Primary Flexor Tendon Repair: Surgical Techniques & Zones
Key Takeaway
Primary flexor tendon repair requires meticulous surgical technique and a profound understanding of hand biomechanics. Outcomes depend heavily on the anatomical zone of injury, particularly within Zone II's fibro-osseous sheath. Successful repair necessitates precise core and peripheral suturing, preservation of the A2 and A4 pulleys, and careful management of the flexor digitorum sublimis and profundus relationship. This guide details zone-specific approaches, surgical pearls, and rehabilitation protocols to optimize functional recovery.
Comprehensive Introduction and Patho-Epidemiology
The primary repair of flexor tendons remains unequivocally one of the most technically demanding and unforgiving procedures in the armamentarium of the orthopedic hand surgeon. The ultimate functional outcome of a severed flexor tendon is inextricably linked to the initial operating surgeon’s technical acumen, the precise management of the delicate fibro-osseous sheath, and the rigorous, unwavering application of postoperative rehabilitation protocols. Historically, flexor tendon surgery was fraught with unacceptably high rates of restrictive adhesion formation and catastrophic catastrophic repair rupture. However, modern primary flexor tendon repair—when executed by an experienced, fellowship-trained hand surgeon utilizing contemporary multi-strand core suture techniques—yields satisfactory to excellent functional results in over 80% to 90% of appropriately selected patients.
The epidemiology of flexor tendon injuries reveals a predilection for the young, active, and working-class populations, with a significant peak in incidence occurring in males between the ages of 15 and 40 years. These injuries are frequently sustained via occupational hazards involving sharp machinery, accidental lacerations from broken glass or knives, and sports-related trauma (such as the classic "jersey finger" avulsion). The patho-epidemiology dictates that outcomes are generally superior in these younger demographics, whose robust intrinsic healing capabilities and neuroplasticity significantly outpace the results observed in older cohorts or those requiring delayed secondary repairs and staged tendon reconstructions.
The decision to perform a primary repair carries profound clinical responsibility. The operating surgeon must possess not only the advanced microsurgical proficiency required to execute the primary repair but also the comprehensive knowledge to perform subsequent tenolysis or staged tendon grafting should the primary repair fail. The paradigm of flexor tendon surgery has shifted dramatically over the past several decades, moving away from the historical dogma of passive-only rehabilitation toward aggressive Early Active Motion (EAM) protocols. This shift necessitates a paradigm change in the operating room; the surgeon must construct a biomechanically superior repair capable of withstanding the substantial forces generated during active digital flexion without succumbing to gap formation.
Furthermore, the pathoanatomy of a flexor tendon laceration extends beyond the tendon itself. These injuries are rarely isolated. The surgeon must maintain a high index of suspicion for concomitant neurovascular injuries, particularly digital nerve lacerations in the digits and median or ulnar nerve transections at the level of the wrist. The failure to identify and primarily repair these associated structures leads to devastating sensory deficits, intrinsic muscle atrophy, and a profoundly compromised functional outcome, regardless of the success of the tendon repair itself.
Detailed Surgical Anatomy and Biomechanics
A profound and exhaustive understanding of the surgical anatomy and biomechanics of the flexor tendon system is the absolute prerequisite for successful surgical intervention. The flexor surface of the hand and distal forearm is universally divided into five distinct anatomical zones, originally classified by Verdan, based on the unique biomechanical, vascular, and anatomical challenges present in each specific region.

Zone I to Zone V Anatomy
Zone I extends from just distal to the insertion of the flexor digitorum sublimis (FDS) tendon to the terminal insertion of the flexor digitorum profundus (FDP) tendon at the volar base of the distal phalanx. Injuries in this zone isolate the FDP tendon. Zone II, famously coined "no man's land" by Sterling Bunnell due to historically dismal outcomes, encompasses the critical area of the flexor pulley system. It extends from the distal palmar crease to the insertion of the FDS tendon. This zone houses both the FDS and FDP tendons within a tightly constrained fibro-osseous sheath, making it highly susceptible to post-surgical adhesions. Zone III comprises the area between the distal margin of the transverse carpal ligament and the proximal reflection of the flexor sheath (the A1 pulley), characterized by the origin of the lumbrical muscles from the FDP tendons. Zone IV represents the segment of tendons passing deep to the transverse carpal ligament within the carpal tunnel, a highly restricted space where injuries are frequently accompanied by median nerve lacerations. Finally, Zone V extends proximally from the transverse carpal ligament into the distal volar forearm.
The Fibro-Osseous Sheath and Pulley System
The digital fibro-osseous sheath is a complex, multi-layered structure essential for efficient biomechanical function. It is composed of five stout annular pulleys (A1 through A5) and three thinner, collapsible cruciform pulleys (C1 through C3). The annular pulleys act as critical biomechanical fulcrums, keeping the flexor tendons closely apposed to the phalangeal longitudinal axis during flexion. The A2 pulley (located over the proximal phalanx) and the A4 pulley (located over the middle phalanx) are biomechanically paramount. Disruption or surgical excision of these specific pulleys leads to profound "bowstringing" of the flexor tendons, resulting in a devastating loss of mechanical advantage, reduced digital excursion, and a significant decrease in the active range of motion at the interphalangeal joints.
Tendon Nutrition and Vascularity
The survival, healing, and gliding capacity of the flexor tendons rely on a highly specialized dual system of nutrition: vascular perfusion and synovial diffusion. The vascular supply is segmental. Proximally, blood is supplied by longitudinal vessels originating from the muscle belly. Distally, the tendons receive blood from the osseous insertions. Within the critical Zone II, the tendons are relatively avascular anteriorly, receiving their blood supply dorsally through delicate mesenteric structures known as the vincula (vincula brevia and vincula longa). However, modern research has definitively established that synovial diffusion (imbibition) provides the overwhelming majority of the nutritional requirements for the tendons within the digital sheath. This physiological reality underscores the importance of minimizing trauma to the epitenon and, when possible, repairing the synovial sheath to restore the closed environment necessary for optimal synovial fluid dynamics.
Biomechanics of Tendon Repair
The mechanical integrity of a flexor tendon repair must withstand the forces of early active motion protocols to prevent adhesion formation while simultaneously avoiding gap formation or catastrophic rupture. The work of flexion—the force required to pull the tendon through the sheath—increases exponentially in the presence of edema, bulky suture knots, or a poorly approximated repair site. A gap of merely 3 millimeters at the repair site significantly alters the biomechanics of the digit, leads to a functionally longer tendon with reduced force transmission, and drastically increases the risk of complete rupture. Consequently, the modern surgeon must utilize multi-strand core suture configurations that provide immense tensile strength while maintaining a low-profile, smooth epitenon surface to minimize gliding resistance.
Exhaustive Indications and Contraindications
The timing and indication for flexor tendon repair are dictated by the nature of the injury, the physiological status of the wound, and the patient's overall capacity to participate in rigorous postoperative rehabilitation. Primary repair is defined as surgical intervention occurring within the first 24 hours post-injury. Delayed primary repair occurs between 24 hours and 14 days. Secondary repair is undertaken between 2 and 4 weeks, while late secondary repair or reconstruction is reserved for injuries presenting after 4 weeks.
The absolute indication for primary or delayed primary flexor tendon repair is a sharply lacerated or avulsed flexor tendon in a medically stable patient with adequate soft tissue coverage and a clean, uncontaminated wound bed. Early intervention prevents tendon retraction, muscle belly contracture, and the collapse of the fibro-osseous sheath, which severely complicate delayed reconstructions. Furthermore, primary repair allows for the simultaneous definitive management of concomitant digital nerve and vascular injuries, restoring the critical neurovascular bundles before irreversible retraction occurs.
Conversely, contraindications to primary repair must be strictly respected to avoid disastrous complications such as deep space infections or massive tissue necrosis. Absolute contraindications include severe crush injuries with extensive soft tissue loss that precludes adequate coverage of the repaired tendon. Grossly contaminated wounds, such as human bites or agricultural injuries with heavy soil contamination, must undergo serial debridement and delayed closure; primary tendon repair in this setting guarantees purulent tenosynovitis and subsequent tendon necrosis.
Relative contraindications require nuanced surgical judgment. Patients with severe cognitive impairments, psychiatric instability, or a documented history of profound non-compliance are poor candidates for primary repair followed by early active motion. In these populations, the intricate balance of protecting the repair while preventing adhesions cannot be maintained, often leading to rupture. In such scenarios, delayed staged reconstruction, tenodesis, or even primary arthrodesis of the distal interphalangeal joint may represent a more prudent and ultimately functional definitive treatment strategy.
| Category | Indications for Primary Repair | Contraindications for Primary Repair |
|---|---|---|
| Wound Characteristics | Sharp, clean lacerations (e.g., glass, knife). | Severe crush injuries; gross contamination (bite wounds, farm injuries). |
| Soft Tissue Envelope | Adequate, viable skin coverage available. | Massive soft tissue avulsion requiring complex flap coverage. |
| Timing | Acute presentation (< 14 days). | Late presentation (> 4 weeks) with fixed muscle contracture. |
| Anatomical Factors | Intact or repairable pulley system (A2/A4). | Destruction of the entire fibro-osseous sheath. |
| Patient Factors | Compliant, motivated, cognitively intact. | Severe non-compliance, profound cognitive deficits, severe psychiatric illness. |
| Associated Injuries | Concomitant clean nerve/artery lacerations. | Unstable, complex, comminuted phalangeal fractures requiring extensive fixation. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning begins with a comprehensive and systematic clinical examination. The surgeon must meticulously assess the integrity of both the FDS and FDP tendons independently. The FDS is tested by holding all non-injured digits in absolute extension to neutralize the common muscle belly of the FDP, thereby allowing isolated assessment of FDS flexion at the proximal interphalangeal (PIP) joint. The FDP is tested by neutralizing the PIP joint in extension and assessing active flexion of the distal interphalangeal (DIP) joint. Furthermore, a rigorous assessment of digital perfusion (capillary refill, Allen's test of the digit) and sensibility (static two-point discrimination) is mandatory to rule out concomitant neurovascular compromise.
Imaging modalities play a secondary but occasionally vital role. While standard orthogonal radiographs are obligatory to rule out associated fractures or retained radiopaque foreign bodies (such as glass or metallic fragments), advanced imaging is rarely required for acute sharp lacerations. However, in cases of delayed presentation or closed avulsion injuries (Jersey finger), high-resolution musculoskeletal ultrasound or Magnetic Resonance Imaging (MRI) without contrast can precisely delineate the level of tendon retraction, the integrity of the vincula, and the presence of bony avulsion fragments, thereby guiding the surgical approach and the decision between primary repair versus staged reconstruction.
Patient positioning and operating room setup are critical elements that directly influence surgical efficiency and outcome. The patient is typically positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Historically, general anesthesia or axillary regional blocks were universally employed. However, the modern era has seen a massive paradigm shift toward the use of Wide Awake Local Anesthesia No Tourniquet (WALANT). Utilizing a mixture of lidocaine and epinephrine injected meticulously into the surgical field, WALANT provides excellent hemostasis without a tourniquet and, crucially, allows the awake patient to actively flex their digits intraoperatively. This enables the surgeon to directly visualize the tendon repair, assess for gap formation under physiological load, and ensure that the repair glides smoothly through the pulley system without triggering.
Surgical instrumentation must be highly specialized. The surgeon must utilize loupe magnification (minimum 2.5x to 3.5x) or an operating microscope for nerve and vessel repair. Fine microsurgical instruments, including delicate atraumatic forceps, tenotomy scissors, and fine needle holders, are indispensable. The surgical field must be meticulously prepped and draped to allow for full, unrestricted passive and active mobilization of the wrist and all digits during the procedure, facilitating the retrieval of retracted tendons and the assessment of the digital cascade.
Step-by-Step Surgical Approach and Fixation Technique
Incisions and Exposure
The surgical approach must provide expansile exposure while preventing postoperative flexion contractures. Volar zigzag Bruner incisions or mid-lateral incisions are the gold standards. The Bruner incision utilizes angles of approximately 90 degrees, ensuring that the apices of the flaps do not cross the transverse digital flexion creases perpendicularly. Once the skin flaps are elevated, full-thickness dissection is maintained to protect the delicate subdermal vascular plexus and the underlying digital neurovascular bundles, which must be identified and systematically protected throughout the entirety of the procedure.
Sheath Management and Pulley Preservation
Upon exposing the fibro-osseous sheath, the surgeon must meticulously evaluate the integrity of the pulley system.
Crucial pulleys, specifically A2 and A4, must be preserved at all costs. Access to the severed tendon ends is typically achieved by creating transverse or L-shaped windows in the thinner cruciform pulleys or the membranous portions of the sheath. If the tendon has retracted proximally, it can often be "milked" distally by flexing the wrist and MCP joints. If this fails, a pediatric feeding tube or a specialized tendon retriever can be passed through the intact sheath to capture the proximal stump. Blind, forceful grasping within the sheath is strictly prohibited, as it destroys the delicate epitenon and guarantees severe adhesion formation.
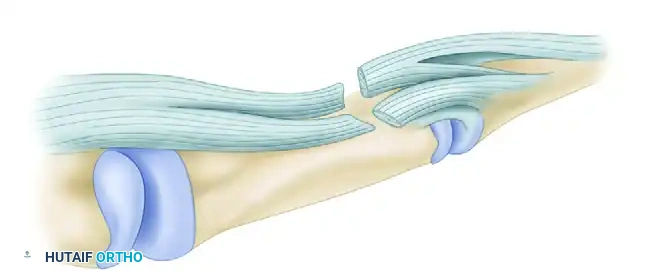
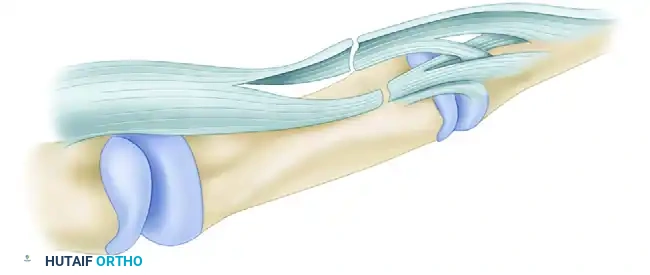
Managing the Sublimis Spiral (Camper's Chiasma)
In Zone II injuries, a profound understanding of the FDS anatomy is required to avoid catastrophic surgical errors. Just distal to the metacarpophalangeal (MCP) joint, the FDS splits into two slips. These slips wind around the FDP tendon, decussating at Camper's chiasma to insert on the middle phalanx.

If a laceration occurs at the midpoint of this spiral, the proximal and distal ends rotate 90 degrees in opposite directions. An unwary surgeon may suture ends that appear to align but are actually malrotated. This obliterates the channel for the FDP tendon, blocking excursion and destroying functional motion.
Delivering the Retracted Profundus
When the FDP has retracted proximally, it must be carefully delivered back through the split portion of the FDS. The anatomical relationship must be perfectly reestablished, ensuring the FDP lies palmar to Camper's chiasma before passing distally into the digit.
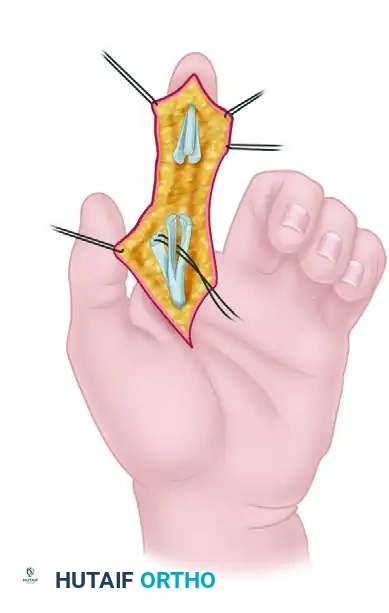
Core and Epitendinous Suture Configuration
The biomechanical foundation of the repair is the core suture. Contemporary evidence unequivocally supports the use of a four-strand or six-strand core suture utilizing a 3-0 or 4-0 non-absorbable braided synthetic material (e.g., FiberWire, Supramid, or Tycron). The core sutures should be placed in the dorsal half of the tendon, which provides a mean repair strength that is significantly greater than volar placement. The suture technique (e.g., Modified Kessler, Cruciate, or Strickland) must incorporate locking loops that securely grasp the longitudinal tendon fibers, preventing pull-out under tension.
Following the core repair, a running, circumferential peripheral epitendinous suture utilizing 5-0 or 6-0 monofilament nylon is mandatory. This peripheral stitch serves two vital functions: it increases the overall tensile strength of the repair by up to 50%, and it smooths the repair site, tucking in any exposed collagen bundles. This smooth surface minimizes gliding resistance, prevents "triggering" or catching on the annular pulleys during excursion, and significantly reduces the biological stimulus for adhesion formation.
Zone-Specific Nuances
In Zone I, if the distal FDP stump is less than 1 cm, the proximal tendon is advanced and reinserted directly into the distal phalanx using a pull-out wire technique or modern suture anchors, strictly adhering to the "1-Centimeter Rule" to avoid the quadriga effect. In Zone III, the surgeon must meticulously avoid suturing the lumbrical muscle bellies to prevent the debilitating "lumbrical plus" finger. In Zone IV, the transverse carpal ligament should be released using a Z-lengthening configuration, allowing it to be repaired loosely to act as a retaining pulley while accommodating postoperative swelling and preventing tendon subluxation.
Complications, Incidence Rates, and Salvage Management
Despite flawless surgical technique and rigorous postoperative care, primary flexor tendon repair is associated with a recognized spectrum of complications. The surgeon must constantly navigate the precarious biomechanical tightrope between repair rupture (resulting from excessive force or inadequate suture strength) and restrictive adhesion formation (resulting from inadequate excursion and prolonged immobilization). Understanding the incidence and management of these complications is critical for comprehensive patient care.
Tendon rupture is the most devastating acute complication, typically occurring between the first and third postoperative weeks when the intrinsic tensile strength of the healing tendon is at its nadir. The incidence of rupture in modern, multi-strand protocols ranges from 2% to 5%. Rupture is usually precipitated by an accidental sudden extension force applied to the digit or patient non-compliance with the splinting regimen. If a rupture is identified within the first 10 to 14 days, prompt surgical re-exploration and primary re-repair can be attempted. However, late ruptures or repeated failures necessitate a transition to salvage procedures, such as two-stage tendon grafting utilizing a silicone Hunter rod.
Adhesion formation remains the most common complication, with clinically significant restriction of glide occurring in 15% to 25% of patients. Adhesions tether the repaired tendon to the surrounding fibro-osseous sheath or adjacent bone, severely limiting active flexion while passive flexion remains relatively preserved. If the patient reaches a definitive plateau in rehabilitation (typically 3 to 6 months postoperatively) with supple joints and resolved induration, a surgical tenolysis is indicated. Flexor tenolysis is a technically demanding salvage procedure requiring extensive dissection to liberate the tendon while meticulously preserving the vital A2 and A4 pulleys.
Other notable complications include joint contractures, particularly PIP joint flexion contractures, which occur due to prolonged immobilization or bowstringing if the pulley system fails. Infection is relatively rare (less than 2% incidence) but catastrophic when it involves the closed synovial space of the flexor sheath, rapidly leading to tendon necrosis and requiring emergent radical debridement. Finally, complex regional pain syndrome (CRPS) may develop, necessitating immediate recognition, aggressive pain management, and intensive desensitization therapy.
| Complication | Estimated Incidence | Primary Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Tendon Rupture | 2% - 5% | Non-compliance, weak core suture, sudden extension force. | Early: Re-repair. Late: 2-stage tendon graft (Hunter rod). |
| Restrictive Adhesions | 15% - 25% | Immobilization, severe initial trauma, poor epitenon repair. | Intensive hand therapy; Surgical Tenolysis at 3-6 months. |
| PIP Flexion Contracture | 10% - 15% | Prolonged splinting in flexion, pulley incompetence. | Dynamic extension splinting; surgical release if refractory. |
| Bowstringing | < 5% | Failure to preserve or reconstruct A2 / A4 pulleys. | Pulley reconstruction using extensor retinaculum or tendon graft. |
| Deep Space Infection | 1% - 2% | Contaminated wound, delayed presentation, poor soft tissue. | Emergent I&D, targeted IV antibiotics, delayed reconstruction. |
| "Lumbrical Plus" Finger | Rare | Erroneous suturing of lumbrical belly in Zone III repairs. | Lumbrical tendon sectioning / release under local anesthesia. |
Phased Post-Operative Rehabilitation Protocols
The success of a primary flexor tendon repair is not achieved in the operating theater alone; it is equally dependent on the stringent execution of a phased postoperative rehabilitation protocol directed by a certified hand therapist. The evolution of flexor tendon rehabilitation has transitioned from historical passive-only protocols (such as the Kleinert or Duran protocols) to modern Early Active Motion (EAM) protocols (such as the modified Belfast, Indiana, or Manchester protocols). EAM protocols capitalize on the robust tensile strength of 4- and 6-strand core repairs to initiate actual tendon excursion, which dramatically reduces the formation of dense, restrictive adhesions.
The initial phase (Weeks 0 to 4) focuses on protecting the repair while stimulating intrinsic healing. The patient is placed in a dorsal blocking splint, typically positioning the wrist in 20 to 30 degrees of extension, the MCP joints in 50 to 70 degrees of flexion, and the IP joints in neutral extension. Placing the wrist in slight extension represents a critical biomechanical advantage; it significantly reduces the "work of flexion" required by the flexor muscle bellies to pull the tendon through the sheath. During this phase, patients perform controlled, light active flexion of the digits within the constraints of the splint, followed by passive extension to the splint limits.
The intermediate phase (Weeks 4 to 6) marks the transition to increased mechanical loading. The dorsal blocking splint is gradually modified or discontinued during the day, though it may be retained at night for protection against involuntary movements. Active composite flexion and extension exercises are progressed. The therapist may introduce specific tendon gliding exercises—hook fist, straight fist, and full fist—to maximize differential glide between the FDS and FDP tendons. Differential gliding is essential to prevent cross-adhesions between the two tendon slips in Zone II.
The advanced phase (Weeks 6 to 8 and beyond) focuses on restoring full functional capacity and tensile strength. Passive extension exercises are aggressively pursued to resolve any residual PIP joint flexion contractures. At 8 weeks, light strengthening exercises are initiated, utilizing therapeutic putty or light gripping devices. Unrestricted, heavy functional use of the hand, including heavy lifting and contact sports, is strictly prohibited until a minimum of 10 to 12 weeks postoperatively, allowing the collagen matrix of the healing tendon to mature, cross-link, and achieve maximal physiological resilience.
Summary of Landmark Literature and Clinical Guidelines
The modern principles of primary flexor tendon repair are the culmination of decades of rigorous biomechanical research and landmark clinical trials. Understanding this foundational literature is imperative for the academic orthopedic surgeon. The seminal work of Sterling Bunnell in the mid-20th century highlighted the profound difficulties of Zone II injuries, cementing the term "no man's land" in the surgical lexicon. However, it was Claude Verdan who subsequently proved that primary repair within this zone was not only possible but superior to delayed grafting, fundamentally altering the surgical approach.
The biomechanical revolution in suture configurations was spearheaded by researchers such as James Strickland. Strickland's exhaustive in vitro studies definitively demonstrated that the tensile strength of a tendon repair is directly proportional to the number of suture strands crossing the repair site. His advocacy for the 4-strand core repair, combined with a robust peripheral epitendinous suture, provided the mechanical foundation that made Early Active Motion protocols safe and effective. Furthermore, the work of Tang et al. expanded upon this, popularizing the 6-strand repair for even greater security, particularly in complex or multi-level injuries.
In the contemporary era, the clinical guidelines established by the American Society for Surgery of the Hand (ASSH) and international consensus groups strongly endorse the widespread adoption of the WALANT technique. Landmark publications by Donald Lalonde have demonstrated that WALANT not only eliminates the risks associated with general anesthesia and tourniquet use but also provides the surgeon with real-time, intraoperative biomechanical feedback. The ability to observe the repaired tendon actively gliding through the pulley system allows for immediate correction of gaps or triggering, representing the single greatest advancement in flexor tendon surgery in the 21st century. These evidence-based principles—multi-strand core repairs, meticulous epitenon approximation, WALANT anesthesia, and aggressive Early Active Motion—constitute the definitive standard of care for primary flexor tendon repair today.
