Advanced Management of Talar Process Fractures and Talar Body Extrusions

Key Takeaway
Talar body extrusions and posterior process fractures represent severe, high-energy injuries requiring meticulous surgical management. Successful outcomes depend on prompt recognition, aggressive soft-tissue debridement, and anatomic restoration. This guide details the biomechanics, diagnostic imaging protocols, and step-by-step surgical interventions—ranging from fragment excision to complex tibiocalcaneal arthrodesis—essential for mitigating osteonecrosis and preserving hindfoot biomechanics.
Comprehensive Introduction and Patho-Epidemiology
The talus represents a unique biomechanical keystone within the lower extremity, functioning as the critical osseous link that transmits the entire weight of the human body from the tibial plafond to the complex articulations of the hindfoot and midfoot. Because approximately 60% of its surface area is enveloped by articular cartilage, the talus possesses a highly tenuous, retrograde extraosseous and intraosseous blood supply. This unforgiving anatomic reality makes the talus exceptionally vulnerable to ischemic complications, specifically osteonecrosis (avascular necrosis or AVN), following any significant traumatic insult. The management of talar trauma, therefore, requires a profound understanding of both its delicate vascularity and its complex spatial relationships within the ankle mortise and subtalar joint.
While isolated transchondral fractures of the talar dome are frequently encountered in sports medicine and are typically managed via arthroscopic debridement, microfracture, or osteochondral autograft transfer systems (OATS), high-energy trauma often results in far more devastating and mechanically destabilizing injuries. These include displaced fractures of the lateral and posterior talar processes, as well as the catastrophic, limb-threatening extrusion of the entire talar body. Process fractures are notoriously elusive on standard radiographic evaluations and are frequently misdiagnosed in the acute setting as severe ankle sprains. This diagnostic failure invariably leads to delayed presentations characterized by chronic hindfoot disability, severe subtalar arthrosis, and intractable pain.
The epidemiology of these injuries reflects distinct mechanisms of trauma. Lateral process fractures, historically termed "snowboarder's fractures," have seen a dramatic rise in incidence parallel to the popularity of the sport, occurring via a violent mechanism of axial loading combined with forced dorsiflexion and inversion. Conversely, posterior process fractures are frequently the result of forced plantarflexion or direct avulsion forces mediated by the posterior talofibular ligament (PTFL). Talar body extrusions (pan-talar extrusions) represent the extreme end of the trauma spectrum, almost exclusively resulting from high-velocity motor vehicle collisions, motorcycle accidents, or falls from significant heights. These are universally open, grossly contaminated injuries that present an immediate threat to limb salvage.
The primary overarching goal in the management of severe talar trauma—whether a displaced process fracture or a total extrusion—is the meticulous restoration of articular congruity, the preservation of hindfoot height, and the stabilization of the biomechanical axes of the foot. Even in the face of a high statistical risk of subsequent osteonecrosis, modern orthopedic traumatology dictates that anatomic reduction and rigid fixation offer the highest probability of functional salvage. The paradigm has shifted significantly over the past two decades from primary extirpative procedures (talectomy) toward aggressive joint preservation and reimplantation protocols.
Detailed Surgical Anatomy and Biomechanics
A masterful command of talar anatomy and its vascular supply is the absolute prerequisite for any surgeon undertaking the operative management of these injuries. The talus is anatomically divided into the head, neck, body, and two distinct processes (lateral and posterior). It is entirely devoid of muscular or tendinous origins or insertions, relying solely on capsuloligamentous structures for its stability and vascular inflow. The posterior process is bipartite, consisting of a lateral tubercle (which provides the attachment for the PTFL and may exist as an unfused os trigonum) and a medial tubercle. The fibro-osseous sulcus situated directly between these two tubercles serves as the conduit for the flexor hallucis longus (FHL) tendon. Fractures here directly compromise FHL excursion, leading to stenosing tenosynovitis or mechanical tethering.
The lateral process is a broad, wedge-shaped osseous prominence extending from the lateral aspect of the talar body. It forms a critical portion of the subtalar articulation, providing the articular surface for the posterior facet of the calcaneus inferiorly, while articulating with the distal fibula laterally. The lateral talocalcaneal ligament and the bifurcate ligament originate in this vicinity. Because the lateral process acts as a foundational pillar for the lateral column of the ankle, displaced fractures inherently destabilize both the ankle mortise and the subtalar joint, fundamentally altering the kinematics of hindfoot eversion and inversion.
The vascular anatomy of the talus is perhaps the most critical factor dictating surgical outcomes and complication rates. The blood supply is famously retrograde, forming an anastomotic sling around the talar neck before feeding the body. The primary contributor is the artery of the tarsal canal, a major branch of the posterior tibial artery, which supplies the majority of the talar body. This is supplemented by the artery of the sinus tarsi, formed by anastomoses between the perforating peroneal artery and the dorsalis pedis artery. Furthermore, delicate deltoid branches supply the medial aspect of the talar body. In high-energy trauma, particularly talar neck fractures and total extrusions, these extraosseous vessels are violently torn, and the intraosseous anastomoses are disrupted, virtually guaranteeing a period of profound ischemia to the talar body.
Biomechanically, the talus acts as a complex universal joint. During the normal gait cycle, it translates axial loads from the tibia into compressive and shear forces distributed across the calcaneus and the navicular. The subtalar joint, heavily reliant on the integrity of the lateral and posterior processes, functions as a multidirectional torque converter, translating the internal and external rotation of the tibia into pronation and supination of the foot. Disruption of this complex geometry by even 2 millimeters of articular step-off dramatically decreases the contact area of the subtalar joint, exponentially increasing peak contact stresses and rapidly accelerating the onset of post-traumatic arthrosis.
Exhaustive Indications and Contraindications
The decision-making algorithm for talar process fractures and extrusions requires a nuanced balancing of fracture morphology, patient physiology, and soft tissue integrity. Nonoperative management is strictly reserved for acute, truly non-displaced fractures of the lateral or posterior processes with intact articular congruity. However, the threshold for surgical intervention in the modern era is exceedingly low due to the catastrophic functional consequences of malunion or nonunion in the hindfoot.
For posterior and lateral process fractures, absolute indications for surgical intervention include any displacement greater than 2 millimeters, any demonstrable articular step-off involving the subtalar or tibiotalar joints, and the presence of large, comminuted fragments that block joint excursion. Furthermore, late presentations of missed posterior process fractures that have failed a 6-to-8-week trial of conservative immobilization and protected weight-bearing represent a strong indication for surgical excision of the nonunited fragment and meticulous neurolysis of the FHL tendon.
In the context of total talar body extrusion, the indications have evolved dramatically. Historically, primary talectomy with or without acute tibiocalcaneal arthrodesis was advocated to prevent the dreaded complications of deep infection and massive osteonecrosis. However, current evidence-based practice strongly mandates the reimplantation of the extruded talus as the primary standard of care. Reimplantation preserves the anatomic height of the ankle mortise, maintains limb length, and provides a structural scaffold for potential creeping substitution, even if avascular necrosis ensues.
Contraindications to surgical fixation or reimplantation must be carefully respected to avoid catastrophic septic complications. The primary absolute contraindication to reimplantation of an extruded talus is gross, unsalvageable contamination—such as that sustained in farmyard injuries involving soil or manure, or injuries with direct sewage exposure. Additionally, severe, non-reconstructable crushing or pulverization of the talar body where no structural integrity remains precludes reimplantation. In these scenarios, a staged "damage control" orthopedic protocol utilizing antibiotic spacers is indicated.
| Injury Type | Primary Indications for Surgery | Contraindications for Primary Fixation/Reimplantation |
|---|---|---|
| Posterior Process Fracture | Displacement >2mm; Subtalar incongruity; FHL tethering; Failed conservative tx (>6 weeks). | Truly non-displaced fractures; Severe peripheral vascular disease precluding wound healing. |
| Lateral Process Fracture | Displacement >2mm; Subtalar joint step-off; Large comminuted fragments blocking eversion. | Non-displaced fractures; Active local soft tissue infection (cellulitis). |
| Talar Body Extrusion | Open extrusion with salvageable bone; Ability to achieve adequate soft tissue coverage. | Gross contamination (farm/sewage); Pulverized bone; Unsalvageable ischemic limb. |
| Missing/Unsalvageable Talus | Acute stabilization required; Dead space management needed. | Primary internal hardware or allograft placement in the acute, contaminated setting. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful outcomes in complex talar trauma. Standard anteroposterior (AP), lateral, and mortise radiographs of the ankle are mandatory but are notoriously inadequate for defining the true spatial geometry of process fractures due to the dense osseous overlap of the medial and lateral malleoli, the calcaneus, and the midfoot. A lateral radiograph of the contralateral, uninjured foot is highly recommended for comparison, particularly to differentiate an acute avulsion fracture of the lateral tubercle from a bipartite, well-corticated os trigonum.

Preoperative lateral radiograph demonstrating a suspicious osseous density posterior to the talus, often difficult to distinguish from an os trigonum without advanced imaging.
Computed Tomography (CT) is the absolute gold standard for preoperative diagnosis and surgical templating. Thin-slice (1mm) axial, coronal, and sagittal reconstructions are essential. Coronal CT images are particularly critical for evaluating the degree of displacement, comminution, and subtalar joint involvement in lateral process fractures. Sagittal reconstructions provide unparalleled visualization of the posterior process, the FHL sulcus, and the posterior facet of the subtalar joint.

Preoperative sagittal CT scan clearly delineating a large, displaced posterior process fracture with intra-articular extension into the subtalar joint.
Surgical templating involves selecting the appropriate fixation modalities. For process fractures, mini-fragment sets utilizing 2.0 mm, 2.4 mm, or 2.7 mm cortical lag screws are required. Headless compression screws are frequently utilized to allow for subchondral burial of the hardware, preventing impingement during joint articulation. For talar extrusions, external fixation components (spanning delta-frames) and heavy Steinmann pins (typically 4.0 mm to 5.0 mm) must be available to achieve acute stabilization of the reimplanted, highly unstable talus.
Patient positioning is dictated by the specific surgical approach required. For posterior process fractures, the patient is typically positioned prone on a radiolucent Jackson table. This allows for direct, unimpeded access to the posterolateral or posteromedial ankle. A thigh tourniquet is applied, and the foot is allowed to hang freely off a bump to facilitate intraoperative fluoroscopy. For lateral process fractures, the patient is positioned supine with a substantial bump placed under the ipsilateral hip. This internally rotates the lower extremity, bringing the lateral malleolus and the lateral hindfoot into a direct vertical trajectory for the surgeon. For talar extrusions, a supine position is standard, often requiring a radiolucent triangle to elevate the leg for simultaneous anterior, medial, and lateral access during the aggressive debridement and reimplantation process.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution for talar trauma demands meticulous soft tissue handling to preserve whatever tenuous blood supply remains. For posterior process fractures, the decision between Open Reduction and Internal Fixation (ORIF) versus fragment excision depends on the size of the fragment and the chronicity of the injury. Acute, large fragments involving the subtalar joint warrant ORIF, while late presentations or small, comminuted fragments are best treated with sharp excision.
When excising a lateral tubercle fracture, a posterolateral approach is utilized. A longitudinal incision is made midway between the lateral border of the Achilles tendon and the posterior border of the fibula. The lesser saphenous vein and the sural nerve are carefully identified and retracted laterally. The deep fascia is incised, and the surgeon develops the internervous plane between the peroneal tendons (lateral) and the FHL tendon (medial). The fractured fragment is identified within the posterior capsule. Meticulous dissection is required to free the FHL tendon from the osseous fragment to prevent postoperative tethering. The fragment is sharply excised, the joint is irrigated, and the retinaculum is repaired.

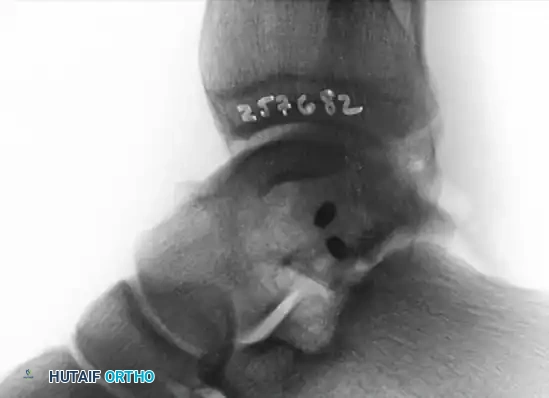
Postoperative lateral radiograph following successful excision of the posterior process fragment. The patient subsequently became asymptomatic with full restoration of FHL excursion.
For lateral process fractures, an anterolateral approach provides optimal exposure. The incision begins 2 centimeters proximal to the ankle joint line, just anterior to the fibula, and extends distally toward the base of the fourth metatarsal. The superficial peroneal nerve (SPN) branches must be identified and protected in the subcutaneous tissue. The inferior extensor retinaculum is incised, and the extensor digitorum brevis (EDB) muscle belly is mobilized inferiorly. The fracture hematoma is evacuated from the lateral gutter and the subtalar joint.
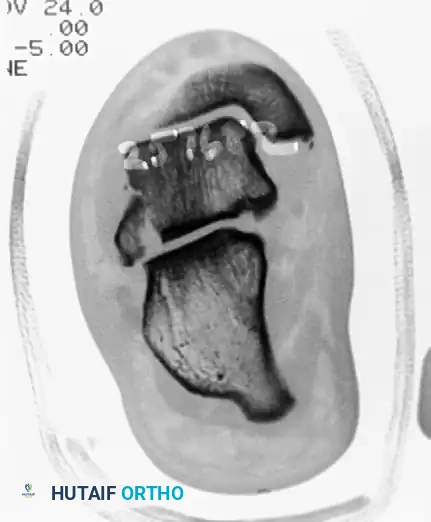
Preoperative coronal CT scan demonstrating a significantly displaced lateral process fracture of the talus, disrupting the subtalar articulation.
Anatomic reduction is achieved using a dental pick or small point-to-point reduction forceps, taking great care not to crush the fragile cancellous bone. Stabilization is achieved using two 2.0 mm or 2.4 mm cortical lag screws directed from lateral to medial, compressing the fragment into the talar body. It is absolutely critical that the screw heads are fully countersunk beneath the articular cartilage or utilizing headless compression screws to prevent catastrophic impingement against the lateral malleolus during eversion.
Postoperative Anteroposterior (AP) radiograph showing anatomic reduction and stabilization of the lateral process.
Postoperative lateral radiograph confirming the placement of fully countersunk screws, ensuring no intra-articular hardware prominence.
In the catastrophic event of a talar body extrusion, the surgical technique shifts to a damage-control and salvage paradigm. The extruded talus is taken to the back table and subjected to high-volume pulsatile lavage (typically 9 liters of normal saline) and soaked in a broad-spectrum antibiotic solution (e.g., Vancomycin and Tobramycin). Simultaneously, the open ankle wound undergoes aggressive surgical debridement of all necrotic soft tissue and foreign debris. The talus is carefully reinserted into the ankle mortise, ensuring precise anatomic orientation. Because the reimplanted talus is entirely devoid of ligamentous stability, rigid fixation is mandatory. This is achieved via a spanning external fixator or heavy transfixion Steinmann pins driven from the plantar aspect of the calcaneus, through the reimplanted talus, and into the distal tibia. Immediate soft tissue coverage, frequently necessitating collaboration with plastic surgery for free tissue transfer (e.g., anterolateral thigh flap), is mandatory to prevent desiccation of the avascular bone.
In scenarios where the talus is missing or unsalvageable, a staged Masquelet-type protocol is employed. Stage 1 involves aggressive irrigation and debridement followed by the placement of a polymethylmethacrylate (PMMA) antibiotic-impregnated spacer molded to mimic the talar body. A spanning external fixator maintains limb length. At 2 to 3 weeks, if cultures remain negative, Stage 2 involves removal of the PMMA spacer and definitive tibiocalcaneal arthrodesis. A structural femoral head allograft is contoured to fill the void, restoring hindfoot height, and rigid internal fixation is achieved using a retrograde intramedullary tibiotalocalcaneal (TTC) nail.
Complications, Incidence Rates, and Salvage Management
The management of severe talar trauma is fraught with high rates of debilitating complications, necessitating extensive preoperative counseling and meticulous postoperative surveillance. The most feared and prevalent complication is osteonecrosis (AVN) of the talar body. Because total extrusions completely sever the retrograde blood supply, AVN is an expected physiologic consequence rather than an avoidable complication. The incidence of partial or total AVN following talar extrusion ranges from 54% to 83%, with rates approaching 100% if the extruded talus is concurrently fractured or crushed.
Surgeons must monitor for the "Hawkins sign" on serial AP or mortise radiographs at 6 to 8 weeks post-injury. The Hawkins sign manifests as a subchondral radiolucent band in the talar dome, indicating that the bone is hyperemic, revascularization is occurring, and the talus is viable. The absence of this lucency, coupled with relative sclerosis of the talar body compared to the osteopenic surrounding bone, is highly predictive of AVN. If AVN develops, the talus may undergo creeping substitution—a prolonged process where osteoclasts resorb dead bone while osteoblasts lay down new woven bone. During this phase, the talus is structurally compromised and highly susceptible to mechanical collapse.
Infection is another catastrophic complication, particularly given that extrusions are high-energy open injuries. Historically, deep infection rates following reimplantation approached 50%, leading to early recommendations for primary talectomy. However, modern aggressive debridement protocols, immediate administration of systemic antibiotics, and the utilization of local antibiotic-impregnated spacers or bead pouches have dramatically reduced infection rates to 0% to 10% in specialized tertiary trauma centers. If a deep, recalcitrant infection occurs, hardware removal, aggressive debridement, and conversion to a septic nonunion protocol with an external fixator (e.g., Ilizarov or Calandruccio frame) is mandatory.
Post-traumatic arthritis of the subtalar and tibiotalar joints is nearly ubiquitous following displaced process fractures and extrusions, regardless of the quality of the initial anatomic reduction. The initial chondral impact, combined with altered joint kinematics and potential avascular collapse, leads to progressive joint space narrowing, subchondral cyst formation, and debilitating pain. Salvage management for end-stage post-traumatic arthritis or painful talar collapse involves definitive arthrodesis. Depending on the extent of the pathology, this may require an isolated subtalar fusion, a tibiotalar fusion, or a comprehensive tibiotalocalcaneal (TTC) arthrodesis utilizing a retrograde intramedullary nail or rigid locking plates.
| Complication | Estimated Incidence | Pathophysiology / Risk Factors | Salvage Management |
|---|---|---|---|
| Osteonecrosis (AVN) | 54% - 83% (Extrusions) | Disruption of artery of tarsal canal/sinus tarsi; Concurrent talar neck/body fractures. | Protected weight-bearing (PTB brace); Core decompression; TTC Arthrodesis for collapse. |
| Deep Infection | 0% - 10% (Modern protocols) | Open fractures; Gross contamination; Inadequate initial debridement; Poor soft tissue envelope. | Serial I&D; Hardware removal; Antibiotic spacers; External fixation; Amputation (extreme cases). |
| Post-Traumatic Arthritis | >60% (Long-term) | Initial chondral injury; Articular step-off >2mm; Altered hindfoot kinematics. | Activity modification; Intra-articular injections; Subtalar or Tibiotalar Arthrodesis. |
| FHL Tethering / Tenosynovitis | 15% - 25% (Posterior Process) | Fibrosis within the FHL sulcus; Malunion of the medial/lateral tubercles. | Surgical exploration; FHL neurolysis/tenolysis; Excision of malunited fragments. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following the surgical management of talar process fractures and extrusions is a prolonged, demanding process that requires strict patient compliance and close coordination with specialized physical therapists. The overarching philosophy of the rehabilitation protocol is to protect the precarious osseous fixation and the fragile vascular status of the talus while preventing the devastating stiffness that commonly afflicts the hindfoot following prolonged immobilization.
For isolated posterior and lateral process fractures that have undergone ORIF or excision, Phase 1 (0 to 4 weeks) involves strict non-weight-bearing (NWB) status. The patient is placed in a well-padded, short-leg splint in neutral dorsiflexion to minimize tension on the posterior capsule and the FHL tendon. At 2 weeks, sutures are removed, and the patient is transitioned to a controlled ankle motion (CAM) boot. Phase 2 (4 to 8 weeks) initiates progressive weight-bearing, contingent upon radiographic evidence of early callus formation and the absence of hardware failure. Active, non-weight-bearing range of motion (ROM) exercises of the ankle and subtalar joints are initiated out of the boot to prevent capsular contracture. Phase 3 (8 to 12 weeks) involves full weight-bearing, aggressive proprioceptive training, and strengthening of the peroneal and posterior tibial musculature.
The rehabilitation protocol for a reimplanted talar body extrusion is drastically more conservative due to the profound risk of avascular necrosis and structural collapse. Phase 1 (0 to 12 weeks) mandates absolute, strict non-weight-bearing status. The limb is immobilized either in a spanning external fixator or a rigid cast. Serial radiographs are obtained at 4, 8, and 12 weeks to monitor for the critical development of the Hawkins sign. The soft tissue envelope, particularly if managed with a free flap, is meticulously monitored by the plastic surgery team.
If at 12 weeks the talus demonstrates radiographic evidence of AVN (increased radiodensity without a Hawkins sign), Phase 2 management shifts to protecting the talus during the prolonged phase of creeping substitution, which can take up to 24 to 36 months. To prevent mechanical deformation and collapse of the avascular talar dome, the patient is fitted with a custom patellar tendon-bearing (PTB) orthosis. This specialized brace unloads the ankle joint by transferring axial loads directly from the proximal tibia to the ground. The patient remains in the PTB brace during all weight-bearing activities until serial imaging (often requiring MRI or CT) confirms structural revascularization and the resolution of the necrotic segment.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical decision-making in severe talar trauma is deeply rooted in several landmark orthopedic studies that have fundamentally shifted the standard of care. Historically, the management of talar extrusions was guided by an overwhelming fear of overwhelming sepsis and gas gangrene. Early 20th-century literature universally advocated for the immediate extirpation of the extruded talus (primary talectomy) and a delayed tibiocalcaneal fusion. However, the functional results of primary talectomy were universally poor, leaving patients with a foreshortened, mechanically inefficient limb and severe gait abnormalities.
A paradigm shift occurred in the late 1990s and early 2000s, driven by advancements in high-energy trauma management, modern antibiotic protocols, and sophisticated soft tissue reconstruction techniques. Landmark retrospective reviews from major Level 1 trauma centers demonstrated that reimplantation of the extruded talus, when combined with aggressive, high-volume pulsatile lavage and immediate broad-spectrum antibiotics, resulted in deep infection rates comparable to other high-energy open fractures (under 10%). These studies established the modern clinical guideline that an extruded talus should almost always be reimplanted, acting at the very least as an anatomic, biologic spacer that preserves limb length and the geometry of the ankle mortise, even if a secondary fusion is ultimately required.
Regarding process fractures, the seminal work by Hawkins in the 1970s, originally describing the classification and vascular implications of talar neck fractures, laid the foundation for understanding the retrograde blood supply of the entire talus. Later literature specifically addressing lateral process fractures (the "snowboarder's fracture") highlighted the unacceptably high rates of missed diagnoses in emergency departments. Modern clinical guidelines now firmly dictate that any patient presenting with persistent lateral ankle pain and swelling beyond 4 weeks, with a mechanism of axial load and inversion, must undergo a thin-slice CT scan to definitively rule out a displaced lateral process fracture.
In summary, the contemporary literature demands a high index of suspicion, aggressive utilization of advanced cross-sectional imaging, and meticulous, joint-preserving surgical techniques. The definitive goal remains the anatomic restoration of the talar keystone, prioritizing the preservation of hindfoot biomechanics and mitigating the severe long-term morbidity associated with these devastating injuries.
