
Contraindications and Patient Selection
While surgery offers profound functional improvement, strict contraindications must be respected to avoid disastrous outcomes. Absolute contraindications include active, untreated infection (either local or systemic) and severe peripheral vascular disease that would preclude wound healing. In patients with profound neuropathy and absent protective sensation, surgical intervention carries a high risk of Charcot neuroarthropathy or postoperative ulceration, making it a relative contraindication that requires extensive preoperative optimization and patient counseling.

Relative contraindications also include medically unstable patients who cannot tolerate prolonged anesthesia, as these reconstructive procedures are often lengthy. Furthermore, the patient's ambulatory status must be considered. In non-ambulatory patients, extensive bony reconstruction may not be warranted; instead, limited soft-tissue releases to allow for proper shoe wear or wheelchair positioning may be more appropriate. Finally, a patient's inability to comply with a strict, prolonged postoperative non-weight-bearing and rehabilitation protocol is a significant red flag that may contraindicate complex reconstruction.
Indications and Contraindications Summary
| Parameter | Indications for Surgery | Contraindications for Surgery |
|---|---|---|
| Clinical Presentation | Intractable pain, recurrent lateral ankle sprains, brace intolerance, progressive deformity. | Asymptomatic patient, well-controlled with AFOs, non-ambulatory (relative). |
| Soft Tissue Status | Intact vascular supply, healthy skin envelope, correctable muscle imbalance. | Severe peripheral arterial disease, active local infection, severe venous stasis. |
| Bony Architecture | Flexible or rigid malalignment causing abnormal focal pressure (e.g., 5th MT base ulcers). | Active Charcot neuroarthropathy (acute inflammatory phase). |
| Patient Factors | Motivated patient, capable of strict NWB compliance, realistic expectations. | Medical instability, severe psychiatric non-compliance, uncontrolled diabetes (HbA1c > 8.5%). |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and the Coleman Block Test
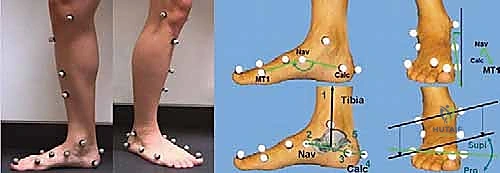
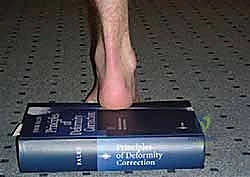
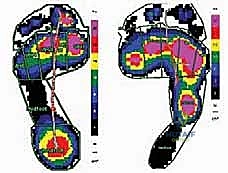
Meticulous preoperative planning is the cornerstone of successful equinocavovarus correction. The clinical examination must be exhaustive, evaluating the patient both seated and standing. In the standing position, the surgeon must assess the medial arch height, the degree of hindfoot varus, the presence of a "peek-a-boo" heel sign (visibility of the medial heel from the anterior view), and the "hello big toe" sign (visibility of the hallux from the posterior view due to severe forefoot adduction). Callosity patterns on the plantar aspect provide a roadmap of abnormal pressure distribution.

The most critical clinical assessment tool is the Coleman block test. This test determines whether the hindfoot varus is flexible and driven by a plantarflexed first ray, or if it is a rigid, structural deformity of the subtalar joint. The patient stands with their heel and lateral border of the foot on a 1-inch wooden block, allowing the first metatarsal to hang freely off the medial edge. If the hindfoot varus corrects to a neutral or valgus position, the hindfoot is flexible, and the deformity is primarily forefoot-driven. In this scenario, a first metatarsal dorsiflexion osteotomy, combined with soft tissue balancing, may suffice.

If the hindfoot varus does not correct off the block, the deformity is rigid. This indicates that structural changes have occurred within the subtalar joint complex, necessitating a calcaneal osteotomy (e.g., a Dwyer lateral closing wedge or a lateralizing calcaneal slide) or a subtalar/triple arthrodesis to achieve a plantigrade foot. Additionally, the Silfverskiöld test is mandatory to differentiate between isolated gastrocnemius tightness and a combined gastrocnemius-soleus contracture, dictating whether a gastrocnemius recession or a formal Achilles tendon lengthening is required.
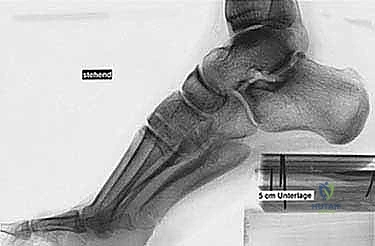
Advanced Imaging and Radiographic Templating
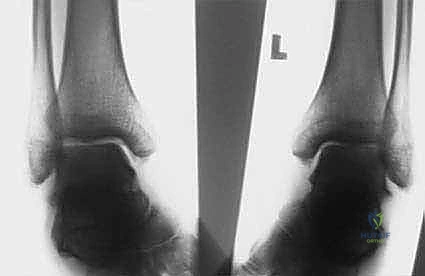
Standard weight-bearing radiographs of the foot and ankle are mandatory. On the lateral view, Meary’s angle (the angle between the longitudinal axis of the talus and the first metatarsal) is assessed; in a cavus foot, this angle intersects plantarly. The calcaneal pitch is typically increased (often >30 degrees), and Hibbs angle (intersection of the calcaneal axis and the first metatarsal axis) approaches 90 degrees in severe cases. The anteroposterior (AP) view is scrutinized for talonavicular uncoverage, calcaneocuboid alignment, and the degree of forefoot adduction.

For rigid, complex, or revision deformities, a Computed Tomography (CT) scan with 3D reconstruction is invaluable. CT imaging provides unparalleled detail regarding joint congruity, the presence of subtle tarsal coalitions, and the extent of degenerative joint disease. This is particularly crucial when planning complex midfoot osteotomies (like a Cole or Japas procedure) or when assessing the feasibility of joint-sparing procedures in the presence of suspected arthritis.

Preoperative templating, whether digital or analog, is highly recommended. The surgeon should map out the proposed osteotomy sites, calculate the exact wedge sizes needed for correction, and determine the anticipated hardware trajectories. This mental rehearsal minimizes intraoperative hesitation and ensures that the necessary fixation systems (e.g., specific staple sizes, compression screws, or specialized midfoot plates) are available in the operating theater.
Patient Positioning and Surgical Setup
Proper patient positioning is critical for facilitating the multiple exposures required in a comprehensive cavovarus reconstruction. The patient is typically placed in a supine position with a bump under the ipsilateral hip. This internally rotates the leg slightly, bringing the lateral malleolus and the lateral aspect of the foot into a more accessible anterior position. This is essential for lateral-sided procedures such as the calcaneal osteotomy, peroneus longus to brevis transfer, and lateral column lengthening.

A well-padded thigh tourniquet is applied to provide a bloodless surgical field, which is vital for identifying delicate neurovascular structures during tendon transfers and soft tissue releases. The entire lower extremity is prepped and draped free to the knee, allowing the surgeon to assess the overall mechanical axis of the leg and ankle during intraoperative correction.

Fluoroscopy must be positioned strategically, usually entering from the contralateral side of the table. The C-arm should be draped and readily available to confirm osteotomy placement, verify the correction of radiographic angles (such as restoring Meary's line), and ensure appropriate hardware position and length. A sterile bump or a radiolucent triangle is kept on the field to assist with foot positioning during lateral fluoroscopic imaging.
Step-by-Step Surgical Approach and Fixation Technique
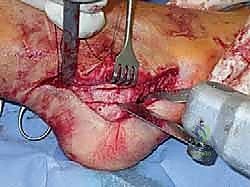
Soft Tissue Releases: The Foundation of Correction
The surgical correction of equinocavovarus is executed sequentially, typically beginning with the soft tissues and progressing to bony work. The first step in almost all cases is a radical plantar fascia release, often performed via a Steindler stripping. Through a medial incision over the calcaneal tuberosity, the plantar fascia, the origin of the abductor hallucis, the flexor digitorum brevis, and the quadratus plantae are sharply elevated off the calcaneus. This immediately reduces the longitudinal arch tension and allows for subsequent bony correction without soft tissue tethering.

Following the plantar release, the posterior equinus contracture is addressed. Based on the preoperative Silfverskiöld test, a Strayer or Baumann gastrocnemius recession is performed for isolated gastrocnemius tightness. If the contracture involves the entire triceps surae, a percutaneous or open Z-lengthening of the Achilles tendon (TAL) is executed. Care must be taken not to over-lengthen the Achilles, as a resultant calcaneocavus deformity or profound push-off weakness can be devastating.

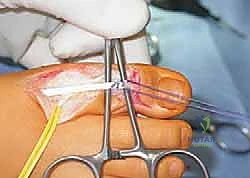
Next, the tendon transfers are prepared. To address the overactive peroneus longus and weak peroneus brevis, the peroneus longus is detached distally and tenodesed to the peroneus brevis tendon at the level of the lateral malleolus. This transfer eliminates the plantarflexing force on the first ray and augments the eversion power of the hindfoot. If foot drop is present, a transfer of the posterior tibial tendon through the interosseous membrane to the dorsum of the foot, or a split anterior tibial tendon transfer (STATT), may be required to restore balanced dorsiflexion.
Bony Reconstruction: Osteotomies and Realignment
Once the soft tissues are balanced, attention turns to the bony architecture. If the Coleman block test indicated a flexible hindfoot driven by a rigid forefoot, a first metatarsal dorsiflexion osteotomy is performed. A dorsal closing-wedge osteotomy is executed at the base of the first metatarsal, approximately 1 cm distal to the tarsometatarsal joint. The plantar cortex is preserved as a hinge if possible. The osteotomy is closed, elevating the first ray, and secured with a dorsal plate, crossed K-wires, or a compression staple.

If the hindfoot varus is rigid, a calcaneal osteotomy is mandatory. The classic Dwyer procedure involves a lateral closing-wedge osteotomy just posterior to the posterior facet of the subtalar joint. Alternatively, a lateralizing calcaneal sliding osteotomy can be performed. An oblique cut is made through the calcaneal tuberosity, and the posterior fragment is translated laterally by 10 to 15 millimeters. This lateral shift moves the insertion of the Achilles tendon laterally, creating an eversion moment arm during gait. The osteotomy is rigidly fixed with one or two large-fragment cannulated screws directed from the heel to the anterior calcaneus.

For severe midfoot cavus, midtarsal osteotomies may be required. The Cole procedure involves a dorsal closing-wedge osteotomy through the naviculocuneiform and cuboid joints, effectively shortening the dorsal column and elevating the arch. The Japas V-osteotomy is an alternative that avoids shortening by utilizing a V-shaped cut through the midfoot, with the apex proximal, allowing the distal segment to be elevated. These complex osteotomies require robust fixation, typically utilizing multiple staples or specialized midfoot locking plates.
Management of Claw Toes and Final Fixation
The final stage of the reconstruction addresses the claw toe deformities, which, if left untreated, will continue to cause dorsal shoe wear and plantar metatarsal head pain. For the hallux, a modified Jones procedure is frequently employed. The extensor hallucis longus (EHL) tendon is detached from the distal phalanx and rerouted through a drill hole in the neck of the first metatarsal. This transforms the EHL from a deforming force (hyperextending the MTP joint) into a corrective force (elevating the first metatarsal). Because the EHL is detached, the hallux IP joint must be arthrodesed using a screw or K-wire to prevent a floppy toe.
For the lesser toes, the Girdlestone-Taylor procedure (flexor-to-extensor tendon transfer) is highly effective for flexible clawing. The flexor digitorum longus is harvested plantarly, split, and routed dorsally to be sutured into the extensor hood. If the MTP joints are rigidly hyperextended, a dorsal capsulotomy and collateral ligament release (Weil osteotomy if severely contracted) are performed. Rigid IP joint flexion contractures require proximal interphalangeal (PIP) joint resection arthroplasty or arthrodesis, stabilized with longitudinal K-wires.

Before closure, the tourniquet is deflated, and meticulous hemostasis is achieved. The foot is assessed clinically and fluoroscopically to ensure a plantigrade, balanced alignment with the ankle at neutral dorsiflexion. Wound closure must be performed with minimal tension, particularly over the lateral calcaneal and dorsal midfoot incisions, as the skin in these areas is notoriously unforgiving. A bulky, well-padded posterior splint is applied with the foot held in neutral position.
Complications, Incidence Rates, and Salvage Management
Recognizing and Mitigating Surgical Risks
The surgical reconstruction of the equinocavovarus foot is a high-stakes endeavor with a substantial complication profile. The most common and devastating complications are related to wound healing. The skin over the lateral calcaneus and the dorsum of the foot has a tenuous blood supply. Aggressive retraction, excessive tourniquet time, or closing the skin under tension over prominent hardware can lead to marginal necrosis, dehiscence, and deep infection. Meticulous soft tissue handling and the use of full-thickness flaps are non-negotiable principles.

Nonunion and delayed union of osteotomies and arthrodeses are significant concerns, particularly in the midfoot and subtalar joints. The incidence of nonunion in triple arthrodesis can approach 10-15%, often exacerbated by patient non-compliance with weight-bearing restrictions, smoking, or inadequate rigid internal fixation. Careful preparation of the bony surfaces, utilizing osteotomes and curettes rather than thermal necrosis-inducing burrs, and the judicious use of autologous bone graft or orthobiologics can
Clinical & Radiographic Imaging Archive