Staged Digital Flexor Tendon Reconstruction: An Intraoperative Masterclass
Key Takeaway
This masterclass guides fellows through staged flexor tendon reconstruction, a critical procedure for chronic Zone II injuries. We cover meticulous anatomical considerations, pre-operative planning, and granular, real-time surgical execution for both silicone rod placement and definitive tendon grafting. Emphasizing optimal tensioning, pulley reconstruction, and comprehensive postoperative care, this guide prepares you for successful outcomes in complex hand surgery.
Comprehensive Introduction and Patho-Epidemiology
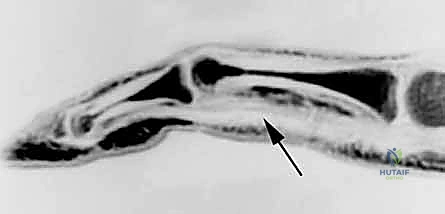
Staged digital flexor tendon reconstruction remains one of the most formidable challenges in the realm of orthopedic hand surgery. When dealing with neglected ruptures, delayed diagnoses, or the catastrophic failure of a primary flexor tendon repair, the surgeon is confronted not merely with a mechanical discontinuity, but with a profoundly altered biological environment. The concept of staged reconstruction, pioneered by James Hunter in the 1970s, revolutionized our approach to these complex injuries by acknowledging that a tendon graft cannot successfully glide within a scarred, obliterated fibro-osseous canal. This procedure is an exercise in biological re-engineering, requiring the surgeon to first cultivate a hospitable environment—a pseudosheath—before introducing a definitive biological graft.
The pathogenesis of flexor tendon repair failure, particularly within Zone II, is rooted in the delicate balance between intrinsic tendon healing and extrinsic scar formation. Following trauma or surgical intervention, the highly specialized synovial lining of the flexor sheath is frequently destroyed. The ensuing inflammatory cascade, driven by fibroblasts and macrophages, leads to the deposition of dense, disorganized collagen. This proliferative scar tissue bridges the gap between the healing tendon and the surrounding static structures (the sheath, pulleys, and phalanges), effectively tethering the tendon and obliterating the frictionless gliding interface. When a primary repair fails, or when a diagnosis is delayed beyond the window of primary repair (typically 3 to 4 weeks), the proximal muscle belly undergoes myostatic contracture, and the empty digital sheath collapses and scars down.
Attempting a single-stage tendon graft in such a compromised bed is biologically unsound; the graft will invariably become encased in scar tissue, resulting in a stiff, non-functional digit. The two-stage approach elegantly circumvents this. Stage 1 utilizes a biologically inert silicone elastomer rod to act as a spacer. Over a period of 3 to 6 months, the body responds to this foreign body by forming a smooth, mesothelial-lined fibrous capsule around it. This newly formed pseudosheath mimics the native synovial sheath, providing a frictionless conduit and a biologically favorable environment that limits extrinsic adhesions.
Without meticulous reconstruction, these injuries condemn the patient to a stiff, often painful digit that severely compromises overall hand mechanics. The loss of active flexion impairs grip strength and fine motor dexterity. Furthermore, the chronic imbalance of forces—specifically, unopposed extensor tone acting on an unstable digit—can precipitate secondary joint contractures, volar plate laxity, and debilitating hyperextension deformities at the proximal interphalangeal (PIP) joint. Therefore, staged reconstruction is not merely a salvage procedure; it is a vital restorative intervention demanding precise execution and an exhaustive understanding of hand biomechanics.
Detailed Surgical Anatomy and Biomechanics
Flexor Tendon Zones and Topography
A profound mastery of flexor tendon anatomy is the absolute prerequisite for any reconstructive endeavor in the hand. The volar aspect of the hand and forearm is classically divided into five distinct anatomical zones, a classification system that dictates both prognosis and surgical strategy.

Zone I extends distally from the insertion of the flexor digitorum superficialis (FDS) on the middle phalanx to the insertion of the flexor digitorum profundus (FDP) at the base of the distal phalanx. Injuries here isolate the FDP. Zone II, famously christened "no man's land" by Sterling Bunnell, spans from the proximal edge of the A1 pulley (at the metacarpal neck) to the FDS insertion. This zone is uniquely unforgiving because both the FDS and FDP tendons are tightly constrained within the narrow fibro-osseous sheath. The intimate relationship between the two tendons, coupled with the unyielding nature of the surrounding pulleys, maximizes the probability of adhesion formation following injury or surgery.
Zone III encompasses the region from the distal border of the transverse carpal ligament to the proximal edge of the A1 pulley. Here, the tendons are free of the restrictive digital sheath, often carrying a better prognosis for primary repair. Zone IV represents the carpal tunnel, where the nine flexor tendons and the median nerve are densely packed. Finally, Zone V extends proximally from the carpal tunnel into the distal forearm, encompassing the musculotendinous junctions. Understanding the precise boundaries and contents of these zones is critical when planning the proximal and distal incisions for rod placement and subsequent graft tensioning.
The Fibro-Osseous Sheath and Pulley System
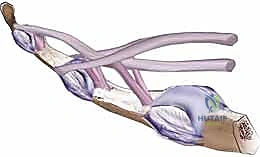
The flexor tendon sheath is a highly specialized, multi-layered structure that serves as a mechanical fulcrum, optimizing the work of flexion and preventing tendon bowstringing. It is composed of a continuous synovial lining reinforced by distinct condensations of fibrous tissue known as pulleys.
The annular (A) pulleys are rigid, transverse bands that provide primary mechanical support. There are five annular pulleys (A1-A5). The A2 pulley, located over the proximal half of the proximal phalanx, and the A4 pulley, situated over the middle third of the middle phalanx, are the most biomechanically critical. They are firmly anchored to the periosteum and are essential for maintaining the tendons close to the axis of joint rotation. Loss or incompetence of the A2 or A4 pulleys results in bowstringing—a phenomenon where the tendon pulls away from the bone during flexion. This drastically increases the moment arm, requiring greater tendon excursion to achieve the same degree of joint flexion, ultimately resulting in a profound loss of active range of motion and grip strength.
The cruciate (C) pulleys (C1-C3) are thin, cross-hatched structures located between the annular pulleys. They are highly flexible and collapse during digital flexion, allowing the sheath to accommodate the changing geometry of the flexing digit without buckling. During Stage 1 reconstruction, the surgeon must meticulously preserve or reconstruct the A2 and A4 pulleys to ensure the biomechanical viability of the future graft.
Vascularity and Camper's Chiasm
The blood supply to the flexor tendons within the digital sheath is dual in nature, relying on both extrinsic vascular perfusion and intrinsic synovial diffusion. The extrinsic supply is delivered via the vincula tendinum—delicate folds of mesotenon that carry vessels from the digital arteries to the dorsal aspect of the tendons. There are typically two vincula brevia (short, robust bands near the insertions of the FDS and FDP) and two vincula longa (longer, more proximal bands). Surgical dissection must be exquisitely careful to avoid damaging these fragile structures, as devascularization leads to tendon necrosis and catastrophic rupture.
Adding to the anatomical complexity of Zone II is Camper's chiasm. At the level of the proximal phalanx, the FDS tendon flattens and bifurcates into two slips that pass dorsally around the centrally located FDP tendon. These slips decussate (cross over) dorsal to the FDP before inserting into the volar aspect of the middle phalanx. This intricate three-dimensional relationship creates a highly constrained environment where the FDP must glide smoothly through the FDS bifurcation. In the setting of trauma, this area is a prime nidus for dense, cross-adhesion formation, often necessitating the excision of the FDS remnants during Stage 1 reconstruction to create adequate space for the silicone rod and subsequent graft.
Exhaustive Indications and Contraindications
Patient selection is arguably the most critical determinant of success in staged flexor tendon reconstruction. The procedure is technically demanding, necessitates a prolonged and arduous rehabilitation protocol, and carries a significant risk of complications. Therefore, the surgeon must rigorously evaluate both the biological status of the digit and the psychological readiness of the patient. Boyes' preoperative factors—which include patient age, the extent of scarring, joint mobility, and the status of digital nerves—must be carefully weighed.
The ideal candidate presents with an isolated loss of FDP and FDS function in a digit that is otherwise supple, well-perfused, and sensate. The soft tissue envelope must be of high quality; severe scarring, compromised vascularity, or inadequate volar skin coverage will doom the reconstruction. Crucially, the patient must possess nearly full passive range of motion (PROM) in the metacarpophalangeal (MCP), PIP, and distal interphalangeal (DIP) joints. Tendon reconstruction cannot overcome joint contractures; any stiffness must be aggressively addressed with hand therapy prior to surgical intervention.
| Category | Specific Clinical Parameters |
|---|---|
| Primary Indications | Delayed presentation (>4 weeks) of Zone II FDP/FDS rupture. |
| Failed primary flexor tendon repair with dense adhesion formation. | |
| Segmental tendon loss following trauma or tumor resection. | |
| Supple joints with full or nearly full passive range of motion. | |
| Intact or reconstructable digital neurovascular bundles. | |
| Absolute Contraindications | Active or untreated local infection (e.g., flexor tenosynovitis). |
| Severe, unyielding joint contractures (ankylosis). | |
| Inadequate or severely compromised soft tissue coverage. | |
| Ischemic digit with non-reconstructable vascular inflow. | |
| Non-compliant patient unable to adhere to strict rehabilitation. | |
| Relative Contraindications | Advanced physiological age with low functional demands. |
| Intact, fully functional FDS with isolated chronic FDP rupture (risk of FDS compromise). | |
| Severe concomitant skeletal trauma requiring complex fixation. |
Active infection is an absolute contraindication. The presence of bacteria within the closed space of the flexor sheath or around a silicone implant will lead to rampant destruction of the soft tissues and inevitable failure. Any suspected infection must be treated with aggressive surgical débridement, copious irrigation, and targeted intravenous antibiotics. Only after the infection has been definitively eradicated and the soft tissue envelope has normalized can the surgeon entertain the possibility of staged reconstruction.
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive Clinical Evaluation
The preoperative assessment begins with a meticulous physical examination. The surgeon must evaluate the resting cascade of the hand; a normal hand exhibits progressively increasing flexion from the index to the small finger. A disruption in this cascade immediately signals a flexor tendon injury. Specific testing of the FDS and FDP must be performed to isolate the level of dysfunction. The tenodesis effect—passive finger flexion upon active wrist extension—should be assessed; its absence confirms discontinuity of the flexor system.
Equally important is the assessment of the digital soft tissue envelope. The skin must be supple, well-vascularized, and free of active inflammation. The surgeon must meticulously map the distribution of previous surgical scars, as these will dictate the approach for Stage 1. A thorough neurovascular examination is mandatory. Two-point discrimination should be recorded for both the radial and ulnar digital nerves. If a digital nerve injury is identified, plans must be made for concurrent nerve repair or grafting during the Stage 1 procedure, as protective sensation is vital for the functional utility of the reconstructed digit.
Graft Selection and Donor Site Templating
Preoperative planning must include a definitive strategy for graft harvest during Stage 2. The ideal tendon graft is long, thin, strong, and readily available without causing significant donor site morbidity.
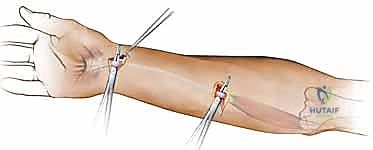
- Palmaris Longus (PL): This is the gold standard and first choice. It is present in approximately 85% of the population. It provides adequate length for a single digit reconstruction and its harvest leaves no functional deficit. Its presence should be confirmed preoperatively by asking the patient to oppose the thumb and small finger while flexing the wrist.
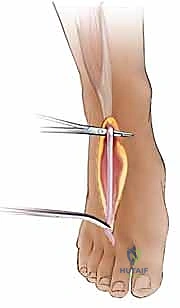
- Plantaris Tendon: If the PL is absent or if multiple digits require reconstruction, the plantaris tendon is an excellent alternative. It is the longest tendon in the body, providing ample material. Its harvest requires a small incision at the medial malleolus and the use of a tendon stripper.
- Extensor Digitorum Longus (EDL) of the Toes: The EDL tendons to the second, third, or fourth toes can be utilized. They provide excellent length and strength, though harvest requires a longer incision on the dorsum of the foot and carries a slightly higher risk of donor site morbidity.
- Extensor Indicis Proprius (EIP): Useful when a shorter graft is needed, though its harvest slightly weakens independent index finger extension.
Operating Room Setup
The patient is positioned supine on the operating table. The operative arm is abducted and supported on a radiolucent hand table. A non-sterile pneumatic tourniquet is applied to the proximal arm over adequate padding. This is critical for maintaining a bloodless surgical field, which is absolutely essential for the meticulous dissection of scarred neurovascular structures and the preservation of delicate pulleys.
The surgeon and assistant sit opposite each other. Loupe magnification (typically 2.5x to 3.5x) is mandatory for both stages. A C-arm fluoroscopy unit should be draped and available in the room, particularly for Stage 2, to assist in confirming the placement of distal fixation anchors if utilized. If a lower extremity donor site (plantaris or toe extensor) is planned, the ipsilateral leg must be prepped, draped, and exposed simultaneously with the upper extremity.
Step-by-Step Surgical Approach and Fixation Technique
Stage 1: Pseudosheath Creation and Rod Placement
The primary objective of Stage 1 is to excise the scarred, non-functional tendon remnants, reconstruct the critical pulley system, and place a silicone rod to induce the formation of a biologically favorable pseudosheath.
Incision and Exposure:
The procedure commences with a volar Brunner (zigzag) incision extending from the distal phalanx to the distal palmar crease. This approach provides wide exposure while preventing longitudinal scar contracture across the flexion creases. A separate, secondary incision is made in the distal forearm or proximal palm to identify the proximal tendon stumps and to provide a gliding space for the proximal end of the silicone rod.
Adhesiolysis and Sheath Preparation:
Upon elevating the full-thickness skin flaps, the surgeon encounters the scarred flexor sheath. Dissection must proceed with extreme caution to identify and protect the digital neurovascular bundles, which are often encased in scar tissue and displaced from their normal anatomical positions.
The surgeon carefully incises the sheath to expose the scarred FDS and FDP tendons. To preserve the critical A2 and A4 pulleys while gaining access to the canal, L-shaped or window flaps can be created in the non-critical portions of the sheath (e.g., the cruciate pulleys or the A3 pulley).

The scarred FDS and FDP tendons are radically excised from the level of the distal phalanx to the palm. A small, 1-cm stump of the FDP is retained at its insertion on the distal phalanx to serve as a distal anchoring point for the silicone rod. The proximal stumps of the FDS and FDP are identified in the palm or forearm and tagged.
Pulley Reconstruction:
If the A2 or A4 pulleys are incompetent or destroyed, they must be reconstructed during Stage 1. Failure to do so will result in bowstringing of the rod and eventual failure of the graft. Pulley reconstruction can be performed using remnants of the excised FDS tendon, free tendon grafts (e.g., palmaris longus), or slips of the extensor retinaculum. The reconstructive tissue is woven around the proximal or middle phalanx (often deep to the extensor apparatus) and sutured to itself to create a robust, unyielding ring.

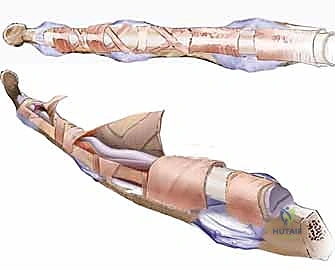
Silicone Rod Sizing and Insertion:
The surgeon selects a Hunter silicone rod (typically 3, 4, or 5 mm in diameter). The rod must glide smoothly within the reconstructed sheath without causing undue friction or buckling. A rod that is too large will cause necrosis of the overlying skin or pulleys; one that is too small will create an inadequate pseudosheath.

The rod is passed from distal to proximal through the preserved and reconstructed pulleys.
Distal and Proximal Fixation:
The distal end of the rod is secured to the preserved FDP stump using non-absorbable, monofilament sutures (e.g., 4-0 Prolene). Alternatively, it can be secured directly to the distal phalanx using a small suture anchor or through drill holes.

The proximal end of the rod is passed into the palm or distal forearm, depending on the planned site of the future proximal tendon weave. It is crucial that the proximal end of the rod is left free-gliding within the soft tissues. It must not be sutured to the proximal tendon stumps, as this would prevent the necessary passive excursion of the rod during postoperative rehabilitation. The surgeon must passively flex and extend the digit to ensure the rod glides smoothly without buckling or catching.

The incisions are closed meticulously, and the hand is placed in a dorsal blocking splint.
Stage 2: Tendon Grafting and Tensioning
Stage 2 is typically performed 3 to 6 months after Stage 1. The surgeon must ensure that the soft tissue envelope is completely healed, the digit is supple, and the patient has achieved full passive range of motion.
Incision and Graft Preparation:
Limited incisions are made: one distally over the DIP joint to access the distal end of the rod, and one proximally in the palm or forearm to access the proximal end. The previously selected donor tendon (e.g., palmaris longus) is harvested using standard techniques.
Graft Passage:
The proximal end of the silicone rod is identified. The distal end of the harvested tendon graft is firmly sutured to the proximal end of the rod. By applying gentle traction to the distal end of the rod at the DIP joint, the rod is slowly pulled out, simultaneously drawing the tendon graft through the newly formed, frictionless pseudosheath. This step must be performed smoothly to avoid disrupting the delicate mesothelial lining of the pseudosheath.
Distal Fixation:
Once the graft is fully passed, the distal end is secured to the distal phalanx. This can be achieved using the classic pull-out button technique (where sutures are passed through drill holes in the distal phalanx and tied over a button on the sterile nail matrix) or, more commonly in modern practice, utilizing a micro-suture anchor embedded directly into the volar base of the distal phalanx. The fixation must be absolutely rigid to withstand the forces of early active motion.
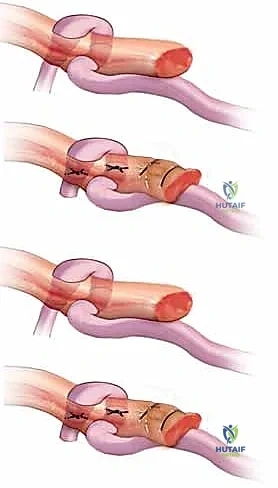
Proximal Weave and Tensioning:
The proximal end of the graft is now woven into the selected motor tendon (usually the proximal stump of the FDP or FDS of the affected digit, or an adjacent FDS if the native motor is irreparably contracted). The Pulvertaft weave is the biomechanical gold standard for this junction.
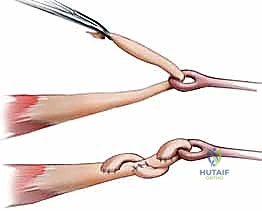
The graft is passed through multiple perpendicular slits in the motor tendon, creating a robust, interlacing mechanical bond.

Setting the correct tension is the most challenging and artistic aspect of the procedure. The surgeon must adjust the tension of the weave so that the reconstructed digit sits in a cascade slightly more flexed than its normal physiological resting posture. This slight over-tensioning anticipates the inevitable biological stretch that occurs as the graft heals and remodels. The surgeon must intraoperatively assess the tenodesis effect: wrist extension should produce full digital flexion, and wrist flexion should allow full digital extension. Once the ideal tension is achieved, the weave is secured with multiple non-absorbable mattress sutures (e.g., 3-0 or 4-0 braided polyester).
Complications, Incidence Rates, and Salvage Management
Staged flexor tendon reconstruction is fraught with potential pitfalls. The surgeon must be vigilant in identifying and managing complications to salvage functional outcomes.
| Complication | Estimated Incidence | Pathophysiology & Clinical Presentation | Salvage Management |
|---|---|---|---|
| Graft Rupture | 5% - 10% | Mechanical failure at the distal fixation or proximal weave, often due to aggressive early motion or non-compliance. Presents as sudden loss of active flexion. | Immediate surgical exploration and re-repair if the graft is viable. If the graft is destroyed, revision grafting or conversion to arthrodesis may be required. |
| Adhesion Formation | 15% - 30% | Fibroblastic proliferation tethering the graft to the pseudosheath, usually due to inadequate early motion or excessive bleeding. Presents as progressive loss of active, but not passive, motion. | Intensive hand therapy. If refractory after 4-6 months, a surgical tenolysis is indicated to free the graft, provided the tendon is intact. |
| Silicone Synovitis | 2% - 5% | Inflammatory response to the silicone rod during Stage 1. Presents as swelling, erythema, and pain along the flexor sheath, mimicking infection. | Oral anti-inflammatories and rest. If severe, premature removal of the rod and immediate Stage 2 grafting (if the bed is suitable) or abandonment of the procedure. |
| Bowstringing | 5% - 15% | Failure of the A2 or A4 pulleys (either native or reconstructed). Presents as visible tethering of the skin during flexion and profound loss of grip strength. | Surgical exploration and formal pulley reconstruction using tendon grafts or extensor retinaculum. |
| Infection | 1% - 3% | Bacterial inoculation of the surgical site. Catastrophic if it involves the pseudosheath. Presents as severe pain, purulence, and systemic signs. | Immediate aggressive surgical débridement, removal of the rod/graft, copious irrigation, and prolonged culture-directed intravenous antibiotics. |
| Joint Contracture | 10% - 20% | PIP joint flexion contracture due to prolonged immobilization or imbalance between flexor and extensor forces. | Aggressive dynamic splinting and therapy. Surgical capsulotomy is rarely successful if the underlying tendon mechanics are poor. |
The dichotomy between graft rupture and adhesion formation represents the fundamental tightrope walk of flexor tendon surgery. Aggressive rehabilitation risks rupture, while overly cautious immobilization guarantees adhesions. Silicone synovitis, while relatively rare with modern medical-grade elastomers, requires careful differentiation from acute bacterial infection; the latter demands immediate surgical exploration, while the former can often be managed conservatively.
Phased Post-
