Masterclass in Flexor Tendon Repair: Zones I and II Surgical Techniques
Key Takeaway
Flexor tendon injuries in Zones I and II demand meticulous surgical technique to restore digital biomechanics and prevent adhesions. Zone I repairs focus on the flexor digitorum profundus insertion, while Zone II—historically termed "no man's land"—requires precise management of both the profundus and sublimis tendons within the fibroosseous sheath. Successful outcomes rely on atraumatic tendon retrieval, robust multi-strand core suturing, preservation of the A2 and A4 pulleys, and early active motion protocols.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of flexor tendon lacerations, particularly within Zones I and II, represents one of the most exacting, unforgiving, and technically demanding challenges in the entirety of hand surgery. Historically, Zone II was famously dubbed "no man's land" by the pioneering surgeon Sterling Bunnell. This ominous moniker was earned due to the exceptionally high rates of postoperative adhesions, tendon ruptures, and universally poor functional outcomes following primary repair attempts in the mid-20th century. During that era, the standard of care often defaulted to wound closure followed by delayed secondary tendon grafting. Today, however, paradigm-shifting advancements in our understanding of tendon nutrition, the biomechanics of the fibroosseous sheath, multi-strand core suturing techniques, and early active motion (EAM) protocols have completely revolutionized the standard of care, firmly establishing primary repair as the absolute gold standard.
To fully appreciate the modern approach to flexor tendon repair, one must understand the dual mechanisms of tendon healing: intrinsic and extrinsic. Historically, it was believed that tendons healed exclusively via extrinsic mechanisms, relying entirely on the ingrowth of peritendinous fibroblasts and vascular buds from the surrounding sheath and soft tissues. This extrinsic healing is the primary driver of restrictive adhesion formation, which binds the tendon to the sheath and obliterates digital excursion. Modern research has definitively proven that flexor tendons possess a robust intrinsic healing capacity mediated by epitenon-derived and endotenon-derived tenocytes. By utilizing atraumatic surgical techniques, preserving the synovial sheath, and implementing early active motion, surgeons can stimulate this intrinsic healing pathway while simultaneously suppressing the adhesion-forming extrinsic pathway.
Epidemiologically, flexor tendon injuries predominantly affect the young, working-age population, with a significant male predominance. The vast majority of these injuries are the result of sharp lacerations from knives, glass, or industrial machinery. The socioeconomic impact of these injuries is profound, often resulting in prolonged absences from work and permanent disability if managed suboptimally. Therefore, the ultimate goal of flexor tendon repair is not merely anatomical continuity, but rather the creation of a biomechanical construct strong enough to withstand the forces of early active motion while maintaining a low-profile, streamlined repair site that glides seamlessly through the preserved, unyielding pulley system. Achieving this delicate balance requires meticulous surgical precision, profound anatomical knowledge, and a rigorously controlled rehabilitation environment.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of flexor tendon anatomy and its surrounding biomechanical envelope is absolutely non-negotiable for successful surgical repair. The flexor tendons of the hand are enclosed within a highly specialized, double-walled synovial sheath that provides both essential nutrition (via synovial fluid diffusion) and a low-friction gliding environment critical for digital excursion. This synovial sheath is externally reinforced by a complex, dense retinacular system composed of five annular (A1 through A5) and three cruciate (C1 through C3) pulleys. The annular pulleys are rigid, transverse bands of fibrous tissue that hold the tendons closely apposed to the phalanges, while the cruciate pulleys are thin, highly compliant, crisscrossing fibers that allow the sheath to collapse and expand during digital flexion without buckling.
Biomechanically, the A2 and A4 pulleys are the most critical components of the fibroosseous canal. The A2 pulley arises from the periosteum of the proximal half of the proximal phalanx, while the A4 pulley arises from the mid-portion of the middle phalanx. These structures are essential for preventing tendon bowstringing and maintaining the mechanical advantage (moment arm) of the flexor tendons. Loss of the A2 or A4 pulley results in an immediate increase in the moment arm, which paradoxically decreases the functional excursion of the tendon, leading to a profound loss of active interphalangeal joint flexion and a simultaneous loss of grip strength. Therefore, the absolute preservation or anatomical reconstruction of the A2 and A4 pulleys during surgical exploration is a fundamental tenet of hand surgery. Conversely, the thin, filamentous C1, C2, and C3 pulleys are highly compliant and represent the optimal sites for surgical incisions (sheath windows) to access retracted tendons without compromising digital biomechanics.
In Zone II, the anatomical relationship between the Flexor Digitorum Superficialis (FDS) and the Flexor Digitorum Profundus (FDP) is uniquely complex. At the level of the proximal third of the proximal phalanx, the FDS bifurcates into two distinct slips, creating a portal that allows the FDP to pass from deep to superficial. The two slips of the FDS then rotate 180 degrees—a phenomenon known as the FDS spiral—before decussating to insert into the volar base of the middle phalanx. This intricate crossing creates Camper's chiasm. Failure to recognize and anatomically restore this exact spiral orientation during FDS repair will inevitably result in a twisted, bulky repair that acts as a mechanical block, irrevocably binding the FDP tendon within the narrow sheath.
Furthermore, the vascular supply to the flexor tendons within the digital sheath is highly specialized and precarious. The tendons receive blood via a segmental system of vincular vessels (Vincular Brevis Profundus, Vincula Longa Profundus, Vincular Brevis Superficialis, and Vincula Longa Superficialis) which arise from the transverse communicating branches of the proper digital arteries. These vessels enter the tendons strictly on their dorsal surface. Consequently, surgical dissection, core suture placement, and tendon handling must be rigorously confined to the volar, lateral, and cut surfaces of the tendon to avoid devascularizing the intrinsic tendon substance. Disruption of the vincular supply forces the tendon to rely entirely on synovial diffusion, significantly delaying the proliferative phase of intrinsic healing and increasing the risk of late rupture.
Exhaustive Indications and Contraindications
The decision-making process for flexor tendon repair is dictated by the timing of the injury, the mechanism of trauma, the degree of wound contamination, and the overall physiological status of the patient. Primary repair, performed within the first 24 to 48 hours of injury, is the absolute gold standard and yields the most superior functional outcomes. Delayed primary repair, performed between 2 and 14 days post-injury, is also highly successful and is often indicated when the initial presentation is delayed, or when the wound requires a period of serial debridement for marginal contamination. Beyond 14 to 21 days, the proximal muscle belly begins to undergo myostatic contracture, the tendon ends become edematous and friable, and the synovial sheath collapses, often precluding a direct end-to-end repair without excessive, ischemia-inducing tension.
Secondary repair (beyond 3-4 weeks) is rarely successful as a single-stage procedure in Zones I and II. In these chronic scenarios, the surgeon must carefully evaluate the integrity of the pulley system, the suppleness of the interphalangeal joints, and the availability of a viable proximal muscle unit. If the joints are stiff or the pulley system is destroyed, a two-stage tendon reconstruction utilizing a silicone Hunter rod is mandated. The first stage reconstructs the pulley system and creates a pseudo-sheath, while the second stage (performed 3-6 months later) involves definitive tendon grafting (e.g., using the palmaris longus or plantaris tendon).
Absolute contraindications to primary flexor tendon repair include severe, untidy crush injuries with massive segmental tendon loss, gross purulent contamination, or injuries presenting with profound, unyielding joint contractures. Attempting primary repair in a heavily contaminated wound invites deep space infection, which will invariably destroy the tendon repair, the pulley system, and potentially the articular cartilage of the interphalangeal joints. In such cases, the initial management must focus exclusively on radical surgical debridement, skeletal stabilization, and soft tissue coverage, deferring tendon reconstruction until a clean, stable, and supple soft tissue envelope has been established.
| Category | Indications for Primary/Delayed Primary Repair | Contraindications for Primary Repair |
|---|---|---|
| Timing | Acute lacerations (< 14 days post-injury) | Chronic injuries (> 3-4 weeks) with myostatic contracture |
| Wound Status | Clean, sharp lacerations (e.g., knife, glass) | Gross contamination, purulence, or severe crush injuries |
| Soft Tissue | Adequate viable skin coverage available | Massive soft tissue avulsion requiring complex flap coverage |
| Skeletal | Stable fractures or easily fixable phalangeal fractures | Unstable, highly comminuted fractures precluding early motion |
| Joint Status | Supple passive range of motion in PIP and DIP joints | Severe pre-existing joint contractures or arthritis |
| Pulley System | Intact or primarily repairable A2 and A4 pulleys | Complete destruction of the fibroosseous sheath |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative clinical examination is the cornerstone of surgical planning. The surgeon must systematically isolate and test the FDS and FDP tendons of each digit. To test the FDS, the adjacent non-injured fingers are held in absolute, rigid extension to neutralize the common muscle belly of the FDP; the patient is then asked to flex the PIP joint of the injured finger. To test the FDP, the PIP joint of the injured finger is stabilized in extension by the examiner, and the patient is asked to actively flex the DIP joint. A thorough neurovascular examination, specifically assessing two-point discrimination and capillary refill, must be documented prior to the administration of any local anesthetic.
Knife laceration through Zone II with the digit in full flexion at the time of injury.
The posture of the hand at the exact moment of injury provides critical diagnostic information regarding the anticipated level of tendon retraction. If the digit was in full flexion when the laceration occurred (e.g., grasping a knife blade), the distal tendon stumps will have advanced distally when the finger was subsequently extended, often lying far distal to the skin wound. Conversely, if the finger was extended during injury, the tendon laceration will closely correspond to the level of the cutaneous wound. Understanding this dynamic relationship dictates the design of the surgical extensions required for adequate exposure.
In the modern era, the anesthetic approach to flexor tendon repair has undergone a paradigm shift with the advent of WALANT (Wide Awake Local Anesthesia No Tourniquet). Utilizing a mixture of lidocaine, epinephrine, and sodium bicarbonate, WALANT provides profound surgical anesthesia and a bloodless surgical field without the need for an ischemic pneumatic tourniquet. The paramount advantage of WALANT is the ability to communicate with the conscious patient intraoperatively. Once the repair is completed, the surgeon can ask the patient to actively flex and extend the digit. This allows for real-time visualization of the repair's tensile strength, confirms the absence of gapping under physiological load, and ensures that the repair glides smoothly through the pulley system without bunching or triggering.
Positioning for the procedure requires the patient supine with the operative extremity extended on a radiolucent hand table. The surgeon should be seated comfortably, utilizing loupe magnification (minimum 2.5x to 3.5x) and focal illumination. A meticulously organized Mayo stand equipped with fine, atraumatic hand instruments—including Adson forceps, tenotomy scissors, fine needle holders, pediatric feeding tubes (for tendon retrieval), and a variety of non-absorbable braided core sutures (e.g., 3-0 or 4-0 Supramid, FiberWire, or Tycron) and monofilament epitendinous sutures (5-0 or 6-0 Prolene or Nylon)—is essential for the efficient execution of the repair.
Step-by-Step Surgical Approach and Fixation Technique
Surgical Approach and Exposure in Zone I
Zone I extends from the insertion of the FDS on the middle phalanx to the insertion of the FDP on the distal phalanx. Injuries in this zone exclusively involve the FDP tendon. The surgical approach must provide wide, unhindered exposure while rigorously protecting the delicate neurovascular structures of the distal pulp.

Incision outlined on the digit and palm utilizing a classic volar zigzag (Bruner) approach.
The skin incision typically begins by extending the traumatic laceration. A classic volar zigzag (Bruner) approach or a midaxial incision is utilized. The Bruner incision uses perfectly angled flaps with the apices located at the flexion creases to prevent scar contracture. When elevating the skin flaps, dissection must remain either strictly dorsal or strictly volar to the neurovascular bundles to avoid devascularizing the skin or causing iatrogenic neuromas.
Exposure of the fibroosseous flexor tendon sheath after meticulous flap elevation.
Once the fibroosseous sheath is exposed, the surgeon must identify the proximal FDP stump. In Zone I injuries, the vincula brevis profundus may remain intact, preventing significant proximal retraction. However, if the vincula are torn, the FDP can retract into the palm, requiring a separate incision at the distal palmar crease for retrieval. When opening the sheath to access the tendon, it is absolutely critical to preserve the A4 pulley. A small L-shaped or trapdoor window is made in the C3 cruciate area to allow for delivery of the tendon.
If the distal stump of the FDP is longer than 1 cm, a true end-to-end multi-strand core repair is performed. However, if the laceration is flush with the distal phalanx insertion, the proximal stump must be advanced and directly reattached to the bone. Modern techniques utilize small suture anchors (e.g., 1.5mm or 2.0mm micro-anchors) placed into the volar base of the distal phalanx. Alternatively, antegrade pull-out techniques tying over a dorsal button can be used, though these carry a higher risk of nail bed deformity and pin-tract infections.

Closed incision demonstrating tension-free skin approximation.
Surgical Approach and Exposure in Zone II
Zone II extends from the proximal edge of the A1 pulley to the FDS insertion. Lacerations here frequently involve both the FDS and FDP tendons. The traumatic wound almost always requires proximal and distal extension to achieve adequate exposure of the retracted tendon stumps.
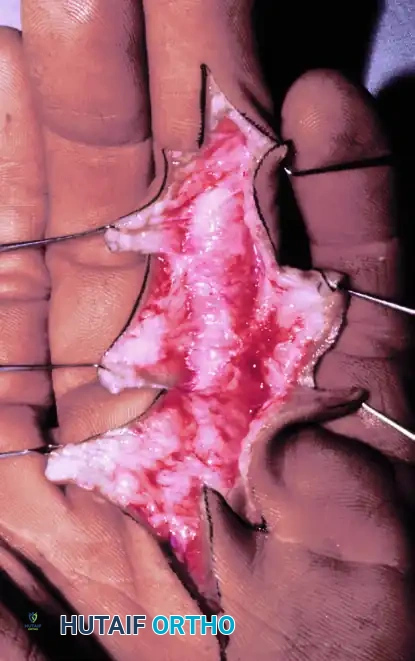
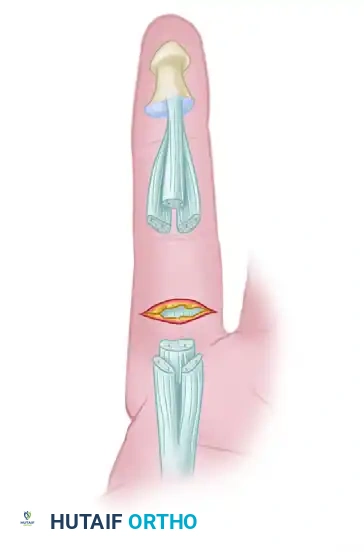
Level of flexor tendon retraction of the same finger after digital extension. Note the mismatch between the skin laceration and the tendon stumps.
Green lines depict radial and ulnar incisions to allow wide exposure of the flexor tendon system.
Careful reflection of the skin flaps is performed, meticulously identifying and protecting the digital nerves and arteries. If a digital nerve has been transected, its ends should be mobilized, cleanly sectioned, and tagged. Crucially, the definitive epineurial repair of the digital nerve must be delayed until after the flexor tendons have been completely repaired. Manipulating the digit to retrieve and suture tendons will inevitably disrupt a freshly repaired microscopic nerve anastomosis.

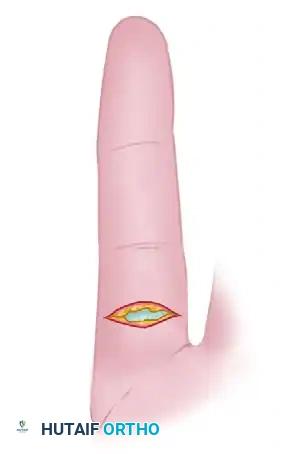
Flexor tendon system of the involved finger after reflection of skin flaps. The laceration has occurred through the C1 cruciate pulley area.
Sheath Management and Tendon Retrieval
Exposing the flexor sheath requires precision. The A2 and A4 pulleys must be identified and rigorously protected. If the sheath must be opened to retrieve the tendons, incisions are strictly limited to the filamentous cruciate areas (C1, C2, C3).
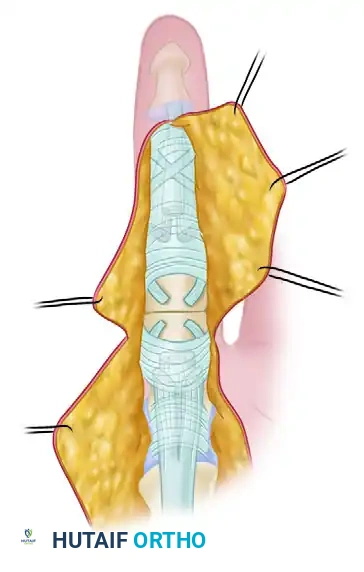
Reflection of small triangular flaps at the cruciate-synovial sheath allows distal flexor tendon stumps to be delivered into the wound.
Retrieving a retracted flexor tendon from the palm without causing iatrogenic trauma to the epitenon is a hallmark of surgical mastery. Blind grasping with heavy forceps inside the sheath is strictly prohibited. Instead, the surgeon should first attempt to "milk" the tendon distally by applying firm pressure from the proximal palm while passively flexing the wrist and MCP joints. If this fails, a pediatric feeding tube or a flexible plastic IV catheter is passed retrograde from the digital sheath into the palm. A separate palmar incision is made, the tendon is identified, and a core suture is placed into its tip. The suture is then threaded into the catheter, allowing the tendon to be gently "led" distally through the intact pulley system without friction or crush injury.
Tendon Stabilization and Core Suturing
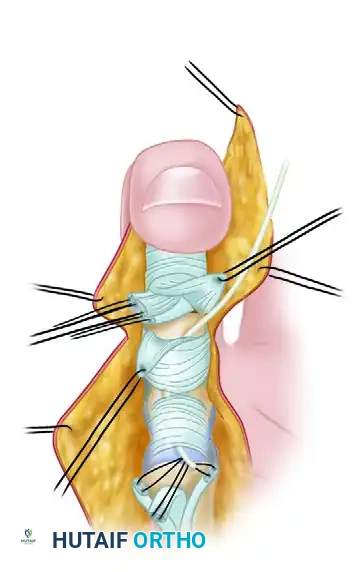
Once the proximal ends of the FDS and FDP are delivered into the repair window (usually between A2 and A4), they must be secured to prevent re-retraction, which would necessitate repeated, traumatic retrieval.
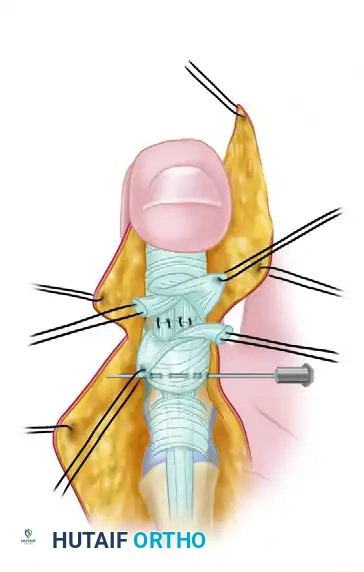
Proximal flexor tendon stumps are maintained at the repair site by means of a transversely placed small-gauge hypodermic needle.
A 25-gauge or 26-gauge hypodermic needle is passed transversely through the adjacent intact pulley or soft tissue, directly through the substance of the tendons, and out the opposite side. This effectively pins the tendons in place, completely removing tension from the repair site and allowing the surgeon to focus entirely on precise suture placement.
The FDS is repaired first to restore the anatomical floor of the sheath. The surgeon must meticulously respect the FDS spiral, ensuring that the proximal and distal stumps are matched perfectly without malrotation. The FDP is then repaired utilizing a robust, multi-strand core suture technique. Biomechanical studies have definitively shown that the tensile strength of a tendon repair is directly proportional to the number of core suture strands crossing the repair site. A minimum of a 4-strand repair (e.g., modified Kessler combined with a cruciate suture, or a Strickland 4-strand technique) is required to safely withstand the forces of early active motion. Many modern surgeons advocate for a 6-strand or even 8-strand repair (e.g., M-Tang technique) using 3-0 or 4-0 non-absorbable braided sutures. The core sutures should be placed in the volar half of the tendon to avoid compressing the dorsal vincular vascular supply, and the knots must be buried deep within the tendon interface to prevent friction against the sheath.
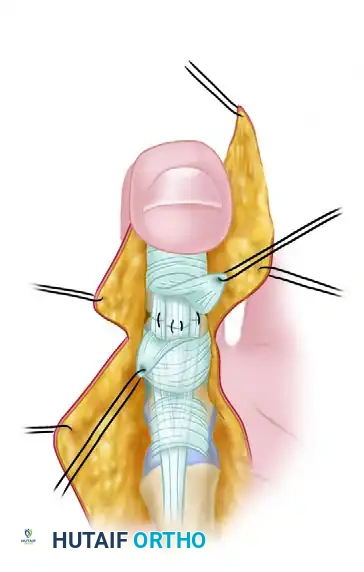
Completed repair of both tendons with the distal interphalangeal joint in full flexion.
Following the core repair, a circumferential epitendinous suture is absolutely mandatory. Using a 5-0 or 6-0 monofilament (e.g., Prolene), a running interlocking or cross-stitch technique is applied. This epitendinous suture serves two critical functions: first, it adds up to 30% to the overall tensile strength of the construct; second, and perhaps more importantly, it neatly tucks in the raw, fraying edges of the epitenon, dramatically reducing the cross-sectional area of the repair and significantly decreasing gliding resistance within the sheath.
Dynamic Testing and Closure
Upon completion of the epitendinous repair, the stabilizing hypodermic needles are removed. If the procedure is performed under WALANT, the patient is instructed to actively flex and extend the digit. The surgeon meticulously observes the repair as it glides under the intact pulley system.
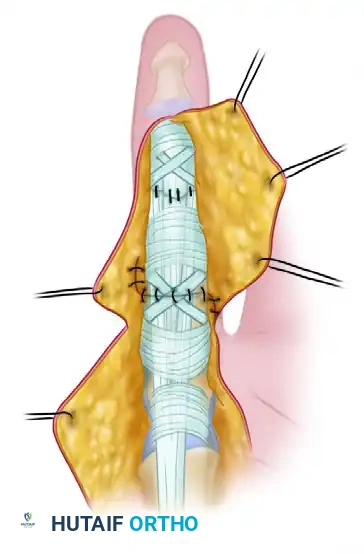
Extension of the distal interphalangeal joint delivers the repair under the intact distal flexor tendon sheath. Repair of the cruciate (C1) synovial pulley has been completed.
If any catching or triggering is observed, the epitendinous suture must be revised to smooth the profile. If the sheath window can be closed without constricting the tendon, it is repaired with 6-0 nylon to re-establish the synovial fluid boundary. Finally, the skin is closed with interrupted 5-0 nylon sutures, avoiding excessive tension that could lead to marginal necrosis.

Wound repair at the conclusion of the procedure, demonstrating excellent approximation of the Bruner flaps.
Complications, Incidence Rates, and Salvage Management
Despite flawless surgical execution, flexor tendon repairs in Zones I and II are fraught with potential complications. The surgeon is constantly walking a tightrope between two opposing catastrophic failures: restrictive adhesions (due to inadequate motion) and tendon rupture (due to excessive force or weak repair).
The "Strickland curve" of tendon healing demonstrates that a repaired tendon actually loses tensile strength during the early inflammatory and fibroblastic phases, reaching its absolute weakest point between days 5 and 21 postoperatively. It is during this critical window that the majority of ruptures occur. Ruptures typically present with a sudden, painless loss of active flexion, often accompanied by a palpable "pop." If a rupture is identified within the first 7 to 10 days, prompt surgical re-exploration and re-repair are indicated. However, late ruptures or repeated failures necessitate a two-stage tendon reconstruction.
Restrictive adhesions are the most common complication, presenting as a severe discrepancy between passive and active range of motion (i.e., the digit can be passively flexed, but active flexion is absent or severely limited). If aggressive hand therapy fails to progress motion by 3 to 6 months postoperatively, and the soft tissues are completely supple, a surgical tenolysis is indicated. Tenolysis is a highly demanding procedure requiring wide awake anesthesia (WALANT) to ensure the patient can actively demonstrate the release of adhesions intraoperatively.
Another unique complication is the "Lumbrical Plus" finger, which occurs when the FDP is transected distal to the lumbrical origin, or when an FDP graft is excessively long. When the patient attempts to flex the fingers, the proximal FDP stump pulls proximally, transmitting force through the intact lumbrical muscle. This paradoxically extends the PIP and DIP joints while flexing the MCP joint. Treatment involves surgical division of the offending lumbrical tendon.
| Complication | Estimated Incidence | Pathophysiology / Mechanism | Salvage Management |
|---|---|---|---|
| Tendon Rupture | 4% - 9% | Excessive force during weak phase (Days 5-21); inadequate core strands; knot unraveling | Early (<10 days): Direct re-repair. Late: Two-stage Hunter rod reconstruction. |
| Restrictive Adhesions | 15% - 30% | Extrinsic healing; poor post-op compliance; traumatic tissue handling; prolonged immobilization | Aggressive hand therapy. Surgical tenolysis after 3-6 months if plateaued. |
| PIP Joint Contracture | 10% - 20% | Imbalance of flexor/extensor forces; volar plate scarring; failure to achieve full passive extension | Dynamic extension splinting. Surgical volar plate release (capsulotomy) if refractory. |
| Bowstringing | Rare (<2%) | Iatrogenic destruction or failure to repair the A2 or A4 pulleys | Pulley reconstruction using extensor retinaculum or palmaris longus graft. |
| Lumbrical Plus Finger | Variable | FDP retraction drawing lumbrical proximally, causing paradoxical IP extension during attempted flexion | Surgical transection of the lumbrical tendon under local anesthesia. |
| Deep Infection | 1% - 3% | Contaminated wound; retained foreign body; poor vascularity of skin flaps | Urgent surgical I&D, removal of sutures, IV antibiotics. Defers repair to secondary grafting. |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of a Zone I or II flexor tendon repair relies just as heavily on the rigorous execution of a postoperative rehabilitation protocol as it does on the intraoperative surgical technique. The fundamental principle of modern rehabilitation is controlled stress. Mechanical loading of the healing tendon stimulates tenocyte proliferation, aligns collagen fibers longitudinally, and dramatically increases the ultimate tensile strength of the repair, all while preventing the formation of dense, restrictive peritendinous adhesions.
Immediately postoperatively, the limb is immobilized in a custom thermoplastic dorsal blocking splint. The precise positioning of this splint is critical to minimize resting tension on the repair: the wrist is positioned in 20 to 30 degrees of palmar flexion, the metacarpophalangeal (MCP) joints are placed in 70 degrees of flexion, and the interphalangeal (IP) joints are left in neutral extension. This posture effectively relaxes the musculotendinous units of the flexor compartment.
Modern rehabilitation heavily favors Early Active Motion (EAM) protocols, provided the surgeon has achieved a robust 4-strand or
