Mastering Flexor Tendon Pulley Reconstruction and Two-Stage Grafting
Key Takeaway
Reconstruction of the flexor tendon pulley system is critical for restoring digital biomechanics and preventing bowstringing. This surgical guide details the indications, operative techniques, and staged protocols for flexor pulley reconstruction and two-stage tendon grafting. Emphasizing the preservation of the A2 and A4 pulleys, it covers graft selection, Silastic rod placement, and precise postoperative rehabilitation to optimize functional outcomes in severely traumatized digits.
Comprehensive Introduction and Patho-Epidemiology
The management of complex flexor tendon injuries, particularly within the notoriously unforgiving fibro-osseous tunnel of Zone II—historically termed "No Man's Land" by Sterling Bunnell—remains one of the most formidable challenges in orthopedic hand surgery. When primary or delayed primary repair is precluded by severe trauma, extensive segmental tendon loss, or profound fibro-osseous scarring from previous failed interventions, the native gliding environment is irreversibly obliterated. In these catastrophic scenarios, the physiological capacity for intrinsic tendon healing is overwhelmed by an aggressive extrinsic healing response, resulting in dense, restrictive peritendinous adhesions that tether the tendon to the surrounding phalanges and fascial structures.
The two-stage flexor tendon reconstruction, originally conceptualized and popularized by James Hunter in the 1970s, represents a paradigm-shifting salvage procedure designed to overcome this biological impasse. The foundational principle of this technique is the induction of a biologically active, pseudo-synovial sheath. By temporarily implanting a biologically inert, Dacron-impregnated silicone rod (the Hunter prosthesis), the surgeon exploits the body's foreign-body reaction to encapsulate the implant in a smooth, mesentery-like layer of specialized connective tissue. This newly formed sheath mimics the low-friction environment of the native synovium, providing a pristine conduit for subsequent autologous tendon grafting.
Epidemiologically, the demand for two-stage reconstruction frequently arises in the context of devastating industrial accidents, high-energy crush injuries, or extensive infections (suppurative flexor tenosynovitis) that cause widespread necrosis of the flexor mechanism. Furthermore, a significant cohort of patients requiring this procedure are those who have undergone primary repair complicated by rupture, severe adhesion formation, or iatrogenic destruction of the critical pulley system. The success of this reconstructive endeavor is not merely a function of technical surgical execution; it is fundamentally dependent on meticulous patient selection, flawless preoperative optimization of joint mobility, and absolute patient compliance with a grueling, multi-month rehabilitation protocol.
Mastering this technique requires an intimate understanding of digital biomechanics, the precise spatial anatomy of the flexor pulley system, and the viscoelastic properties of tendon grafts. The surgeon must be adept at radical tenosynovectomy, intricate pulley reconstruction, and the dynamic tensioning of tendon grafts. This chapter provides an exhaustive, step-by-step exposition of the surgical anatomy, biomechanical principles, operative techniques, and postoperative management strategies essential for executing a successful two-stage flexor tendon and pulley reconstruction.
Detailed Surgical Anatomy and Biomechanics
The digital flexor sheath is a highly specialized, multi-layered fibro-osseous tunnel lined by a delicate synovial membrane. Its primary evolutionary function is to provide a low-friction, nutrient-rich gliding environment for the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons. Mechanically, the sheath acts as a complex system of retinacular restraints, maintaining the tendons in intimate apposition to the longitudinal axis of the phalanges. This close anatomical relationship is critical for optimizing the moment arm, allowing the linear excursion of the forearm flexor muscles to be efficiently translated into angular rotation at the metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints.
The structural integrity of this tunnel is maintained by a series of distinct retinacular condensations comprising five annular (A1-A5) and three cruciate (C1-C3) pulleys. The annular pulleys are dense, transversely oriented bands of fibrous tissue that provide the primary mechanical resistance against tendon bowstringing. The A1, A3, and A5 pulleys are strategically located over the MCP, PIP, and DIP joints, respectively. They are inherently flexible, attaching to the volar plates to accommodate joint flexion without buckling. Conversely, the A2 and A4 pulleys are rigid, diaphyseal structures originating directly from the periosteum of the proximal and middle phalanges. The cruciate pulleys (C1-C3) are thin, highly deformable, cross-hatched structures interspersed between the annular pulleys, designed to collapse and expand, thereby permitting unhindered digital flexion while maintaining continuous sheath coverage.
From a reconstructive and biomechanical standpoint, the A2 pulley (located over the proximal half of the proximal phalanx) and the A4 pulley (located over the middle third of the middle phalanx) are the most critical determinants of digital kinematics. Loss or incompetence of these crucial pulleys results in the biomechanical catastrophe known as "bowstringing." During active flexion, the unconstrained tendons displace volarly, pulling away from the center of joint rotation. This volar displacement significantly increases the moment arm of the tendon. While an increased moment arm paradoxically increases the theoretical mechanical advantage (force of flexion), it severely depletes the available linear tendon excursion. Because the muscle belly has a finite amplitude of contraction, this excursion is rapidly exhausted before full joint flexion is achieved, resulting in a profound, disabling loss of active PIP and DIP joint motion, accompanied by a secondary flexion contracture.
Furthermore, the anatomical preservation of the vascular supply to the tendons is paramount. The FDS and FDP tendons receive nutrition through a dual mechanism: intrinsic vascular perfusion via the vincula (vincula longa and brevia) and extrinsic diffusion from the synovial fluid within the sheath. The vincula enter the tendons dorsally, carrying delicate branches from the digital arteries. During a two-stage reconstruction, the native vascularity is invariably sacrificed during the radical excision of the scarred tendons. Consequently, the survival and incorporation of the subsequent tendon graft rely entirely on the rapid revascularization from the newly formed pseudo-sheath and the diffusion of nutrients from the surrounding bed, underscoring the absolute necessity of creating a healthy, well-vascularized soft-tissue envelope during Stage I.
Exhaustive Indications and Contraindications
The decision to embark on a two-stage flexor tendon reconstruction is a major clinical undertaking that requires rigorous patient evaluation. Primary or delayed primary repair remains the gold standard for acute tendon lacerations, yielding superior functional outcomes and minimizing surgical morbidity. However, when the native tendon bed is compromised beyond the salvageable limits of primary repair or single-stage grafting, the two-stage Hunter rod technique becomes the definitive reconstructive option. The primary indication is excessive, unyielding scarring of the flexor tendon sheath, typically seen in Zone II ("No Man's Land"), where the FDS and FDP tendons are tightly constrained within the fibro-osseous tunnel.
Concomitant digital pathology frequently dictates the necessity for a staged approach. Patients presenting with severe joint stiffness, profound flexion contractures, or compromised soft tissue envelopes require intensive preparatory interventions. Stage I not only allows for the placement of the silicone spacer but also facilitates concurrent procedures such as volar plate releases, collateral ligament excisions, digital nerve grafting, and soft tissue coverage via local or regional flaps. The silicone rod acts as an inert spacer, preventing the newly reconstructed soft tissues from adhering to the skeletal plane while the patient undergoes aggressive hand therapy to restore passive joint mobility prior to Stage II grafting.
Despite its utility, two-stage reconstruction is fraught with potential pitfalls and carries strict contraindications. The most absolute contraindication is an irrecoverably stiff digit. If full passive range of motion cannot be achieved either preoperatively or intraoperatively during Stage I through capsulotomies, placing a tendon graft will be entirely futile; a tendon graft cannot motor a rigid joint. Additionally, severe neurovascular insufficiency that threatens the viability of the digit, or a patient who lacks the cognitive capacity or psychological resilience to adhere to a stringent, months-long rehabilitation protocol, should be steered toward alternative salvage procedures. In such cases, digital arthrodesis, tenodesis, or even ray amputation may provide a more functional, pain-free, and reliable outcome.
| Category | Specific Clinical Scenarios | Rationale / Considerations |
|---|---|---|
| Primary Indications | Failed primary flexor tendon repair with dense Zone II adhesions. | Native gliding bed is destroyed; requires pseudo-sheath induction. |
| Delayed presentation of Zone II lacerations with segmental tendon loss. | Primary end-to-end repair impossible; single-stage graft prone to adhesion. | |
| Severe crush injuries with destruction of the A2 and A4 pulleys. | Requires staged pulley reconstruction over a passive implant. | |
| Suppurative flexor tenosynovitis resulting in tendon necrosis. | Infection must be eradicated; sheath must be biologically reconstituted. | |
| Relative Contraindications | Moderate joint stiffness unresponsive to preoperative therapy. | Requires extensive intraoperative capsulotomies during Stage I. |
| Single-vessel digit or compromised venous drainage. | Surgical trauma of radical tenosynovectomy may precipitate ischemia. | |
| Advanced patient age with low functional demands. | The grueling rehab protocol may outweigh the functional benefits. | |
| Absolute Contraindications | Irrecoverable, rigid joint contractures (ankylosis). | A tendon graft cannot move a mechanically locked joint; favor arthrodesis. |
| Severe, uncorrectable vascular insufficiency. | High risk of digital necrosis; amputation or conservative care preferred. | |
| Non-compliant patient or active substance abuse. | Inability to follow complex rehab protocols guarantees surgical failure. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of a successful two-stage reconstruction. The clinical examination must be exhaustive, focusing on the assessment of passive joint mobility, neurovascular status, and the integrity of the proximal motor units. The Boyes test and dynamic tenodesis evaluations are utilized to assess the amplitude and viability of the proximal muscle bellies in the forearm. If the native FDP or FDS muscle bellies have contracted, fibrosed, or lost their excursion due to prolonged disuse, alternative motor donors (such as adjacent FDS tendons or wrist flexors) must be identified and templated prior to surgery.
Radiographic evaluation is mandatory to assess the skeletal architecture, identify occult fractures, and evaluate the joint spaces for post-traumatic arthrosis. In cases of severe crush injuries, advanced imaging such as MRI or high-resolution ultrasound can be employed to map the extent of the fibro-osseous destruction and assess the continuity of the annular pulleys, though direct intraoperative visualization remains the gold standard. Furthermore, the surgeon must ensure that a comprehensive inventory of Hunter rods (varying in diameter from 3 mm to 6 mm) and appropriate tendon harvesting equipment (e.g., Brand tendon strippers) are available in the operative suite.
The evolution of anesthesia in hand surgery has profoundly impacted the execution of Stage II grafting. While Stage I is traditionally performed under regional anesthesia (axillary or supraclavicular block) with a proximal pneumatic tourniquet to facilitate meticulous dissection in a bloodless field, Stage II is increasingly performed utilizing the Wide Awake Local Anesthesia No Tourniquet (WALANT) technique. By infiltrating the surgical sites with a mixture of lidocaine and epinephrine, the surgeon achieves profound hemostasis and analgesia without paralyzing the forearm musculature. This allows for intraoperative, dynamic active tensioning of the tendon graft, drastically reducing the incidence of postoperative flexion contractures or extensor lags.
Patient positioning requires the patient to be supine with the affected upper extremity extended on a radiolucent hand table. For Stage I, a well-padded proximal arm tourniquet is applied. The entire upper extremity, from the fingertips to the axilla, is prepped and draped to allow for potential proximal extension of the incisions and simultaneous harvesting of autologous grafts (such as the palmaris longus or a strip of extensor retinaculum). Loupe magnification (minimum 2.5x to 3.5x) and precise microsurgical instrumentation are essential for the delicate dissection required to preserve the digital neurovascular bundles while performing a radical excision of the scarred flexor apparatus.
Step-by-Step Surgical Approach and Fixation Technique
Stage I: Tenosynovectomy and Implant Placement
The primary objective of the first stage is to prepare a pristine, unencumbered bed for the future tendon graft. The surgical approach typically utilizes a Bruner zigzag or a midlateral incision. The Bruner incision provides extensile, panoramic exposure of the volar digit, but the apex of the flaps must be carefully designed to avoid crossing the flexion creases at right angles, which could precipitate scar contractures. Once the skin flaps are elevated, the neurovascular bundles are identified, mobilized, and protected with vessel loops. The fibro-osseous sheath is then critically evaluated. The surgeon must meticulously excise the dense, restrictive scar tissue while preserving any native, pliable portions of the sheath, particularly the A1 pulley in the palm and the A5 pulley distally.
Following the exposure, a radical tenosynovectomy is performed. The scarred remnants of the FDS and FDP tendons are sharply excised from the distal phalanx down to the palm. It is imperative to trace the proximal tendon stumps into the palm or distal forearm through a separate counter-incision. The FDS is typically excised entirely, while the proximal stump of the FDP is retained. Crucially, the FDP stump must be left attached to the lumbrical muscle in the palm to prevent proximal retraction, maintain the resting length of the muscle belly, and prevent the paradoxical "lumbrical plus" finger deformity.
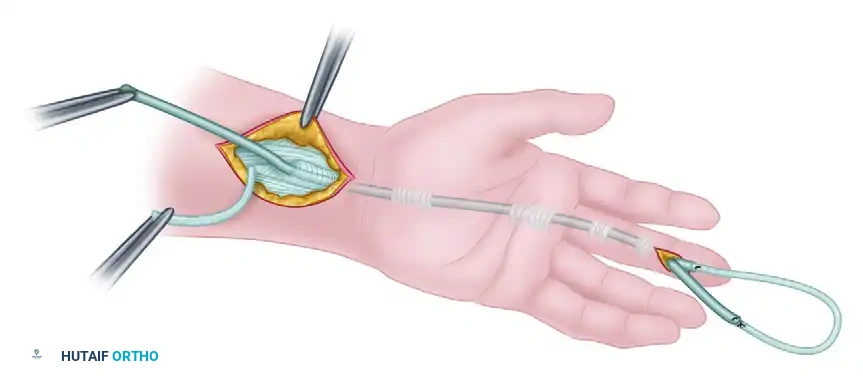
Once the bed is prepared, a Dacron-impregnated silicone rod (Hunter prosthesis) is selected. The rod must be sized accurately; it should glide passively within the reconstructed sheath without buckling or causing excessive friction against the retinacular restraints. The rod is secured distally to the robust stump of the profundus tendon or directly to the distal phalanx using a micro-suture anchor or a transosseous suture. The proximal end of the rod is then passed through the carpal tunnel and positioned in a healthy, scar-free soft-tissue bed in the distal forearm, approximately 5 cm proximal to the wrist crease, ensuring it does not tether during passive wrist and digital motion.
Stage I: Techniques for Pulley Reconstruction
If the native A2 and A4 pulleys are deemed incompetent, avulsed, or destroyed during the trauma, they must be meticulously reconstructed over the silicone rod to prevent postoperative bowstringing. Reconstruction typically utilizes a free tendon graft, such as the palmaris longus, plantaris, or a strip of the excised FDS tendon. Several robust techniques are available, chosen based on the integrity of the remaining fibro-osseous rim.
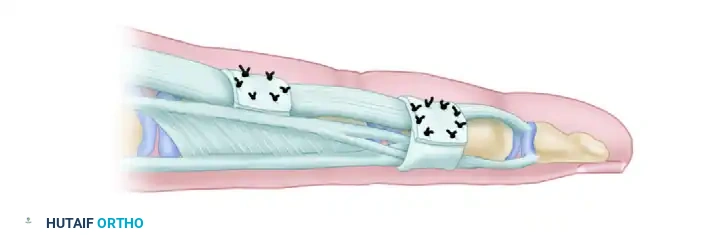
Technique A: Weaving Through an Intact Fibro-osseous Rim
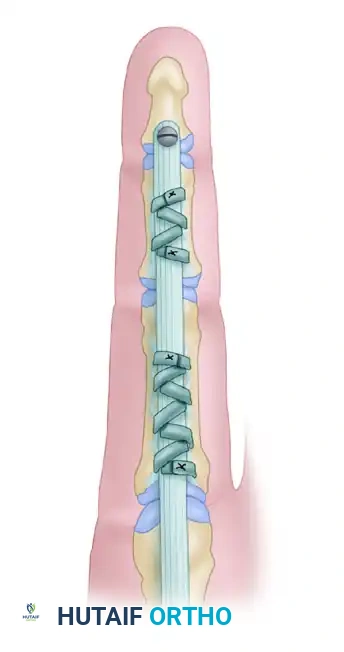
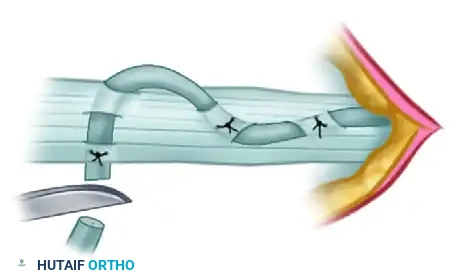
When the original fibro-osseous rim of the flexor sheath remains firmly anchored to the periosteum, it serves as an excellent foundation for reconstruction. The free tendon graft is woven directly through this native rim. The graft is passed through the rim on one side, draped over the silicone rod, and threaded through the rim on the contralateral side. This weave is then doubled back and secured to itself using multiple non-absorbable mattress sutures, creating a sturdy, low-profile pulley.
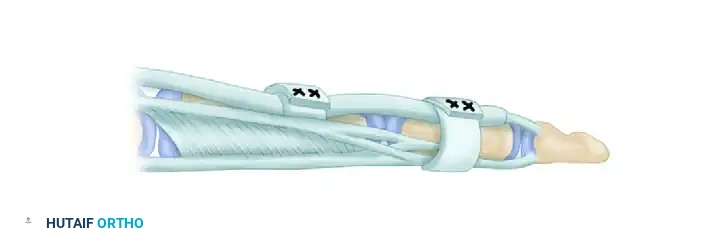
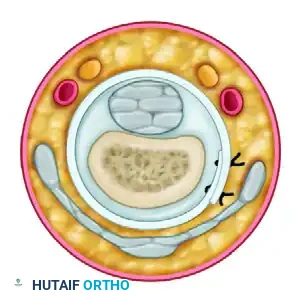
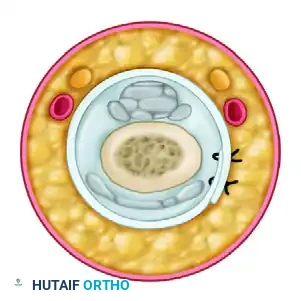
Technique B: Circumferential Phalangeal Reconstruction
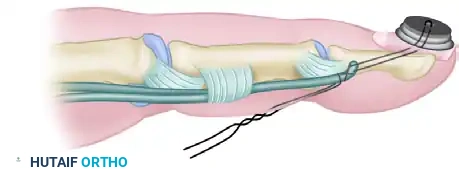
In scenarios involving severe crush injuries where the fibro-osseous rim is completely avulsed or insufficient to hold a suture, the tendon graft must be passed circumferentially around the phalanx. For the A2 Pulley (Proximal Phalanx), the graft is passed over the silicone rod and circumferentially around the bone. It is an absolute biomechanical imperative that the graft passes deep to the extensor tendon mechanism to avoid tethering extensor excursion and causing an extensor lag. Conversely, for the A4 Pulley (Middle Phalanx), the graft is passed circumferentially but must be routed superficial to the extensor tendon (lateral bands). Passing it deep at this level would compress and interfere with the delicate distal extensor mechanism, leading to a boutonniere or mallet deformity.
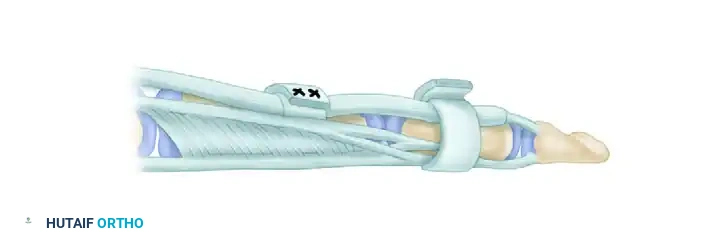
A critical surgical pitfall in circumferential reconstruction is the placement of the suture knot. The suture line inherently represents the weakest point and the bulkiest portion of the reconstructed pulley. After securing the graft to itself with multiple mattress sutures under appropriate tension, the surgeon must rotate the reconstructed pulley ring so that the bulky suture knot lies along the lateral or dorsal-lateral aspect of the digit. This ensures the knot is positioned far away from the direct volar gliding surface of the silicone rod, preventing mechanical impingement.
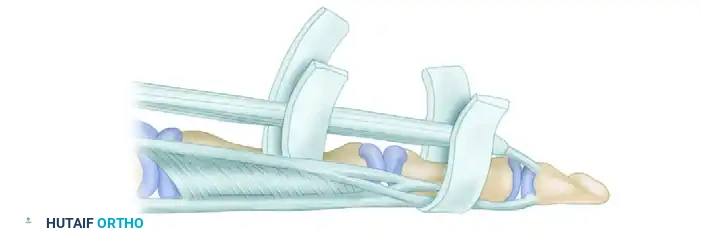
Technique C: Extensor Retinaculum Graft (Lister's Technique)
An elegant alternative for pulley reconstruction is the use of a strip of extensor retinaculum harvested from the dorsal wrist. The retinaculum is highly advantageous because it provides a smooth, pre-formed, anatomically native synovial gliding surface. The surgeon uses a piece of heavy silk suture passed around the finger to accurately template the required length and width of the graft before harvesting. The retinaculum is then wrapped around the phalanx and secured to the remaining periosteal rim, ensuring the smooth synovial surface faces inward toward the silicone rod.
Stage II: Tendon Grafting and Anastomosis
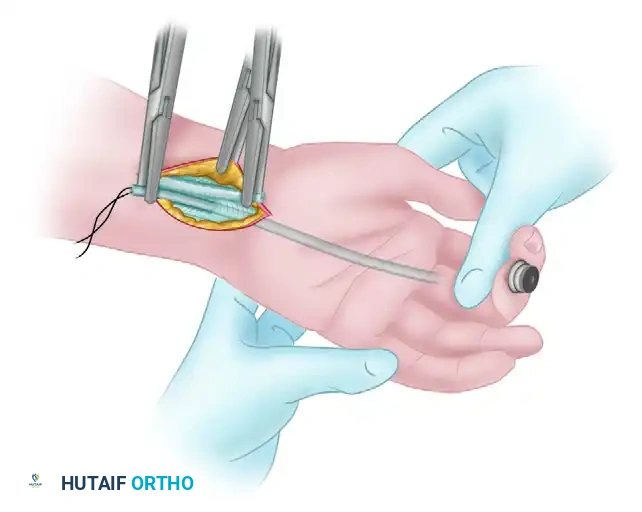
Stage II is typically executed approximately 3 to 4 months following Stage I. This deliberate delay is biologically necessary to allow for the complete resolution of digital edema, the rigid healing of the reconstructed A2 and A4 pulleys, and, most importantly, the maturation of the biologically active pseudo-synovial sheath around the silicone implant. The procedure begins by reopening the distal digital incision to expose the distal fixation of the rod, followed by opening the proximal forearm incision to locate the proximal end of the rod.
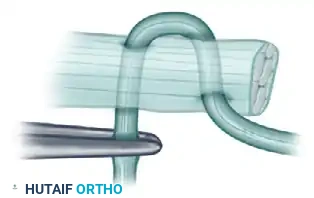
A suitable autologous tendon graft is harvested. The palmaris longus is the graft of choice due to its ideal diameter and minimal donor site morbidity; however, if absent, the plantaris tendon or a long toe extensor can be utilized. The proximal end of the harvested tendon graft is sutured securely to the proximal end of the silicone prosthesis in the forearm. The surgeon then applies gentle, steady traction to the distal end of the prosthesis in the finger. As the prosthesis is withdrawn distally, it acts as a leader, seamlessly pulling the tendon graft through the newly formed pseudo-sheath and safely beneath the reconstructed annular pulleys without traumatizing the delicate synovial lining.
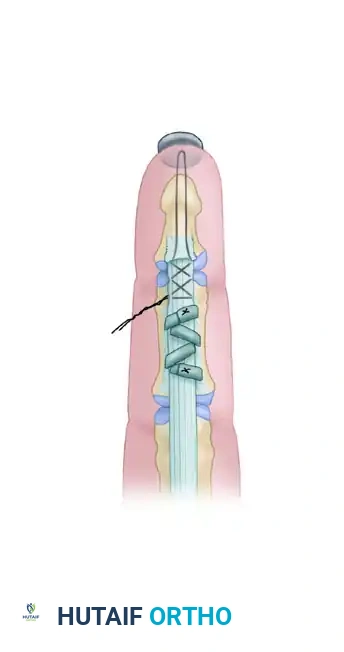
The distal anastomosis must be exceptionally robust to withstand the tensile forces of early active motion protocols. The distal end of the tendon graft is secured to the distal phalanx or the robust remaining stump of the FDP. A classic Bunnell pull-out suture technique is frequently employed. A non-absorbable suture is woven through the distal graft, passed through drill holes in the distal phalanx, and tied over a padded button resting on the sterile matrix of the fingernail. Reinforcing micro-sutures are subsequently placed circumferentially through the remaining stump of the profundus tendon to augment the repair and smooth the transition zone.
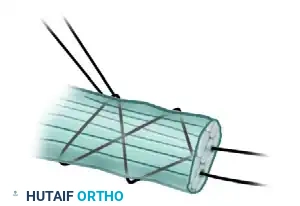
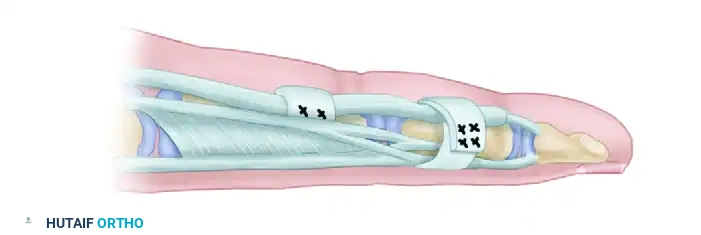
Setting the correct tension at the proximal anastomosis is arguably the most technically demanding aspect of the entire two-stage reconstruction. Incorrect tensioning will result in catastrophic functional failure: excessive tension yields a severe flexion contracture, while insufficient tension results in a profound lag in active flexion. A Pulvertaft weave is utilized for the proximal anastomosis to provide maximum biomechanical strength. The stump of the motor tendon (usually the native FDP) is "fish-mouthed," and the graft is threaded through the motor tendon two to three times at alternating 90-degree angles.


If the procedure is performed under general or regional anesthesia, the tension is set by observing the natural tenodesis effect of the hand; the reconstructed digit should rest in slightly more flexion than its normal position in the natural digital cascade. However, if performed under WALANT, the true amplitude of active muscle contraction can be directly observed. The patient is instructed to actively flex and extend the digit while the graft is held with a single temporary suture. The surgeon can dynamically adjust the tension in real-time. Once optimal tension and full excursion are confirmed, the Pulvertaft weave is formalized with multiple non-absorbable mattress sutures.
Complications, Incidence Rates, and Salvage Management
Despite flawless surgical technique, two-stage flexor tendon reconstruction carries a formidable complication profile. The procedure demands navigating a precarious biological tightrope: the reconstructed tissues must heal with sufficient tensile strength to prevent rupture, yet remain supple enough to prevent restrictive adhesions. The most common complication is the recurrence of dense peritendinous adhesions, particularly at the proximal and distal anastomotic sites, which can severely restrict active excursion. Adhesion formation is exacerbated by prolonged immobilization, aggressive surgical handling of the graft, or postoperative hematoma formation within the pseudo-sheath.
Rupture of the tendon graft or failure of the reconstructed pulleys represents a catastrophic mechanical failure. Graft rupture typically occurs at the proximal Pulvertaft weave or the distal pull-out insertion, often precipitating during the intermediate phase of rehabilitation (weeks 4-6) when the intrinsic tensile strength of
