Two-Stage Reconstruction for Digital Flexion and Key Pinch in Tetraplegia
Key Takeaway
The House two-stage reconstruction is a foundational surgical strategy for restoring digital flexion and key pinch in patients with cervical spinal cord injuries. Stage one establishes a stable extensor tenodesis, while stage two utilizes active tendon transfers—specifically the extensor carpi radialis longus to the flexor digitorum profundus, and the pronator teres to the flexor pollicis longus—to restore functional grasp and pinch biomechanics.
Comprehensive Introduction and Patho-Epidemiology
The restoration of hand function in patients suffering from cervical spinal cord injuries (tetraplegia) represents one of the most profound, life-altering interventions within the realm of reconstructive orthopedic and hand surgery. The epidemiological landscape of spinal cord injuries reveals that a significant proportion of these devastating events occur in the cervical spine, predominantly affecting young, active individuals. For patients with mid-cervical lesions—most classically at the C6 or C7 neurological levels—the preservation of active wrist extension provides a critical, salvageable biomechanical foundation. This residual motor function serves as the physiological engine for restoring functional grasp and key pinch through the surgically optimized tenodesis effect. The profound loss of independence associated with tetraplegia is intimately tied to the inability to perform activities of daily living (ADLs), such as feeding, self-catheterization, and transferring. Consequently, reconstructive tetraplegia surgery is not merely an anatomical exercise, but a definitive pathway to restoring human dignity and functional autonomy.
The House two-stage reconstruction stands as an internationally recognized, highly structured, and biomechanically rigorous surgical protocol designed specifically to restore digital flexion and key pinch in this challenging patient population. Pioneered by Dr. James House and subsequently refined by generations of reconstructive hand surgeons, this technique addresses the complex, multidirectional force requirements of the hand by deliberately dividing the reconstruction into two distinct temporal phases: an "extensor phase" (Stage 1) and a "flexor phase" (Stage 2). By separating these conflicting biomechanical vectors, the surgeon can precisely set the tension required for a functional tenodesis grasp without the deleterious effects of simultaneous, opposing tendon transfers that frequently compromise single-stage procedures. This staged approach allows for the stabilization of the extensor mechanism, ensuring that the critical "release" function of the hand is fully healed before the powerful "grasp" forces are introduced.
Understanding the patho-epidemiology of tetraplegia is essential for anticipating the unique physiological and anatomical challenges encountered during reconstruction. Unlike peripheral nerve injuries, where the lower motor neuron is often the sole site of pathology, spinal cord injuries present a complex upper motor neuron syndrome characterized by spasticity, autonomic dysreflexia, and altered central motor control. The denervated muscles in tetraplegia undergo profound atrophy, while muscles with intact innervation may exhibit varying degrees of spasticity or synergistic co-contraction. The surgeon must meticulously evaluate not only the absolute strength of the potential donor muscles but also their phase of activation, excursion capacity, and susceptibility to spastic override. Furthermore, the chronic nature of tetraplegia often leads to secondary joint contractures, disuse osteopenia, and complex regional pain syndromes, all of which must be aggressively managed prior to surgical intervention to ensure a compliant and functional upper extremity.
Detailed Surgical Anatomy and Biomechanics
The successful execution of the House two-stage reconstruction demands an exhaustive, three-dimensional understanding of the surgical anatomy of the forearm and hand, coupled with a deep appreciation for the complex biomechanics of the tenodesis effect. In the uninjured hand, grasp and pinch are orchestrated by a highly coordinated, synergistic activation of extrinsic flexors, extrinsic extensors, and intrinsic musculature. In the tetraplegic patient with a C6 or C7 injury, the loss of active digital flexors (flexor digitorum profundus [FDP], flexor digitorum superficialis [FDS], flexor pollicis longus [FPL]) and intrinsic muscles (lumbricals, interossei, thenar, and hypothenar groups) fundamentally alters the biomechanical equilibrium of the hand, resulting in a profound functional deficit.
The entire reconstructive paradigm relies on maximizing the biomechanics of wrist-driven tenodesis. The primary motor units driving this system are the extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB). Active wrist extension, powered by these intact muscles, must passively drive the digits into flexion for grasp and the thumb into adduction for key pinch. This relies on the precise tensioning of the transferred or tenodesed tendons across the volar aspect of the wrist joint. Conversely, gravity-assisted or active wrist flexion must passively extend the digits to allow for the release of objects. The moment arms of the tendons crossing the wrist joint dictate the excursion generated at the digits; therefore, preserving the anatomical retinacular systems (such as the extensor retinaculum and the flexor pulleys) is paramount to maintaining optimal biomechanical efficiency and preventing tendon bowstringing.
A critical anatomical and biomechanical consideration in tetraplegia is the management of the intrinsic-minus hand. The loss of intrinsic muscle function inevitably leads to a claw deformity, characterized by hyperextension of the metacarpophalangeal (MCP) joints and flexion of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints. This posture is mechanically disastrous for a tenodesis grasp, as the flexor force will simply exacerbate the PIP/DIP flexion without achieving functional MCP flexion, causing the fingertips to roll into the palm rather than wrapping around an object. To counteract this, an intrinsic tenodesis (such as the House modification or the Zancolli lasso) is mandatory. This procedure creates an anatomical checkrein that prevents MCP hyperextension and couples PIP flexion with MCP flexion, effectively restoring the synchronized rolling motion of the digits required for a functional grasp.
Exhaustive Indications and Contraindications
Patient selection for tetraplegic hand reconstruction is arguably the most critical determinant of ultimate surgical success. The evaluation is guided by the International Classification for Surgery of the Hand in Tetraplegia (ICSHT), which categorizes patients based on the number of intact, Grade 4 or 5 (Medical Research Council scale) muscles available below the elbow. The House two-stage technique is primarily indicated for patients in ICSHT Groups 4 and 5. Group 4 patients possess strong brachioradialis (BR), ECRL, ECRB, and pronator teres (PT) function. Group 5 patients possess all of the above plus the flexor carpi radialis (FCR). These patients have the requisite motor inventory to provide independent motors for wrist extension (ECRB), digital flexion (ECRL transfer), and thumb flexion/key pinch (PT transfer), making them ideal candidates for this comprehensive reconstruction.
Beyond the anatomical classification, the indications for surgery are heavily reliant on the patient's physiological and psychological readiness. The fundamental prerequisite for any tendon transfer or tenodesis in the tetraplegic hand is the presence of supple, contracture-free joints. Preoperative passive range of motion must be rigorously optimized; the patient must demonstrate full, unrestricted passive digital flexion with the wrist extended, and full passive digital extension with the wrist flexed. Furthermore, the patient must be highly motivated, possess adequate cognitive function to participate in a demanding, protracted rehabilitation protocol, and have a stable social support system to assist with ADLs during the lengthy periods of postoperative immobilization.
Contraindications to the House two-stage reconstruction are multifaceted and must be strictly respected to avoid catastrophic functional decline. Absolute contraindications include the presence of fixed, unyielding joint contractures that cannot be resolved through intensive hand therapy or serial casting. Severe, uncontrolled spasticity in the upper extremity is a major contraindication, as spastic override will inevitably rupture tendon weaves, stretch out tenodesis constructs, and result in severe, non-functional deformities. Additionally, a lack of patient motivation or an inability to comply with the strict postoperative immobilization and rehabilitation protocols precludes surgical intervention.
| Parameter | Indications for Two-Stage Reconstruction | Contraindications |
|---|---|---|
| Neurological Level | ICSHT Group 4 or 5 (C6-C7 equivalent level). | ICSHT Group 0-2 (Insufficient donor motors). |
| Muscle Strength | MRC Grade 4 or 5 in BR, ECRL, ECRB, PT. | Weak or spastic donor muscles (MRC < 4). |
| Joint Mobility | Supple, contracture-free joints (full passive ROM). | Fixed joint contractures (especially PIP/MCP). |
| Spasticity | Absent or mild, easily controlled spasticity. | Severe, uncontrolled spasticity or clonus. |
| Psychosocial | Highly motivated, compliant, strong support system. | Cognitive impairment, poor compliance, unrealistic goals. |
| Systemic Health | Stable medical condition, optimized nutrition. | Severe autonomic dysreflexia, active decubitus ulcers. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful tetraplegic hand reconstruction. The evaluation begins with a meticulous manual muscle test (MMT) of the entire upper extremity, repeated on multiple occasions to ensure consistency and rule out transient fatigue or spasticity-induced variations. The surgeon must carefully palpate the proposed donor muscles (ECRL, PT, BR) to assess their bulk, excursion, and independence of activation. Differentiating the ECRL from the ECRB is critical; the patient is asked to perform active wrist extension, and the radial deviation vector (ECRL) is compared to the central extension vector (ECRB). If the ECRB is weak or absent, utilizing the ECRL as a donor will result in a catastrophic loss of wrist extension power, necessitating a complete revision of the surgical plan.
Templating in the context of tendon transfers involves a detailed, written surgical algorithm outlining the primary plan and potential salvage options. The surgeon must map out the intended donor-recipient pairings, the routing pathways (subcutaneous vs. subfascial), and the method of intrinsic reconstruction. If the patient has a hypermobile or unstable thumb carpometacarpal (CMC) joint, the preoperative plan must include a CMC arthrodesis during Stage 1 to provide a stable post against which the key pinch can be generated. Preoperative photographs and videos documenting the patient's baseline functional attempts and passive range of motion are invaluable for intraoperative reference and postoperative outcome assessment.
Patient positioning in the operating room must accommodate the unique physiological vulnerabilities of the tetraplegic patient. The patient is positioned supine on a well-padded operating table, with meticulous attention paid to pressure point offloading to prevent decubitus ulcers. The operative arm is extended on a radiolucent hand table. A pneumatic tourniquet is applied high on the brachium; however, inflation times must be strictly monitored, as tetraplegic patients may exhibit altered ischemic tolerance and are at risk for autonomic dysreflexia triggered by tourniquet pain. The surgical team must work in close communication with the anesthesiologist to monitor blood pressure and heart rate continuously. The use of high-quality loupe magnification (minimum 3.5x) and focal illumination is mandatory for the precise identification of paratenon, retinacular structures, and the execution of meticulous tendon weaves.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the House two-stage reconstruction is an exercise in extreme precision, demanding meticulous tissue handling and an absolute mastery of biomechanical tensioning. The procedure is definitively split into the Extensor Phase (Stage 1) and the Flexor Phase (Stage 2), separated by a healing interval of 2 to 6 months.
Stage 1: The Extensor Phase
The primary objective of the first stage is to establish a reliable mechanism for digital and thumb extension when the wrist is flexed, while simultaneously preventing MCP joint hyperextension. This is achieved through a series of precise tenodeses to the distal radius.
The extensor digitorum communis (EDC) tendons are accessed via a dorsal longitudinal incision over the distal forearm and wrist. The extensor retinaculum is carefully incised, preserving the dorsal carpal ligament to prevent bowstringing. The EDC tendons are mobilized, and their musculotendinous junctions are identified. The tendons are divided proximally and routed to the dorsal aspect of the distal radius. Fixation to the radius is achieved using robust suture anchors or transosseous tunnels. The tensioning here is critical: with the wrist passively flexed to 40 degrees, the EDC tendons are tensioned so that the MCP joints are held in full extension (0 degrees). Crucially, the surgeon must verify that full passive flexion of the fingers remains obtainable when the wrist is extended to 40 degrees. Over-tensioning will result in a permanent extension contracture, obliterating the future grasp.
Simultaneously, the thumb extensor and abductor tenodesis is performed. The abductor pollicis longus (APL) and extensor pollicis longus (EPL) tendons are identified, divided proximally, and rerouted for fixation to the radial styloid or distal radius. The tensioning parameters require that with 40 degrees of wrist flexion, the thumb interphalangeal (IP) joint is extended to 0 degrees, and the thumb metacarpal rests in a position of radial abduction (30 to 40 degrees).
Finally, the intrinsic tenodesis (House modification) is executed to prevent the intrinsic-minus claw deformity. A free tendon graft (typically palmaris longus or a plantaris graft) is harvested. The graft is meticulously sutured into the central slip and lateral bands of the extensor apparatus of the index and middle fingers. It is then routed volarly through the lumbrical canals, passing volar to the deep transverse metacarpal ligament, and anchored to the dorsum of the metacarpal necks. This construct acts as an artificial oblique retinacular ligament; when the PIP joint flexes, it forces concomitant MCP flexion, acting as a robust, permanent checkrein against MCP hyperextension.
Stage 2: The Flexor Phase
Performed 2 to 6 months after Stage 1, the flexor phase is initiated only when the extensor tenodeses are solidly healed, and the patient has regained full, supple passive motion. The goal is to restore active digital flexion and thumb key pinch by transferring the ECRL to the FDP and the PT to the FPL.
A meticulously planned volar longitudinal incision is made, extending from the proximal wrist flexion crease to the midshaft of the radius. The FPL, PT, and FDP tendons are isolated proximal to their musculotendinous junctions. The ECRL is released via a short transverse incision over the base of the second metacarpal and withdrawn proximally into the forearm. The surgeon must absolutely verify the identity of the ECRL and preserve the ECRB, as inadvertent sacrifice of the ECRB will result in a devastating loss of central wrist extension.
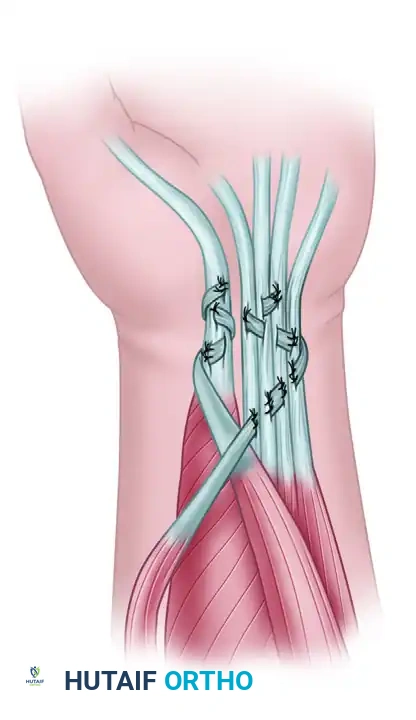
The core of the reconstruction involves the tendon transfers using classic Pulvertaft weaves. The PT is detached from the radius with a generous strip of periosteum to maximize length. The ECRL is freed from all fascial attachments to ensure maximum excursion. The PT is woven into the FPL, and the ECRL is woven into the FDP mass (which is often sutured together side-to-side to ensure a uniform cascade). The Pulvertaft weave must involve at least three, preferably four, orthogonal passes, secured with non-absorbable braided suture (e.g., 2-0 or 3-0 Ticron or Ethibond) to withstand the significant forces of early active rehabilitation.
Figure 71-41: House two-stage technique for reconstruction of digital flexion and key pinch—stage 2 (flexor phase). The Extensor carpi radialis longus is transferred to the flexor digitorum profundus, and the pronator teres is transferred to the flexor pollicis longus.
Tensioning during Stage 2 is the most unforgiving aspect of the entire reconstruction. For the PT to FPL transfer, the tension is set so that the thumb pulp rests firmly against the radial side of the index finger (the key pinch position) when the wrist is passively held in 30 degrees of extension. For the ECRL to FDP transfer, the tension must allow for a synchronous cascade of finger flexion when the wrist is brought into 40 degrees of extension. When the wrist is flexed to neutral, the fingers must fully extend via the Stage 1 tenodesis. If an opponensplasty is required to strengthen the pinch, the brachioradialis (BR) is transferred to the ring finger FDS, which is then routed subcutaneously to the EPL and adductor pollicis insertions.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the House two-stage reconstruction carries a significant risk profile, primarily due to the complex biomechanical demands placed on the transferred tissues and the unique physiological challenges of the tetraplegic patient. Complications can broadly be categorized into biomechanical failures (tensioning errors, tendon ruptures), biological failures (adhesions, joint contractures), and systemic/neurological issues (spasticity, autonomic dysreflexia).
The most common and functionally devastating complication is improper tensioning of the tendon transfers. Over-tensioning of the flexor phase (ECRL to FDP) will result in a permanent flexion contracture of the digits, completely obliterating the patient's ability to release objects. Conversely, under-tensioning will result in a weak, ineffectual grasp, as the transferred muscle will expend its entire excursion taking up the slack in the tendon before generating any force across the joints. Tendon rupture at the site of the Pulvertaft weave is rare (incidence < 2%) if proper technique is utilized, but it can occur if the patient is non-compliant with the postoperative immobilization protocol or experiences severe, sudden spastic spasms.
Adhesions and joint contractures are a constant threat. The extensive dissection required for these multi-tendon transfers creates a highly inflammatory environment prone to dense scar formation. If postoperative rehabilitation is delayed or inadequately supervised, the transferred tendons will adhere to the surrounding fascia, severely limiting excursion. Furthermore, prolonged immobilization can lead to collateral ligament contracture at the MCP and PIP joints. Complex Regional Pain Syndrome (CRPS) is another potential complication, requiring immediate recognition and aggressive multimodal management, including sympathetic blocks and intensive therapy, to prevent permanent stiffness.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Prevention |
|---|---|---|---|
| Over-tensioning (Flexion Contracture) | 5 - 10% | Improper intraoperative tensioning; failure to account for tenodesis effect. | Surgical release and lengthening of the tendon weave; intensive stretching therapy. |
| Under-tensioning (Weak Grasp) | 10 - 15% | Excessive initial slack; stretching of the weave during early rehab. | Surgical revision and re-tensioning (plication) of the tendon transfer. |
| Tendon Rupture | < 2% | Non-compliance with immobilization; severe spasticity; poor weave technique. | Immediate surgical re-exploration and repair; optimization of spasticity management. |
| Severe Adhesions / Stiffness | 15 - 20% | Delayed rehabilitation; excessive surgical trauma; prolonged immobilization. | Tenolysis (often delayed 6-12 months); aggressive active therapy; continuous passive motion. |
| Loss of Wrist Extension | Rare (< 1%) | Inadvertent harvest of the ECRB instead of the ECRL. | Catastrophic error. Requires complex salvage, potentially transferring BR to ECRB. |
Phased Post-Operative Rehabilitation Protocols
The surgical execution of the House two-stage reconstruction represents only half of the therapeutic equation; the ultimate functional outcome is inextricably linked to a rigorous, highly specialized, and phased postoperative rehabilitation protocol. The rehabilitation must be guided by a certified hand therapist with extensive experience in tetraplegia, working in close, continuous communication with the operating surgeon. The overarching principle of the rehabilitation phase is the protection of the healing tendon weaves while simultaneously facilitating cortical remapping and motor re-education.
Following Stage 1 (the extensor phase), the upper extremity is immobilized in a rigid, well-padded cast or orthosis. The wrist is positioned in 40 to 45 degrees of extension, the MCP joints in 40 degrees of flexion, and the IP joints in full extension. This strict immobilization is maintained for exactly 4 weeks to allow the tenodeses to heal solidly to the bone. Following this period, carefully guided active and passive motion is initiated. The focus is on maintaining the suppleness of the digits and training the patient to utilize wrist flexion to achieve passive digital extension.
Following Stage 2 (the flexor phase), the immobilization parameters are critically adjusted. The wrist is immobilized in 25 to 30 degrees of extension to remove tension from the newly constructed ECRL-FDP and PT-FPL transfers. The MCP joints are held in 40 to 50 degrees of flexion to protect the intrinsic tenodesis, while the thumb is positioned in functional key pinch against the radial aspect of the index finger. This immobilization is strictly maintained for 3.5 to 4 weeks.
The subsequent rehabilitation is divided into distinct phases. Phase I (Weeks 4-6) involves the removal of the cast and the fabrication of a custom thermoplastic splint in the identical protective position. Gentle, active-assisted range of motion is initiated. The patient is taught to use active wrist extension to drive digital flexion, consciously practicing the new tenodesis grasp. Crucially, passive stretching of the transfers is strictly prohibited. Phase II (Weeks 6-8) involves the gradual reduction of splint wear during the day. The patient begins light functional tasks, focusing on grasping lightweight, bulky objects (e.g., foam blocks) to train the new motor pathways and encourage tendon glide. Phase III (Weeks 8-12) introduces progressive strengthening. The patient works on refining key pinch dexterity and power. Heavy lifting and forceful passive stretching remain contraindicated until at least 12 weeks postoperatively, ensuring the tendon weaves have achieved maximum tensile strength.
Summary of Landmark Literature and Clinical Guidelines
The evolution of tetraplegic hand reconstruction is deeply rooted in a rich history of landmark anatomical studies and clinical innovations. The foundational concepts of utilizing the tenodesis effect for functional gain were initially popularized in the mid-20th century, but it was the pioneering work of Dr. James H. House and his colleagues at the University of Minnesota that codified the two-stage reconstructive protocol. House's seminal papers in the 1970s and 1980s meticulously detailed the biomechanical rationale for separating the extensor and flexor phases, demonstrating significantly improved functional outcomes and lower complication rates compared to single-stage, multi-tendon procedures. His introduction of the intrinsic tenodesis utilizing a free tendon graft remains a cornerstone technique for preventing the devastating claw deformity in these patients.
Further refinements to the surgical approach were contributed by Eduardo Zancolli, whose extensive work on the biomechanics of the intrinsic-minus hand led to the development of the "Zancolli lasso" procedure. While House utilized a free graft for intrinsic tenodesis, Zancolli's technique of utilizing the FDS tendon looped through the A1 or A2 pulley provided an alternative, dynamic solution that is still widely utilized depending on the availability of donor motors. Additionally, Erik Moberg's profound insights into the necessity of sensory feedback and the biomechanics of key pinch fundamentally shaped the objectives of tetraplegic reconstruction. Moberg emphasized that restoring a strong, stable key pinch (thumb to radial index finger) is functionally superior to attempting to restore a complex, multi-digit chuck pinch in the absence of intrinsic musculature.
Contemporary clinical guidelines are heavily structured around the International Classification for Surgery of the Hand in Tetraplegia (ICSHT), established in 1978 and continually updated by international consensus. The ICSHT provides a standardized, universal language for assessing motor inventory and guiding surgical decision-making. Current best practice guidelines universally mandate a multidisciplinary approach, requiring the integration of orthopedic surgeons, physiatrists, specialized hand therapists, and psychological support teams. The consensus literature emphasizes that surgical intervention should generally be delayed until at least 12 months post-injury to allow for maximal spontaneous neurological recovery and the stabilization of the patient's psychosocial environment, ensuring that the patient is fully prepared for the rigorous demands of the reconstructive journey.
