

Comprehensive Introduction and Patho-Epidemiology
Talocalcaneal coalition represents a complex and historically challenging etiology of the rigid pediatric and adolescent flatfoot. This pathology is characterized by an abnormal union—whether osseous (synostosis), cartilaginous (synchondrosis), or fibrous (syndesmosis)—between the talus and the calcaneus. The condition fundamentally disrupts the normal kinematics of the subtalar joint, essentially tethering the hindfoot and eliminating the crucial torque-converting mechanism of the coxa pedis. This tethering not only limits inversion and eversion but also places tremendous secondary stress on the adjacent Chopart (talonavicular and calcaneocuboid) and ankle joints, leading to premature degenerative changes if left unaddressed. As orthopedic surgeons, our primary objective in managing this condition surgically is the meticulous eradication of the coalition to relieve pain, coupled with the restoration of subtalar kinematics to preserve the long-term health of the hindfoot and midfoot.
The embryological basis of a talocalcaneal coalition lies in the failure of mesenchymal segmentation and joint cavitation during the fetal period, typically between the ninth and twelfth weeks of gestation. Rather than a fusion of previously separated bones, the coalition represents a failure of the bones to ever separate fully. Epidemiologically, tarsal coalitions have an estimated prevalence of 1% to 13% in the general population, with talocalcaneal and calcaneonavicular coalitions being the most frequently encountered, comprising over 90% of all cases. Talocalcaneal coalitions specifically account for roughly 45% of all tarsal coalitions and are bilateral in up to 50% of patients. While the genetic predisposition is well-documented, often following an autosomal dominant inheritance pattern with variable penetrance, the clinical presentation is heavily dependent on the ossification timeline of the coalition itself.
Patients typically present in the second decade of life, most commonly between 12 and 16 years of age. This age of onset directly correlates with the physiological ossification of the cartilaginous or fibrous anlage into a more rigid osseous structure. As the coalition ossifies, the subtalar joint loses its remaining micro-motion, precipitating mechanical pain, recurrent ankle sprains, and the classic "peroneal spastic flatfoot." It is critical to understand that the peroneal spasm is not a true neurological spasticity, but rather a protective, reflex muscle guarding mechanism driven by the mechanoreceptors within the subtalar joint capsule attempting to prevent painful motion. The resulting sustained eversion force further exacerbates the valgus hindfoot deformity and lateral impingement.
Clinically, the hallmark of a talocalcaneal coalition is a rigid, painful planovalgus foot. Upon physical examination, the clinician will note a loss of the medial longitudinal arch, hindfoot valgus, and forefoot abduction. Crucially, the arch fails to reconstitute during the single-leg heel rise test, and the heel fails to invert, confirming the rigidity of the hindfoot complex. Palpation often reveals exquisite tenderness over the medial aspect of the hindfoot, specifically in the region of the sustentaculum tali and the middle facet, which is the most common anatomical site for these coalitions. Lateral pain over the sinus tarsi or the distal tip of the fibula may also be present, representing subfibular impingement secondary to the severe, unyielding valgus alignment.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of medial hindfoot anatomy is the absolute prerequisite for the safe and effective excision of a talocalcaneal coalition. The surgical approach requires navigation through a dense, highly critical network of tendinous, ligamentous, and neurovascular structures. The talocalcaneal coalition most frequently involves the middle facet of the subtalar joint. This facet is supported by the sustentaculum tali, a robust, medial bony projection of the calcaneus that serves as the primary anatomical landmark during surgical dissection. The middle facet is positioned just dorsal to the sustentaculum, bridging the gap to the inferior aspect of the talar neck and body.
Understanding the osteology requires recognizing the distinct facets of the subtalar joint. The posterior facet is the largest, bearing the majority of the axial load, and is located posterior to the tarsal canal. The anterior and middle facets are located anterior to the tarsal canal and are functionally linked, often sharing a single joint capsule with the talonavicular joint (the acetabulum pedis). When resecting a middle facet coalition, the surgeon must utilize the normal articular cartilage of the posterior facet (found posteriorly) and the anterior facet (found anteriorly) as the definitive boundaries for resection. Violating the posterior facet during excision is a catastrophic technical error that will inevitably lead to advanced subtalar arthritis and necessitate a subsequent salvage arthrodesis.
The soft tissue envelope of the medial hindfoot is organized into distinct layers that must be sequentially addressed. Immediately deep to the subcutaneous tissue lies the flexor retinaculum, which roofs the tarsal tunnel. From dorsal to plantar, the structures passing behind the medial malleolus are the tibialis posterior tendon, the flexor digitorum longus (FDL) tendon, the posterior tibial neurovascular bundle, and the flexor hallucis longus (FHL) tendon. The tibialis posterior is the most robust and dorsal structure, serving as the primary dynamic stabilizer of the medial arch. Just plantar to it is the FDL tendon. The FDL sheath is a critical surgical landmark; the coalition lies directly deep to the medial aspect of this sheath.
The neurovascular bundle, comprising the posterior tibial artery and the tibial nerve (which bifurcates into the medial and lateral plantar nerves within the tunnel), lies immediately posterior and slightly plantar to the FDL tendon. Protection of this bundle is the most critical safety imperative of the procedure. Retraction must be performed with meticulous care, utilizing blunt instruments and avoiding excessive tension that could induce a traction neuropraxia. Finally, the FHL tendon runs in a distinct osseous groove on the inferior surface of the sustentaculum tali. The FHL is a vital structure not only to protect but also to potentially harvest; a distally based slip of the FHL or its surrounding muscle belly can be utilized as a biological interposition graft following the resection of the coalition to prevent osseous recurrence.
Exhaustive Indications and Contraindications
The decision to proceed with surgical excision of a talocalcaneal coalition requires a nuanced synthesis of the patient's symptomatology, anatomical parameters, and response to conservative measures. Surgery is never the first-line treatment. Initial management must always include a rigorous trial of non-operative modalities, including activity modification, non-steroidal anti-inflammatory drugs (NSAIDs), custom orthoses (specifically medial heel wedging or University of California Biomechanics Laboratory [UCBL] orthoses), and occasionally immobilization in a short-leg cast or controlled ankle motion (CAM) boot to break the cycle of peroneal spasm and acute inflammation. Surgical intervention is indicated only when a comprehensive 3-to-6-month trial of these conservative measures fails to provide durable symptomatic relief.
The ideal candidate for isolated medial excision and interposition arthroplasty is a young patient (typically under 16 years of age) with a localized middle facet coalition, minimal to no degenerative changes in the posterior facet or talonavicular joint, and a neutrally aligned or only mildly valgus hindfoot. The size of the coalition is a critical determinant of success. The widely accepted "50% rule" dictates that if the coalition involves less than 50% of the total surface area of the posterior facet (as measured on coronal CT imaging), excision is highly likely to be successful. If the coalition exceeds 50%, the remaining articular cartilage is generally insufficient to maintain normal joint kinematics or bear physiological loads, making primary subtalar arthrodesis the preferred intervention.
Contraindications must be strictly observed to prevent disastrous clinical outcomes. Advanced degenerative arthritis of the posterior facet or the Chopart joint is an absolute contraindication for isolated excision, as restoring motion to an arthritic joint will only exacerbate the patient's pain. Similarly, a severe, rigid hindfoot valgus deformity (typically >16 degrees of resting valgus) that cannot be passively corrected is a strong relative contraindication. In such cases, simply excising the coalition will not correct the mechanical axis of the lower extremity; the eccentric load will persist, leading to continued pain and eventual failure. These patients require either a concurrent calcaneal osteotomy (e.g., medializing calcaneal osteotomy) to realign the mechanical axis or a primary arthrodesis.
| Parameter | Indications for Excision | Contraindications for Excision |
|---|---|---|
| Clinical Status | Failure of >3 months conservative care | Asymptomatic incidental finding |
| Age | Skeletally immature or young adult | Advanced age with rigid deformity |
| Coalition Size | < 50% involvement of posterior facet | > 50% involvement of posterior facet |
| Joint Health | Healthy posterior facet and Chopart joint | Advanced subtalar or midfoot arthritis |
| Hindfoot Alignment | Neutral or mild, passively correctable valgus | Severe, rigid valgus (>16 degrees) |
| Infection | None | Active local or systemic infection |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning, anchored by advanced cross-sectional imaging, is the cornerstone of a successful talocalcaneal coalition excision. The diagnostic workup begins with a standard series of weight-bearing radiographs of the foot and ankle, including anteroposterior (AP), lateral, and oblique views.

On the oblique radiograph, the clinician may observe a blurring or absence of the normal radiolucent line of the middle facet.

The lateral radiograph is particularly high-yield, often demonstrating the classic "C-sign"—a continuous radiodense line formed by the medial outline of the talar dome and the inferior outline of the sustentaculum tali. Additionally, a dorsal talar beak may be present; it is crucial to recognize that this beak is a traction osteophyte at the insertion of the talonavicular capsule, driven by altered biomechanics, and does not represent true degenerative arthritis of the talonavicular joint.
While plain radiographs provide valuable alignment data, a Computed Tomography (CT) scan is absolutely mandatory for every patient undergoing surgical excision.
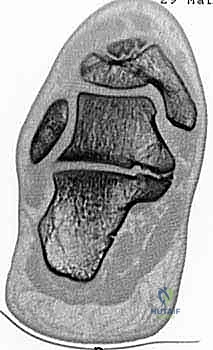
The CT scan, particularly the coronal and axial reformats, provides a definitive, high-resolution, three-dimensional map of the coalition. It allows the surgeon to precisely quantify the percentage of subtalar joint involvement, assess the exact anatomical location and orientation of the osseous bridge, and evaluate the health of the remaining posterior and anterior facets. Magnetic Resonance Imaging (MRI) is generally reserved for cases where plain films and CT are equivocal, specifically when a purely fibrous or cartilaginous coalition (syndesmosis or synchondrosis) is suspected but not clearly visualized on CT, or to evaluate for concurrent soft tissue pathology such as posterior tibial tendon tendinosis.
Patient positioning and operating room setup must be optimized to facilitate unhindered access to the medial hindfoot. The patient is positioned supine on the operating table. Because the medial approach requires excellent visualization of the sustentaculum tali, the operative leg must be allowed to assume a natural external rotation posture. If the patient's intrinsic hip rotation is insufficient to expose the medial ankle adequately, a gel pad or rolled blanket is placed beneath the contralateral hip to bump the pelvis and externally rotate the operative extremity.
A well-padded pneumatic tourniquet is applied to the proximal thigh. Exsanguination and tourniquet inflation are critical; the dissection involves navigating around the posterior tibial neurovascular bundle, and a bloodless field is non-negotiable for the safe identification and protection of these microscopic structures. Prior to standard sterile skin preparation and draping, a thorough examination under anesthesia (EUA) is performed. The surgeon meticulously assesses the resting alignment of the hindfoot and aggressively tests the subtalar range of motion (inversion and eversion). Documenting this baseline rigidity is essential for intraoperative comparison once the coalition is resected.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Superficial Dissection
The procedure commences with a meticulously planned medial approach.

A longitudinal incision is made along the medial aspect of the hindfoot, centered directly over the palpable prominence of the sustentaculum tali. The incision extends from the anterior margin of the Achilles tendon posteriorly to the prominence of the navicular tuberosity anteriorly. This generous length is necessary to expose the normal joint spaces both anterior and posterior to the coalition. The initial dissection is carried through the skin and subcutaneous tissues using a #15 blade, taking care to identify and retract any branches of the saphenous nerve anteriorly or medial calcaneal nerve branches posteriorly.
Deepening the exposure, the surgeon encounters the investing fascia of the abductor hallucis muscle at the plantar margin of the wound. Using Metzenbaum scissors, the superior fascia of the abductor hallucis is incised, and the muscle belly is bluntly mobilized and retracted plantarly. This maneuver exposes the deep fascial layer and the flexor retinaculum.
The surgeon must now systematically identify the critical tendinous landmarks. Dorsally, the robust tibialis posterior tendon is identified. Immediately plantar to it is the flexor digitorum longus (FDL) tendon. The neurovascular bundle is located directly posterior to the FDL tendon and must be visually confirmed and continuously protected throughout the remainder of the procedure.
Deep Dissection and Exposure of the Coalition
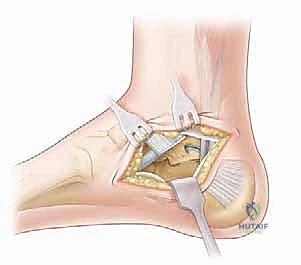
With the neurovascular bundle identified and gently retracted using a blunt vessel loop or a smooth Ragnell retractor, the surgeon focuses on the FDL tendon sheath.

The medial aspect of the FDL sheath is incised longitudinally, directly over the sustentaculum tali. The periosteum overlying the talus and calcaneus in this region is elevated as a continuous flap with the FDL sheath. It is imperative to preserve this tissue layer, as it will be utilized during closure to secure the interposition graft and prevent medial subluxation of the tendons. Retracting the FDL tendon and the neurovascular bundle plantarly reveals the underlying osseous pathology: the talocalcaneal coalition bridging the middle facet.

The limits of the coalition must now be definitively established. The surgeon uses a Freer elevator to probe anteriorly until the normal, cartilage-covered anterior facet or talonavicular joint is identified. Similarly, the elevator is passed posteriorly, navigating superior to the sustentaculum tali, to identify the anterior margin of the normal posterior facet. These two points—the normal anterior and posterior cartilaginous surfaces—dictate the absolute boundaries of the required resection.
Resection of the Osseous Bridge
The resection is the most technically demanding phase of the procedure.
Using a combination of sharp osteotomes, rongeurs, and a high-speed motorized burr, the surgeon begins to systematically dismantle the osseous bridge. The osteotome is directed laterally, parallel to the inclination of the subtalar joint. Extreme caution is required to avoid directing the osteotome too plantarly, which risks fracturing the sustentaculum tali, or too dorsally, which risks violating the talar neck.

The resection must be aggressive and comprehensive. The surgeon must remove a rectangular block of bone, ensuring that no tethering osseous or cartilaginous fragments remain laterally within the depths of the sinus tarsi.
Once the macroscopic bridge is removed, a high-speed burr is utilized to widen the gap, aiming for a minimum clearance of 1.0 to 1.5 centimeters between the talus and the calcaneus across the entire footprint of the former coalition. Following the resection, the surgeon intraoperatively assesses subtalar motion. The previously rigid hindfoot should now demonstrate free, uninhibited inversion and eversion. If a hard, mechanical block persists, the resection is incomplete, and further bone must be removed from the lateral or posterior margins of the defect.
Interposition Arthroplasty and Closure
To prevent the highly probable complication of osseous regrowth (recurrence), an interposition arthroplasty must be performed to fill the dead space created by the resection. While various materials have been described, including bone wax (largely historical and associated with foreign body reactions) and synthetic polymers, autologous biological grafts remain the gold standard.

An autologous fat graft, typically harvested from the ipsilateral gluteal fold, thigh, or the popliteal fossa, is highly effective.

The fat graft is sized to completely obliterate the bony defect.

It is packed tightly into the resected space, extending laterally into the depths of the sinus tarsi. Alternatively, a pedicled slip of the FHL tendon or the local FHL muscle belly can be mobilized and sutured into the defect.

Once the interposition graft is secured, the tourniquet is deflated, and meticulous hemostasis is achieved. The previously preserved periosteal-FDL sheath flap is then carefully repaired over the interposition material using absorbable sutures.

This layer acts as a biological retaining wall, preventing the fat graft from extruding and restoring the smooth gliding surface for the FDL tendon. The abductor hallucis fascia is reapproximated, followed by standard closure of the subcutaneous tissue and skin. The foot is placed in a well-padded, short-leg plaster splint in a neutral alignment.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the excision of a talocalcaneal coalition carries a distinct profile of potential complications. The most frequent and frustrating complication is the recurrence of the coalition, typically secondary to inadequate initial resection or failure of the interposition graft. Recurrence rates in the literature vary from 5% to 15%. Patients with recurrence present with a return of their preoperative pain and a progressive loss of the subtalar motion gained immediately postoperatively. Prevention relies entirely on aggressive intraoperative resection (achieving a 1.5 cm gap) and the secure placement of a robust biological interposition graft.
Neurological injury is the most devastating intraoperative complication. The posterior tibial nerve and its terminal branches (the medial and lateral plantar nerves) are acutely vulnerable during the deep dissection and retraction phases. Injury can range from a transient traction neuropraxia, which typically resolves over 3 to 6 months, to complete transection resulting in permanent plantar numbness and intrinsic muscle paralysis. Meticulous identification, blunt retraction, and continuous visual confirmation of the neurovascular bundle are the only reliable methods of prevention.
Persistent pain and deformity despite successful excision represent another complex challenge. This usually occurs when the procedure is performed in the presence of unrecognized posterior facet arthritis or when a severe preoperative valgus deformity is left unaddressed. In these scenarios, the altered biomechanics continue to generate pain. When conservative salvage measures (custom bracing, orthotics) fail, surgical salvage is required. The definitive salvage procedure for a failed excision, recurrent coalition, or progressive arthritis is a subtalar arthrodesis (if the Chopart joint is spared) or a triple arthrodesis. If the primary issue is persistent valgus malalignment without severe arthritis, a medializing calcaneal osteotomy may be utilized to shift the mechanical axis and offload the lateral column.
| Complication | Estimated Incidence | Prevention Strategy | Salvage/Management |
|---|---|---|---|
| Recurrent Coalition | 5% - 15% | Resect >1.5cm gap; robust fat/FHL interposition | Revision excision vs. Subtalar Arthrodesis |
| Tibial Nerve Injury | < 2% | Direct visualization; gentle, blunt retraction | Observation (neuropraxia) vs. Nerve repair/grafting |
| Persistent Valgus/Pain | 10% - 20% | Pre-op recognition of severe deformity; concurrent osteotomy | Medializing Calcaneal Osteotomy vs. Arthrodesis |
| Subtalar Arthritis | 10% - 25 |
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding excision-of-talocalcaneal-coalition