Tendon Transfer for Thumb Adduction Restoration: Boyes and Smith Techniques
Key Takeaway
Restoration of thumb adduction is critical in ulnar nerve palsy to rebuild key pinch strength. The Boyes and Smith techniques utilize the brachioradialis or extensor carpi radialis brevis, extended by a tendon graft, to dynamically replace the paralyzed adductor pollicis. This guide details the biomechanical principles, precise surgical approaches, graft routing through the interosseous spaces, and postoperative rehabilitation required to achieve optimal functional outcomes.
Comprehensive Introduction and Patho-Epidemiology
The loss of thumb adduction is unequivocally one of the most functionally devastating and biomechanically complex consequences of low ulnar nerve palsy. The intrinsic musculature of the hand, heavily reliant on ulnar nerve innervation, governs the delicate balance between gross motor grasp and fine motor precision. Among these muscles, the adductor pollicis stands paramount as the primary motor unit responsible for powerful key pinch (lateral pinch). In a physiologically intact hand, the adductor pollicis contributes approximately 50% to 80% of the total pinch strength, generating forces that allow humans to perform essential daily tasks ranging from turning a key in a lock to firmly grasping a heavy object. When the adductor pollicis is paralyzed, the resulting functional deficit is profound, leading to a cascade of compensatory biomechanical derangements that severely compromise hand dexterity and power.
Patients suffering from profound adductor pollicis paralysis inevitably develop classic compensatory mechanisms as they attempt to substitute the lost adduction force with intact extrinsic musculature. The most notable of these is Froment’s sign, characterized by hyperflexion of the thumb interphalangeal (IP) joint. This occurs because the patient instinctively recruits the flexor pollicis longus (FPL), innervated by the anterior interosseous branch of the median nerve, to pinch against the index finger. Concurrently, the loss of the adductor pollicis, which normally stabilizes the metacarpophalangeal (MCP) joint in flexion, leads to Jeanne’s sign—a profound hyperextension deformity of the thumb MCP joint during active pinch. Over time, these dynamic imbalances can lead to fixed contractures, articular degeneration, and a severely dysfunctional first web space.
The patho-epidemiology of ulnar nerve palsy leading to adductor paralysis is diverse. Traumatic lacerations of the ulnar nerve at the wrist or distal forearm represent the most common etiology in younger, active populations. However, severe compressive neuropathies (such as advanced cubital tunnel syndrome or Guyon's canal syndrome), Hansen’s disease (leprosy) in endemic regions, and iatrogenic injuries during complex distal radius or volar wrist surgery also contribute significantly to the incidence. Regardless of the etiology, once irreversible motor loss is established and the window for primary nerve repair or nerve transfer has closed (typically beyond 12 to 18 months), dynamic tendon transfers become the definitive reconstructive solution.
To restore functional pinch strength and correct these debilitating deformities, the two most prominent and biomechanically sound procedures are the Boyes technique and the Smith technique. Both procedures fundamentally rely on redirecting a powerful, expendable donor muscle—such as the brachioradialis (BR) or the extensor carpi radialis brevis (ECRB)—through the intermetacarpal spaces to mimic the native vector of the adductor pollicis. The success of these procedures is predicated not merely on surgical execution, but on a profound understanding of the intricate biomechanical interplay between the donor muscle excursion, the chosen pulley system, and the precise tensioning required to restore the adductor moment arm without tethering thumb opposition.
Detailed Surgical Anatomy and Biomechanics
A masterful execution of adductor pollicis reconstruction demands an intimate comprehension of both the native anatomical structures and the biomechanical parameters being recreated. The native adductor pollicis is a bipennate intrinsic muscle consisting of an oblique head and a transverse head. The oblique head originates from the capitate bone and the bases of the second and third metacarpals, while the transverse head originates from the volar surface of the third metacarpal shaft. Both heads converge to insert onto the ulnar sesamoid of the thumb MCP joint and the ulnar base of the proximal phalanx, with fascial expansions contributing to the dorsal extensor apparatus. This dual-headed configuration provides a broad, powerful vector that pulls the first metacarpal proximally and ulnarly, stabilizing the MCP joint and bringing the thumb into the palm for a forceful lateral pinch.
The biomechanics of lateral (key) pinch dictate that the reconstructive vector must closely approximate this native line of pull. If the transfer is routed too volarly, it will act primarily as a thumb flexor rather than an adductor. Conversely, if it is routed too proximally or dorsally, it will fail to provide the necessary transverse force to oppose the index finger. The genius of both the Boyes and Smith techniques lies in their use of the intermetacarpal spaces (the third and second, respectively) as natural biological pulleys. By passing an intercalary tendon graft through these spaces from dorsal to volar, the graft is forced to turn a corner, thereby redirecting the longitudinal pull of a forearm donor muscle into the transverse and oblique vector required for thumb adduction.
When evaluating donor muscles, excursion and force generation are the two critical variables. The Brachioradialis (BR), utilized in the classic Boyes transfer, is a massive muscle with excellent force-generating capacity (high physiological cross-sectional area). However, its native excursion is relatively limited, typically around 15 to 20 mm. To achieve the 30 mm of excursion required for full thumb adduction and abduction, the BR must be meticulously mobilized and freed from its dense fascial investments in the proximal forearm. Failure to perform this radical fascial release is the primary reason for failure in BR-based transfers. The Extensor Carpi Radialis Brevis (ECRB), popularized by Smith, offers a more favorable native excursion (approximately 30 to 40 mm) and a centralized dorsal location, making it an exceptionally reliable donor, provided the Extensor Carpi Radialis Longus (ECRL) is intact and capable of maintaining robust wrist extension.
Because neither the BR nor the ECRB possesses sufficient length to reach the adductor insertion on the thumb, an intercalary tendon graft is mandatory. The palmaris longus (PL) is the premier choice due to its expendability, ease of harvest, and appropriate caliber. However, the PL is absent in approximately 15% of the population. In such cases, the plantaris tendon serves as an excellent, albeit more distant, alternative. The plantaris provides exceptional length, allowing for a doubled graft if additional structural integrity is desired. The biomechanical success of the construct ultimately hinges on the integrity of the Pulvertaft weave connecting the donor to the graft, and the precise tensioning that balances the resting posture of the thumb against the active excursion of the transferred unit.
Exhaustive Indications and Contraindications
The decision to proceed with a dynamic tendon transfer for thumb adduction must be based on a rigorous clinical evaluation. Tendon transfers are powerful tools, but they are unforgiving if applied to the wrong patient or in the presence of uncorrected preoperative deficits. The primary indication is an irreversible ulnar nerve palsy with profound weakness or complete absence of key pinch, typically manifesting as a Medical Research Council (MRC) Grade 0 to 2 in the adductor pollicis.
Patients must demonstrate severe functional impairment, such as the inability to hold a pen, turn a key, or perform occupational tasks requiring lateral pinch. The presence of severe adductor pollicis atrophy, combined with positive Froment’s and Jeanne’s signs, confirms the biomechanical necessity of the procedure. In cases of combined median and ulnar nerve palsies (the severe "intrinsic minus" or "claw" hand), adductor restoration is just one component of a much more complex, multi-tendon reconstructive strategy that must also address thumb opposition and finger clawing.
Absolute and relative contraindications must be meticulously respected to avoid catastrophic functional outcomes. The following table delineates the critical parameters for patient selection.
| Category | Specific Indication / Contraindication | Clinical Rationale and Surgical Implications |
|---|---|---|
| Indications | Irreversible Low Ulnar Nerve Palsy | The primary indication. Must be confirmed clinically and electromyographically that no spontaneous recovery is expected (typically >12-18 months post-injury). |
| Indications | Combined Median/Ulnar Nerve Palsy | Requires adductor restoration in conjunction with opposition transfers (e.g., FDS to APB or EIP to APB). Tensioning must be perfectly balanced to prevent a fixed adducted posture. |
| Indications | Traumatic Adductor Muscle Loss | Severe crush injuries or compartment syndrome resulting in direct ischemic necrosis of the adductor pollicis muscle belly. |
| Contraindications | Fixed First Web Space Contracture | Absolute Contraindication. A tendon transfer cannot overcome a stiff joint or contracted web space. A Z-plasty, skin graft, or release of the first dorsal interosseous fascia must be performed first. |
| Contraindications | Inadequate Donor Muscle Strength | Absolute Contraindication. The donor muscle (BR or ECRB) must be MRC Grade 5. A transferred muscle inherently loses one grade of strength; transferring a Grade 4 muscle will result in non-functional Grade 3 pinch. |
| Contraindications | Lack of Supple CMC/MCP/IP Joints | Absolute Contraindication. Passive range of motion must be full and unrestricted. Fixed hyperextension of the MCP joint may require concurrent MCP arthrodesis or volar capsulodesis. |
| Contraindications | Severe Spasticity or Dystonia | Relative Contraindication. Central nervous system disorders (e.g., cerebral palsy, stroke) make post-operative motor re-education highly unpredictable and risk severe contractures. |
| Contraindications | Poor Soft Tissue Bed | Relative Contraindication. Extensive dorsal or palmar scarring from prior trauma will impede tendon gliding. Staged reconstruction with silicone rods (Hunter rods) may be necessary. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful tendon transfer. The surgeon must begin with a comprehensive physical examination, meticulously documenting the MRC grade of all potential donor muscles. If the Boyes technique (BR) is planned, the surgeon must verify that the patient can forcefully flex the elbow against resistance with the forearm in neutral rotation, ensuring a robust brachioradialis. If the Smith technique (ECRB) is selected, the surgeon must isolate and test the ECRL to guarantee that wrist extension will not be compromised upon harvesting the ECRB. The ECRL is tested by asking the patient to extend the wrist with radial deviation, whereas the ECRB extends the wrist centrally.
Electromyography (EMG) and Nerve Conduction Studies (NCS) are highly recommended, particularly in cases where the etiology of the palsy is ambiguous or if there is a question regarding the integrity of the donor muscle innervation. Furthermore, the surgeon must physically assess the suppleness of the first web space. The thumb should easily achieve wide radial and palmar abduction. If the angle between the first and second metacarpals is less than 40-45 degrees passively, a preliminary or concurrent soft tissue release (such as a four-flap Z-plasty or release of the adductor origin) is mandatory.
Patient positioning and operating room setup must be optimized for meticulous soft tissue handling and intraoperative assessment of tension. The patient is positioned supine on the operating table with the affected extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The use of a tourniquet is essential for maintaining a bloodless field, particularly during the intricate dissection of the intermetacarpal spaces and the fascial release of the brachioradialis. However, the surgeon must be mindful of tourniquet time, as prolonged ischemia can alter the resting tension of the muscles, potentially complicating the final tensioning phase.
Loupe magnification (typically 2.5x to 3.5x) is strongly advised to facilitate the identification and protection of vital neurovascular structures, most notably the superficial branch of the radial nerve (RSN) during the BR harvest, and the digital nerves during the distal adductor attachment. The entire upper extremity, from the fingertips to the axilla, is prepped and draped to allow for full, unimpeded manipulation of the wrist and elbow during the assessment of tendon excursion and the setting of final tension.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of adductor restoration requires precision, respect for soft tissue gliding planes, and a deep understanding of vector mechanics. The two primary techniques—the Boyes procedure and the Smith procedure—differ primarily in their choice of donor muscle and intermetacarpal routing, but both demand identical rigor in graft harvesting and distal fixation.
The Boyes Procedure (Brachioradialis Transfer)
The Boyes technique traditionally employs the brachioradialis (BR) to restore adduction. The BR is a massive, highly pennate muscle capable of generating immense force, but its utility is entirely dependent on the surgeon's ability to maximize its excursion.
Step 1: Donor Muscle Harvest and Radical Mobilization
A longitudinal incision, approximately 8 to 10 cm in length, is made over the radial aspect of the distal forearm, centered precisely over the musculotendinous junction of the brachioradialis. The subcutaneous tissues are divided, and the superficial branch of the radial nerve (RSN) is immediately identified as it emerges from beneath the BR tendon in the distal third of the forearm. The RSN must be meticulously protected with vessel loops. The BR tendon is traced distally and detached sharply from its insertion on the radial styloid.
The critical phase of this step is the proximal mobilization. The BR is heavily invested in the antebrachial fascia, which acts as a tether. The surgeon must systematically release all fascial bands, epimysial attachments, and intermuscular septa up to the proximal third of the forearm. The surgeon should gently pull the detached tendon distally; if the muscle belly does not yield at least 30 mm of free excursion, further proximal fascial release is mandatory.
Step 2: Tendon Graft Harvest
A tendon graft is harvested to bridge the gap. The palmaris longus is identified via a small transverse incision at the distal wrist crease. If present, a tendon stripper is passed proximally to harvest the entire length of the tendon. If the PL is absent, a plantaris tendon is harvested from the ipsilateral or contralateral leg using a standard medial retromalleolar incision and a long tendon stripper.
Step 3: Distal Attachment to the Thumb
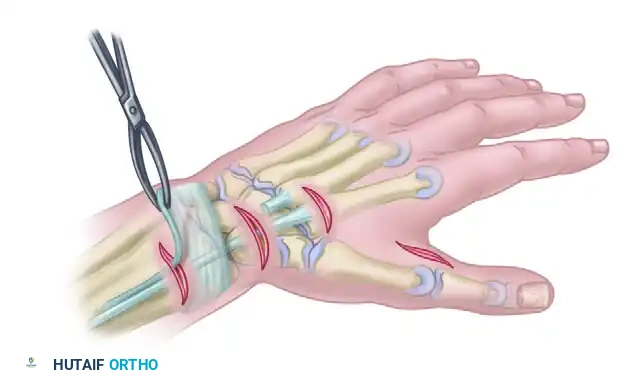
A curved or longitudinal incision is made over the ulnar aspect of the thumb MCP joint. The subcutaneous tissues are swept aside to expose the adductor tubercle and the robust, albeit paralyzed, tendinous insertion of the adductor pollicis. The distal end of the harvested tendon graft is secured to this tendinous insertion. A robust weave technique is preferred, utilizing 3-0 or 4-0 non-absorbable braided polyester sutures (e.g., Ethibond or Ticron). The graft must be deeply embedded into the native adductor tendon to withstand the massive forces of key pinch.
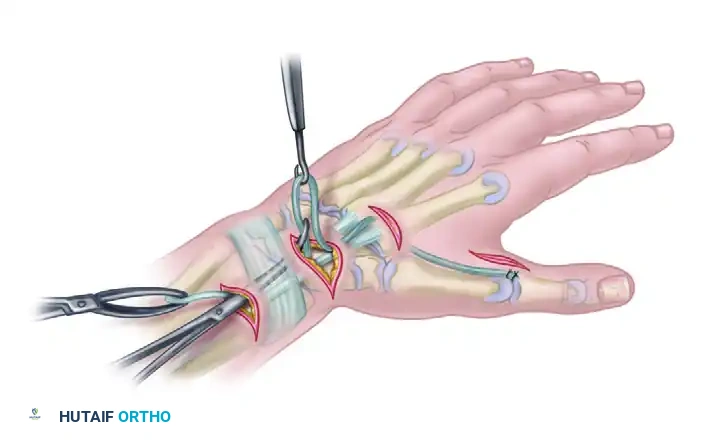
Step 4: Routing the Graft via the Third Interspace
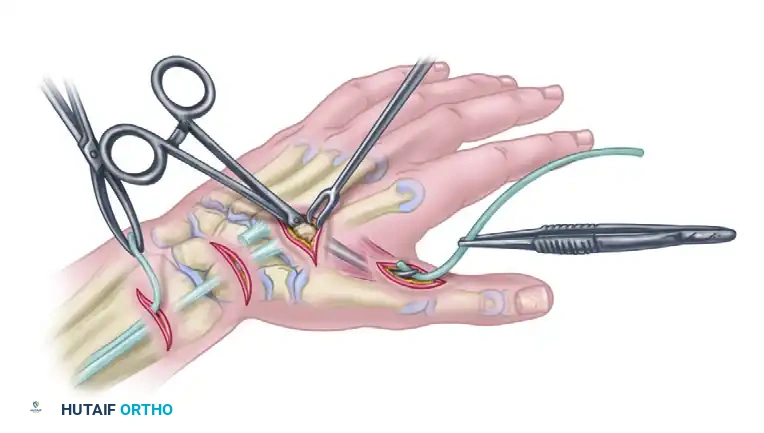
A curved tendon passer is introduced through the thumb incision and directed proximally along the native path of the adductor muscle belly. The passer is then directed dorsally through the third interosseous space (between the third and fourth metacarpals). A small dorsal counter-incision is made over the third web space to retrieve the passer and the graft. This specific routing creates a pulley effect that pulls the thumb metacarpal proximally, ulnarly, and into slight pronation—the exact vector required for lateral pinch.
Step 5: Proximal Attachment and Tensioning
The graft is then passed subcutaneously from the dorsal hand, directed proximally and radially toward the mobilized brachioradialis tendon in the distal forearm. The subcutaneous tunnel must be wide and free of adhesions.
Setting the tension is the most critical phase of the operation. The tension should be set maximally with the thumb held in full radial and palmar abduction, and the wrist in a neutral (zero degrees) position. The graft is woven into the BR tendon using a standard Pulvertaft weave, incorporating at least three separate passes. Each pass is secured with a figure-of-eight non-absorbable suture. The tenodesis effect is then tested: passive wrist flexion should cause the thumb to fall into adduction, while passive wrist extension should allow the thumb to abduct fully.
The Smith Procedure (ECRB Transfer)
Smith described a highly effective modification utilizing the Extensor Carpi Radialis Brevis (ECRB). The ECRB is an ideal donor due to its central dorsal location, excellent native excursion, and expendability. In Smith's original series, key pinch strength was reported to have doubled on average following this specific transfer.
Step 1: Incisions and Exposure
Standard incisions are meticulously planned to access the ECRB dorsally, the intermetacarpal space, and the adductor insertion on the thumb.
* Incision A: A transverse or short longitudinal incision over the base of the third metacarpal to access the ECRB insertion.
* Incision B: A longitudinal incision at the musculotendinous junction of the ECRB in the mid-to-distal forearm.
* Incision C: A dorsal incision over the second intermetacarpal space.
* Incision D: A volar-ulnar incision at the thumb MCP joint to access the adductor pollicis insertion.
Step 2: Detachment and Withdrawal of the ECRB

The ECRB tendon is identified at its insertion on the dorsal base of the third metacarpal. It is transected as distally as possible to maximize functional length. The tendon is then withdrawn proximally through the forearm incision (Incision B). It is imperative that the ECRB is pulled completely proximal to the dorsal retinacular ligament (the extensor sheath). Leaving the tendon within or deep to the retinaculum will result in severe friction, bowstringing, and an altered line of pull that compromises the transfer's efficiency.
Step 3: Graft Passage Through the Second Interspace
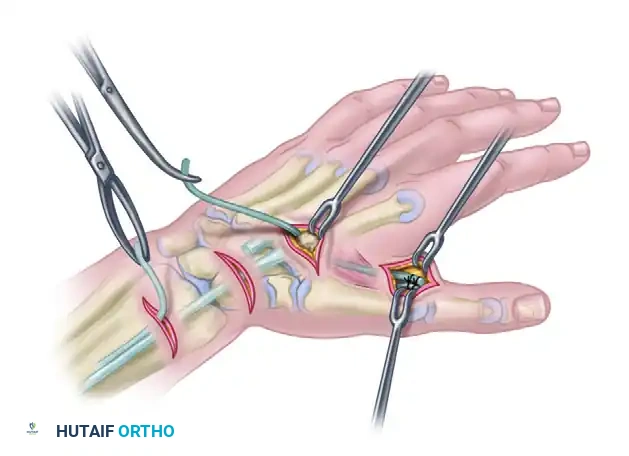
Following the harvest of a palmaris longus or plantaris tendon graft, a curved tendon passer is utilized to channel the graft deep to the adductor pollicis fascia. The graft is passed dorsally between the second and third metacarpals (the second interosseous space). This routing is slightly more radial than the Boyes technique and provides a direct, highly efficient, and powerful vector for thumb adduction against the index finger.
Step 4: Distal Fixation to the Adductor Pollicis
At the thumb MCP joint, the tendinous insertion of the adductor pollicis is definitively identified. The distal end of the tendon graft is sutured securely to this adductor tendon. A robust weave technique, supplemented by locking core sutures, must be utilized to prevent distal pull-out under the extreme forces generated during post-operative key pinch.
Step 5: Subcutaneous Proximal Routing
The proximal end of the tendon graft is retrieved at the dorsal second interspace incision. A large Kelly clamp or tendon passer is used to create a wide subcutaneous tunnel from the dorsal hand to the proximal forearm incision where the ECRB is waiting. The subcutaneous tunnel must be sufficiently capacious to allow unimpeded, frictionless gliding of the bulky graft-tendon Pulvertaft junction.
Step 6: Proximal Suturing and Final Tensioning
The ECRB and the tendon graft are prepared for a Pulvertaft weave. Tensioning parameters for the Smith technique are highly specific: the tendon graft is sutured proximally to the ECRB with the thumb held in full, rigid adduction and the wrist maintained at exactly 0 degrees of extension (neutral). At this precise position, the ECRB should be pulled to its resting length (removing all slack, but not stretching the muscle belly).
Clinical Nuance: If the thenar muscles (median nerve innervated) are also paralyzed, the graft should be tensioned slightly looser (made slightly longer) to prevent a severe, fixed adduction contracture that would block any subsequent attempts at thumb opposition.
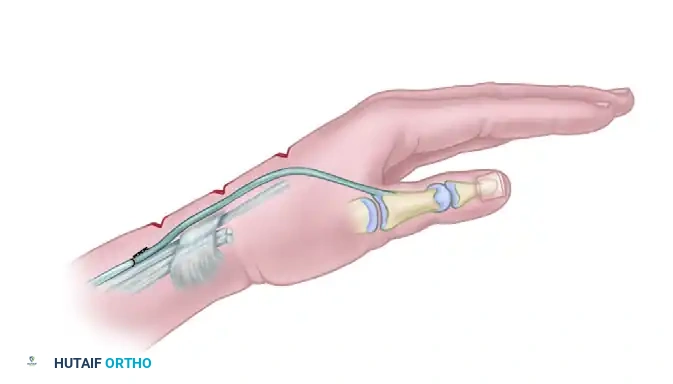
The final construct demonstrates the ECRB withdrawn proximal to the extensor retinaculum, securely woven into the intercalary tendon graft, which dives smoothly through the second intermetacarpal space to insert onto the adductor pollicis. This creates a seamless, biomechanically optimized dynamic restraint that effectively restores the adductor moment arm.
Complications, Incidence Rates, and Salvage Management
While dynamic tendon transfers for thumb adduction are highly successful when executed with precision, they carry a distinct profile of potential complications. The interosseous spaces are highly fascial and unforgiving environments; any technical error in routing, tensioning, or soft tissue handling will be magnified during the rehabilitation phase. The operative surgeon must anticipate these pitfalls and possess the reconstructive armamentarium to manage them effectively.
The most common and arguably most frustrating complication is inappropriate tensioning. Under-tensioning occurs when the graft is left too loose during the Pulvertaft weave. Because tendons naturally undergo a degree of viscoelastic stretching (creep) during the early rehabilitation phase, a transfer that is "just right" on the operating table will often become too loose post-operatively. The donor muscle will expend its entire excursion simply taking up the slack in the system, resulting in weak or entirely absent pinch strength. Conversely, over-tensioning results in a fixed adduction contracture of the first web space. This is particularly devastating in patients with concurrent median nerve weakness, as they will be mechanically unable to abduct the thumb to grasp large objects, rendering the hand functionally worse than before surgery.
Adhesions represent another significant hurdle. The passage of a tendon graft through the second or third intermetacarpal space places it in direct contact with the interosseous fascia and the periosteum of the metacarpals. Rough handling of the graft, failure to create a wide enough tunnel, or prolonged post-operative immobilization can lead to severe, unyielding adhesions. These adhesions tether the graft, nullifying the excursion of the donor muscle and causing the transfer to act as a static tenodesis rather than a dynamic motor unit.
| Complication | Estimated Incidence | Pathophysiology & Etiology | Salvage Management & Revision Strategy |
|---|---|---|---|
| Under-tensioning (Weak Pinch) | 10% - 15% | Failure to set maximum tension intra-op; excessive post-op viscoelastic stretch; failure of the Pulvertaft weave. | Revision surgery to explore the weave, re-tension the graft (shorten the construct), and reinforce the sutures. |
| Over-tensioning (Adduction Contracture) | 5% - 8% | Setting tension with the wrist in excessive extension or thumb in inadequate abduction; failure to account for median nerve palsy. | Aggressive splinting and therapy. If refractory, surgical lengthening of the graft (Z-lengthening) or release of the adductor insertion. |
| Severe Adhesions / Tethering | 10% - 12% | Rough tissue handling; narrow subcutaneous tunnels; prolonged immobilization (>4 weeks) preventing early gliding. | Intensive hand therapy. If no progress by 6 months, surgical tenolysis. In severe cases, a staged reconstruction with a silicone rod may be required. |
| Radial Sensory Nerve (RSN) Neuroma | 2% - 5% | Iatrogenic injury or traction neuropraxia during the fascial release of the Brachioradialis in the Boyes technique. | Non-operative: Gabapentinoids, desensitization. Operative: Neuroma excision and burying the proximal nerve stump into the pronator quadratus or BR muscle belly. |
| Loss of Wrist Extension (Donor Morbidity) | < 2% | Harvesting the ECRB in a patient with an absent, weak, or injured ECRL, resulting in a devastating drop-wrist deformity. | Preventable error. Requires a secondary tendon transfer (e.g., Pronator Teres to ECRB) to restore wrist extension. |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of a Boyes or Smith tendon transfer is inextricably linked to the quality and compliance of the post-operative rehabilitation protocol. The biological goal is to protect the tendon weave during the vulnerable inflammatory and early proliferative phases of healing, while simultaneously introducing controlled stress to prevent restrictive adhesions and promote longitudinal collagen alignment. This requires a delicate, highly supervised balance managed by a specialized hand therapist.
Phase 1: Immobilization and Protection (Weeks 0 to 3)
Immediately post-operatively in the operating room, a bulky, well-padded plaster or fiberglass splint is applied over sterile dressings. The positioning of the hand within this splint is paramount to protect the transfer. The thumb must be held in strict adduction and slight palmar flexion to remove all tension from the distal insertion and the graft. If a wrist extensor (ECRB) or the brachioradialis was utilized, the wrist is immobilized in approximately 30 degrees of extension to relieve tension on the proximal Pulvertaft weave. The fingers (digits 2 through 5) are left entirely free. The patient is instructed to perform active range of motion of the fingers and elbow immediately to reduce dependent edema, facilitate venous return, and prevent stiffness in the uninvolved joints.
Phase 2: Early Active Motion and Cortical Re-education (Weeks 3 to 6)
At exactly 3 weeks post-operation, the rigid surgical splint is removed. The early proliferative phase of tendon healing has provided sufficient tensile strength to withstand gentle, controlled motion, though the weave remains vulnerable to sudden forceful loads. The patient is transitioned to a custom-molded, thermoplastic, removable forearm-based thumb spica splint.
Crucial Restriction: The splint must be fabricated to physically block thumb hyperextension and excessive palmar or radial abduction.
During therapy sessions, the splint is removed, and active, gravity-eliminated adduction exercises are initiated. This phase is critical for "cortical re-education"—training the brain to fire the donor muscle to achieve a new functional outcome. For example, if the ECRB was transferred, the patient is taught to actively attempt wrist extension; because the ECRB is now attached to the thumb, this cognitive effort will result in thumb adduction. The therapist utilizes the natural tenodesis effect (flexing the wrist to passively tighten the extensor-based transfer) to facilitate early gliding of the graft through the intermetacarpal space without overloading the suture lines.
Phase 3: Strengthening, Weaning, and Return to Function (Weeks 6 to 12+)
By 6 weeks, the tendon weave has entered the remodeling phase, and the collagen fibers are cross-linking and aligning along lines of stress. Passive stretching is carefully introduced to regain full first web space mobility, and gentle strengthening exercises are initiated. The protective thermoplastic splint is gradually weaned; initially, it is removed for light activities of daily living and worn only at night or during high-risk environments (e.g., crowded spaces, public transport).
Formal pinch strengthening, utilizing therapeutic putty of increasing resistance and mechanical pinch gauges, begins at 8 weeks. The therapist focuses on integrating the newly restored lateral pinch into complex, multi-step functional tasks. Full, unrestricted activity, including heavy manual labor or sports, is typically permitted by 12 weeks, provided that the patient demonstrates adequate motor control, the tendon weave is clinically stable, and pinch strength has plateaued at a functional level. Maximum functional recovery and cortical plasticity may continue to improve for up to 12 to 18 months post-operatively.
Summary of
