Subtalar Dislocations: Comprehensive Surgical Management

Key Takeaway
Subtalar dislocations, or peritalar dislocations, involve the simultaneous dislocation of the distal articulations of the talus at the talocalcaneal and talonavicular joints. Medial dislocations are most common and often reducible closed. Lateral dislocations frequently require open reduction due to soft tissue interposition, typically the posterior tibial tendon. Post-reduction computed tomography is mandatory to identify occult osteochondral fractures or intra-articular debris that may necessitate surgical debridement or internal fixation to prevent post-traumatic arthrosis.
Comprehensive Introduction and Patho-Epidemiology
Subtalar dislocations, historically and perhaps more accurately referred to as peritalar dislocations, represent a severe, complex, and relatively uncommon disruption of the hindfoot architecture. In this specific injury pattern, the normal anatomic relationships of the talocalcaneal and talonavicular joints are simultaneously obliterated, while the tibiotalar (ankle) and calcaneocuboid joints typically remain congruous and intact. Consequently, the calcaneus, cuboid, navicular, and the entire forefoot become displaced as a single functional unit from the inferior and distal aspects of the talus. This creates a profound biomechanical dissociation between the talus—which remains locked within the ankle mortise—and the remainder of the pedal skeleton.
Epidemiologically, these injuries are relatively rare, accounting for approximately 1% to 2% of all traumatic joint dislocations. They are most frequently the result of high-energy trauma, such as motor vehicle collisions, motorcycle accidents, or falls from a significant height. However, they can also occur in lower-energy, high-torque athletic scenarios, classically described in the literature as "basketball foot" due to the forceful landing on an inverted, plantarflexed foot. Young, active males in their second to fourth decades of life comprise the vast majority of the patient demographic. Because of the immense kinetic forces required to disrupt the robust ligamentous restraints of the peritalar complex, subtalar dislocations are frequently associated with severe soft tissue compromise, osteochondral shear fractures, and substantial long-term morbidity.
The pathoanatomy of subtalar dislocations is intrinsically linked to the direction of the deforming force, which dictates the classification of the injury. Medial dislocations are by far the most ubiquitous, accounting for approximately 65% to 80% of all subtalar dislocations. This pattern typically results from a forced inversion of a plantarflexed foot, driving the talus laterally while the calcaneus and navicular displace medially. Clinically, the foot assumes an "acquired clubfoot" deformity, with the head of the talus becoming highly prominent dorsolaterally. The skin overlying this prominence is often subjected to extreme tension, placing it at an immediate and critical risk for ischemic necrosis if reduction is delayed.
Conversely, lateral dislocations account for 15% to 35% of cases and are generally associated with significantly higher-energy trauma. The mechanism involves forced eversion of a dorsiflexed foot, driving the talus medially while the foot complex translates laterally. This results in an "acquired flatfoot" clinical appearance, with the talar head prominent medially. Anterior and posterior dislocations are exceedingly rare (comprising less than 5% of cases combined) and usually result from extreme, direct high-energy crushing forces. Regardless of the direction, the disruption of the peritalar joints obligates a catastrophic failure of the interconnecting capsuloligamentous structures, necessitating a profound understanding of hindfoot anatomy for successful surgical management.
Detailed Surgical Anatomy and Biomechanics
A masterful comprehension of the peritalar anatomy is an absolute prerequisite for the orthopedic surgeon managing subtalar dislocations. The subtalar joint (talocalcaneal joint) is a complex, multi-faceted articulation divided into an anterior, middle, and posterior facet. The posterior facet is the largest, bearing the majority of the axial load, and is separated from the anterior and middle facets by the tarsal canal and the sinus tarsi. The talonavicular joint, functioning in concert with the subtalar joint, forms the "acetabulum pedis" or coxa pedis—a highly constrained socket formed by the navicular, the anterior and middle facets of the calcaneus, and the spring ligament complex, which articulates with the spherical talar head.
The stability of the peritalar complex is heavily reliant on a robust network of intrinsic and extrinsic ligaments. The primary intrinsic stabilizers are the talocalcaneal interosseous ligament (TCIL) and the cervical ligament, both residing within the sinus tarsi. The TCIL is a dense, broad structure that acts as the primary restraint to excessive supination, while the cervical ligament resists excessive inversion. During a subtalar dislocation, both of these critical intrinsic ligaments are inevitably ruptured. Extrinsic stability is provided by the calcaneofibular ligament (CFL) laterally and the tibiocalcaneal portion of the deltoid ligament medially. The extensor retinaculum and the bifurcate ligament also contribute to regional stability. The obligatory rupture of these structures during dislocation leads to the profound instability observed post-reduction.
The vascular anatomy of the hindfoot is of paramount clinical importance, particularly regarding the blood supply to the talus. The talus receives its perfusion via a retrograde retrograde anastomotic sling derived from the three major vessels of the leg: the posterior tibial, anterior tibial, and peroneal arteries. The artery of the tarsal canal (a branch of the posterior tibial artery) and the artery of the sinus tarsi (formed by anastomoses from the perforating peroneal and anterior tibial arteries) supply the majority of the talar body. During a subtalar dislocation, the violent displacement tears the capsular and ligamentous attachments, frequently disrupting these delicate intraosseous and extraosseous anastomoses. This vascular insult is the primary pathophysiological driver for the development of post-traumatic avascular necrosis (AVN) of the talus, a devastating complication.
Biomechanically, the subtalar joint acts as a complex torque transmitter, converting the transverse plane rotation of the tibia into sagittal and coronal plane movements of the foot (inversion and eversion). The axis of the subtalar joint is obliquely oriented, passing from posterolateral-inferior to anteromedial-superior. Because the talocalcaneal and talonavicular joints function as an obligate coupled mechanism, the disruption of this complex drastically alters hindfoot kinematics. Even after a perfectly congruent reduction, the dense fibrotic healing of the ruptured interosseous and cervical ligaments routinely results in a permanent reduction in subtalar excursion. Understanding this biomechanical reality is crucial for managing patient expectations regarding long-term functional outcomes and navigating uneven terrain.
Exhaustive Indications and Contraindications
The management of subtalar dislocations demands rapid clinical decision-making. While the initial approach to a closed injury is almost universally an attempt at emergent closed reduction under conscious sedation in the emergency department, numerous clinical scenarios necessitate urgent or emergent operative intervention. The decision to proceed to the operating room must be predicated on a thorough assessment of soft tissue viability, the presence of associated fractures, and the reducibility of the joint complex. Repeated, forceful attempts at closed reduction are strictly contraindicated, as they exacerbate soft tissue trauma, increase the risk of iatrogenic osteochondral shearing, and elevate the risk of acute compartment syndrome.
The indications for surgical management are broadly categorized into emergent open reduction for irreducible or open dislocations, and delayed definitive management for associated intra-articular fractures identified on post-reduction computed tomography (CT). Irreducibility is most commonly encountered in lateral dislocations, where the posterior tibial tendon, the extensor digitorum brevis muscle belly, or the joint capsule becomes incarcerated within the talonavicular or subtalar joint spaces. In medial dislocations, the extensor retinaculum or the deep peroneal neurovascular bundle may block reduction. Open injuries require emergent formal surgical debridement, copious irrigation, and open reduction to mitigate the extraordinarily high risk of deep space infection and osteomyelitis.
Relative indications for surgical intervention include the presence of osteochondral shear fractures of the talar dome, talar head, or subtalar articular facets. As emphasized by DeLee and Curtis, the retention of intra-articular osteochondral debris or the failure to anatomically reduce articular step-offs significantly accelerates the onset of post-traumatic degenerative arthritis. Furthermore, fractures of the lateral process of the talus (the "snowboarder's fracture") or impaction fractures of the navicular frequently accompany subtalar dislocations and may require open reduction and internal fixation (ORIF) to restore joint congruity and stability.
Contraindications to immediate open reduction and internal fixation are primarily related to severe host factors or catastrophic soft tissue envelopes. In cases of profound soft tissue crushing injuries, extensive blistering, or gross contamination in an unstable polytrauma patient, definitive internal fixation should be delayed. In these extreme scenarios, the joint should be reduced (open or closed), aggressively debrided if open, and stabilized with a spanning external fixator or stout transarticular Steinmann pins to maintain alignment while the soft tissue envelope is resuscitated.
Table: Indications and Contraindications for Operative Management
| Category | Indications for Operative Management (Open Reduction / ORIF) | Contraindications to Immediate Definitive ORIF |
|---|---|---|
| Emergent / Urgent | Irreducible dislocation after 1-2 closed attempts | Unstable polytrauma patient (Damage Control Orthopedics required) |
| Open subtalar dislocation (Requires immediate I&D) | Grossly contaminated wounds precluding safe internal hardware placement | |
| Impending skin necrosis (tented skin) failing closed reduction | ||
| Acute compartment syndrome of the foot or leg | ||
| Subacute / Definitive | Displaced osteochondral shear fractures of the talus/calcaneus | Severe, unresuscitated soft tissue envelope (fracture blisters, extreme edema) |
| Intra-articular debris blocking congruent joint reduction | Non-ambulatory patient with minimal functional demands (relative) | |
| Associated displaced fractures (lateral process talus, navicular) | Active local infection or severe peripheral vascular disease | |
| Gross instability requiring transarticular pinning |
Pre-Operative Planning, Templating, and Patient Positioning
The pre-operative phase begins with a meticulous initial assessment following Advanced Trauma Life Support (ATLS) protocols, as these injuries frequently occur in the context of polytrauma. Once life-threatening injuries are addressed, attention is directed to the injured extremity. Patients present with gross deformity, severe pain, and profound swelling. A rigorous neurovascular examination is paramount and must be documented prior to any manipulation. The posterior tibial artery and nerve are particularly vulnerable to traction injuries in lateral dislocations, while the superficial peroneal nerve and dorsalis pedis artery are at high risk in medial dislocations. Tented, blanched skin over the prominent talar head represents a true orthopedic emergency; failure to reduce the dislocation expeditiously will result in full-thickness skin necrosis, converting a closed injury into a complex open joint.
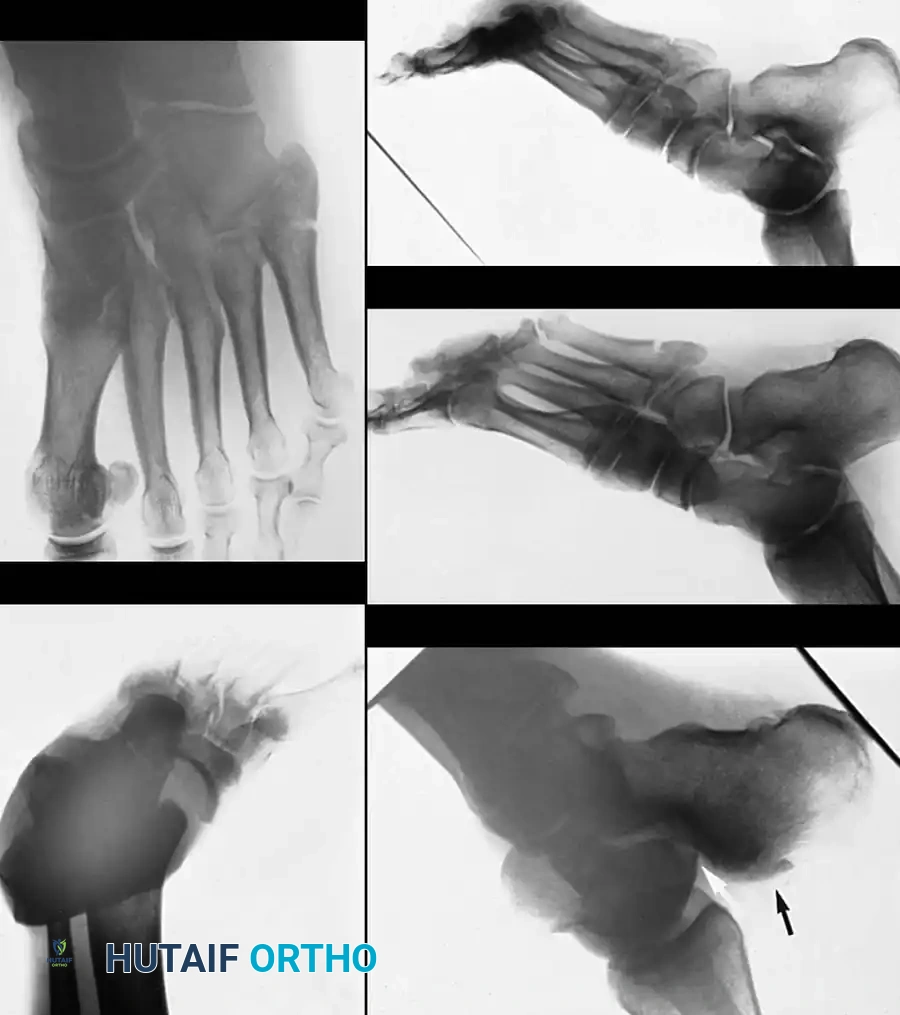
Radiographic evaluation begins with standard trauma radiographs of the foot and ankle, including Anteroposterior (AP), Lateral, and Mortise views. The AP view typically demonstrates the talonavicular dislocation, while the lateral view highlights the talocalcaneal dissociation and the loss of the normal talocalcaneal angle. However, plain radiographs are notoriously inadequate for identifying the full spectrum of pathoanatomy. As definitively established by Bibbo et al., obtaining a post-reduction computed tomography (CT) scan is an absolute necessity. CT imaging with 1mm fine cuts and multiplanar reconstructions frequently reveals occult osteochondral shear fractures, lateral process fractures, navicular impaction injuries, and intra-articular debris that plain films obscure. The findings on this post-reduction CT scan dictate the definitive surgical plan.
Pre-operative templating involves reviewing the CT scan to identify the exact location of any offending osteochondral fragments or osseous blocks to reduction. If internal fixation is anticipated for associated fractures, the surgeon must ensure the availability of headless compression screws, mini-fragment plates, and bioabsorbable pins. For purely ligamentous but highly unstable injuries, stout Steinmann pins or Kirschner wires (K-wires) must be available for transarticular stabilization. The surgical team must also be prepared with a spanning external fixator construct in the event that the soft tissue envelope precludes internal fixation or primary closure.
Patient positioning is critical for optimal surgical access and intraoperative fluoroscopy. The patient is placed supine on a radiolucent operating table. A well-padded bump is placed under the ipsilateral hip to internally rotate the leg, bringing the foot into a neutral position and allowing unhindered access to the lateral aspect of the hindfoot. A well-padded thigh tourniquet is applied to ensure a bloodless surgical field, which is essential for identifying small intra-articular fragments and protecting delicate neurovascular structures. The C-arm fluoroscopy unit must be positioned to easily obtain true AP, lateral, and oblique views of the hindfoot and midfoot without compromising the sterile field. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation.
Step-by-Step Surgical Approach and Fixation Technique
When closed reduction fails, or when advanced imaging reveals intra-articular fragments blocking congruent reduction, open reduction is strictly indicated. The surgical approach must be tailored to the direction of the dislocation and the suspected anatomic block. For the majority of cases, an anterolateral approach provides unparalleled access to the subtalar and talonavicular joints. However, the surgeon must be prepared to utilize a dual-incision technique if the primary approach fails to clear the incarcerated structures.
The Anterolateral Approach
The procedure begins with a longitudinal anterolateral incision, approximately 7.5 to 10 cm in length, originating just proximal to the tibiotalar joint line and extending distally toward the base of the fourth metatarsal, passing directly over the sinus tarsi and the cuboid. Meticulous superficial dissection is required to identify and protect the medial and lateral dorsal cutaneous branches of the superficial peroneal nerve, which frequently traverse the operative field and are highly susceptible to iatrogenic neuroma formation.
The deep dissection exploits the internervous plane between the extensor digitorum longus (EDL) and extensor hallucis longus (EHL) tendons medially, and the peroneus tertius tendon laterally. The extensor digitorum brevis (EDB) muscle belly is identified and elevated from its origin on the lateral calcaneus and reflected distally. This exposes the lateral aspect of the talar neck, the sinus tarsi, the anterior and posterior facets of the subtalar joint, and the calcaneocuboid articulation. A formal capsulotomy is performed over the head and neck of the talus, extending distally into the midtarsus to fully visualize the talonavicular joint. Copious irrigation is utilized to evacuate the fracture hematoma and flush out small, loose osteochondral debris.
Reduction Maneuvers and Addressing Blocks
With the joints exposed, direct visualization allows the surgeon to identify the impediment to reduction. In medial dislocations, the capsule of the talonavicular joint or the EDB muscle may be interposed. A robust periosteal elevator or a bone skid is inserted into the subtalar joint. Utilizing careful leverage combined with longitudinal traction applied by an assistant, the locked articular surfaces are disengaged. For a medial dislocation, the assistant simultaneously abducts and everts the foot while applying axial traction.
If dealing with an irreducible lateral dislocation, the anterolateral approach alone is frequently insufficient because the posterior tibial tendon is typically entrapped within the talonavicular joint, effectively lassoing the talar neck. In this scenario, a secondary medial incision is mandated. A longitudinal incision is made centered over the prominent talonavicular joint. The dorsal neurovascular bundle is carefully protected. The incarcerated posterior tibial tendon is identified, manually extracted from the joint space using a blunt hook, and retracted medially. Once this soft tissue block is removed, the navicular can be smoothly levered around the head of the talus, achieving an anatomic reduction of the coxa pedis.
Assessment of Stability and Fixation Strategy
Following successful reduction, the stability of the subtalar and talonavicular joints is rigorously assessed under live fluoroscopy. If the reduction is stable through a functional range of motion, no internal fixation is required. However, due to the catastrophic disruption of the interosseous, cervical, and capsular ligaments, the complex is frequently highly unstable. In such cases, the reduction must be maintained with temporary transarticular fixation.
Stout Steinmann pins (typically 2.0 mm to 2.8 mm) or heavy K-wires are driven percutaneously or under direct visualization. A common construct involves passing one pin from the navicular into the talar head and neck, and a second pin from the calcaneus dorsally into the talus, effectively neutralizing the peritalar complex. It is imperative to verify on multiple fluoroscopic views that the pins do not inadvertently violate the intact tibiotalar (ankle) joint. Any associated osteochondral shear fractures of the talus or calcaneus that are large enough to accept fixation are stabilized with headless compression screws or bioabsorbable darts. The wounds are then copiously irrigated, the extensor retinaculum is repaired to prevent tendon bowstringing, and a meticulous, tension-free layered closure is performed.
Complications, Incidence Rates, and Salvage Management
The immense kinetic energy required to produce a subtalar dislocation ensures that complications are frequent, even following prompt and anatomic reduction. The surgeon must proactively counsel the patient regarding these expected sequelae. The most devastating early complication is skin necrosis resulting from delayed reduction of a tented soft tissue envelope. Full-thickness skin loss exposes the underlying articular cartilage and bone, necessitating complex soft tissue reconstruction (e.g., free tissue transfer or rotational flaps) and exponentially increasing the risk of deep infection and osteomyelitis.
Avascular necrosis (AVN) of the talus is a profound late complication, directly correlated with the severity of the initial trauma and the degree of vascular disruption. While less common in pure subtalar dislocations compared to talar neck fractures, AVN still occurs in up to 10-20% of high-energy or open dislocations. The disruption of the artery of the tarsal canal and the intraosseous anastomoses leads to ischemia of the talar body. Radiographic evidence of AVN typically manifests between 6 to 12 weeks post-injury as increased radiodensity of the talar dome relative to the surrounding osteopenic bone (a negative Hawkins sign). If AVN progresses to structural collapse of the talar dome, severe tibiotalar and subtalar arthrosis is inevitable.
Post-traumatic osteoarthritis is the most ubiquitous long-term complication, affecting the subtalar and talonavicular joints. This degenerative process is driven by initial chondral impaction damage, retained osteochondral debris, and altered joint kinematics secondary to ligamentous scarring. Bibbo et al. demonstrated that radiographically, up to 89% of patients show subtalar joint abnormalities at long-term follow-up, with 63% being clinically symptomatic. Patients frequently report chronic pain, stiffness, and extreme difficulty ambulating on uneven surfaces.
Salvage management for end-stage post-traumatic arthritis or painful AVN typically involves arthrodesis. An isolated subtalar arthrodesis (in situ or with structural bone graft to restore calcaneal height) is the workhorse procedure for isolated subtalar arthritis. However, if the talonavicular joint is also severely degenerated, a formal triple arthrodesis (fusion of the subtalar, talonavicular, and calcaneocuboid joints) is required to eliminate pain and provide a stable, plantigrade foot. In catastrophic cases of total talar collapse or intractable deep infection, a talectomy combined with a tibiocalcaneal arthrodesis may be the only viable limb salvage option.
Table: Complications and Salvage Strategies
| Complication | Estimated Incidence | Pathophysiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Post-Traumatic Arthritis | 60% - 85% | Chondral shear, altered kinematics, retained debris | NSAIDs, bracing, Subtalar or Triple Arthrodesis |
| Subtalar Stiffness | > 90% | Dense fibrotic healing of peritalar ligaments | Aggressive physical therapy, permanent modification of activities |
| Avascular Necrosis (AVN) | 10% - 20% | Disruption of tarsal canal / sinus tarsi blood supply | Protected weight-bearing, core decompression, Hindfoot Arthrodesis |
| Skin Necrosis / Infection | 5% - 15% (Higher in Open) | Prolonged skin tenting, high-energy open trauma | Serial debridement, negative pressure wound therapy, flap coverage |
| Chronic Instability | < 5% | Inadequate immobilization period (< 4-6 weeks) | Ankle-foot orthosis (AFO), ligamentous reconstruction (rare) |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a subtalar dislocation requires a highly structured, phased approach that delicately balances the absolute necessity of protecting the healing peritalar capsuloligamentous structures with the critical need to prevent profound, permanent hindfoot stiffness. The protocol is heavily influenced by the presence of associated fractures, the stability of the reduction, and whether transarticular pinning was required.
Phase I: Immediate Postoperative Period (0 to 6 Weeks)
Immediately following surgery, the extremity is placed in a bulky, well-padded short-leg cast or a rigid posterior splint extending from the base of the toes to the tibial tuberosity. Swelling management is the paramount concern during the first 72 hours. If a circumferential cast is applied in the operating room, it must be bivalved immediately in the recovery room to accommodate the anticipated severe postoperative edema and to mitigate the risk of acute compartment syndrome. The limb is strictly elevated above the level of the heart.
During this phase, the patient is maintained on a strict non-weight-bearing status on the operative extremity. Crutches, a walker, or a knee scooter are utilized for mobility. While the hindfoot is immobilized, active range of motion exercises of the metatarsophalangeal (MTP) joints and the knee are encouraged immediately to prevent forefoot stiffness, maintain muscle tone, and aid in dependent edema reduction. If temporary transarticular Steinmann pins or K-wires were utilized to maintain stability, they are typically removed in the outpatient clinic at the 4-week mark, provided there is radiographic evidence of maintenance of alignment.
Phase II: Transition and Early Mobilization (6 to 10 Weeks)
The transition to Phase II occurs at exactly 6 weeks post-injury. This timeline is critical; Zimmer and Johnson's seminal investigation into immobilization duration demonstrated a significantly higher incidence of chronic subtalar instability when the period of rigid immobilization was shortened and early hindfoot exercises were instituted prematurely. At 6 weeks, the robust peritalar ligaments have achieved sufficient preliminary tensile strength to tolerate controlled motion.
Cast immobilization is discontinued, and the patient is transitioned into a custom lace-up foot and ankle leather corset or a rigid controlled ankle motion (CAM) boot. Formal physical therapy is initiated. The focus is on active, gravity-assisted inversion, eversion, dorsiflexion, and plantarflexion of the foot and ankle. Passive, forceful stretching by the therapist is strictly avoided, as it can disrupt the maturing collagen cross-links. Weight-bearing is progressively advanced to tolerance while wearing the CAM boot and utilizing crutches. The boot is worn for at least an additional 4 weeks to control the inevitable dependent edema and provide mechanical support to the healing soft tissues.
Phase III: Maturation and Strengthening (10+ Weeks)
By 8 to 10 weeks post-injury, patients should comfortably achieve full weight-bearing status. They are gradually transitioned out of the CAM boot and into supportive, stiff-soled athletic footwear, often supplemented with a custom orthotic to support the medial longitudinal arch and control hindfoot valgus/varus stress. Physical therapy shifts focus toward proprioceptive training, balance exercises (e.g., BAPS board), and advanced strengthening of the peroneal and posterior tibial musculature to provide dynamic stability to the hindfoot.
Patient counseling during this phase is imperative. The surgeon must reiterate that the foot and ankle will likely continue to swell intermittently for up to 12 to 18 months post-injury. Furthermore, the patient must understand that the midfoot and hindfoot will feel mechanically stiff for several months. A permanent loss of 20% to 50% of normal subtalar inversion and eversion excursion is a common, expected, and largely unavoidable outcome, even following a perfectly executed anatomic reduction. Patients must be prepared for long-term difficulty when navigating uneven terrain, ladders, or slanted surfaces.
Summary of Landmark Literature and Clinical Guidelines
The contemporary surgical management of subtalar dislocations is heavily informed by several landmark academic studies that have shaped our understanding of the pathoanatomy, the necessity of advanced imaging, and the long-term prognostic factors. A thorough grasp of this literature is essential for the practicing orthopedic surgeon and serves as the foundation for evidence-based clinical guidelines.
The critical role of advanced cross-sectional imaging was definitively established by Bibbo et al. In their comprehensive review of subtalar dislocations, they emphasized the absolute necessity of obtaining a computed tomography (CT) scan after the reduction of the dislocation. Their series demonstrated that patients who sustained a subtalar dislocation had an exceptionally high incidence of additional osseous abnormalities—such as osteochondral shear fractures of the talar dome, lateral process fractures, and intra-articular debris—that were initially missed on standard plain radiographs. This paradigm shift mandates that post-reduction CT is no longer optional, but rather the standard of care to dictate the need for delayed definitive internal fixation or joint debridement.
The impact of these associated fractures on long-term outcomes was previously highlighted by DeLee and Curtis. After reviewing a cohort of subtalar dislocations observed for an average of 35 months, they concluded that the presence of an osteochondral fracture seen on post-reduction imaging is a critical prognosticator. They strongly advocated that open reduction and internal fixation (ORIF) or meticulous excision of the osteochondral fragment significantly reduces the risk of rapidly progressive degenerative arthritis. Their work underscores the principle that articular congruity and the removal of third-body wear particles are paramount in preserving subtalar joint longevity.
Regarding the conservative management and immobilization protocols, Zimmer and Johnson investigated the optimal duration of cast immobilization. Their findings challenged the trend of early mobilization, noting a frequent and problematic incidence of chronic subtalar instability when the period of immobilization was shortened. Based on their biomechanical and clinical observations, a strict 6 weeks of rigid cast immobilization is now the universally recommended guideline to allow the massive, robust peritalar ligaments (specifically the interosseous and cervical ligaments) to heal adequately before subjecting them to tensile loads.
Finally, the devastating nature of severe and open injuries was documented in a long-term review by Goldner et al. Reviewing adolescents and adults at an average of 18 years after a type III open subtalar dislocation, they noted catastrophic associated injuries, including massive tibial nerve injuries, posterior tibial tendon ruptures, and severe articular fractures. Crucially, they found avascular necrosis (AVN) in the body of the talus in one-third of the patients, with approximately half eventually requiring major salvage procedures such as subtalar or triple arthrodesis. This study serves as a stark reminder of the guarded prognosis associated with high-energy, open peritalar trauma, reinforcing the need for aggressive initial management and realistic patient counseling.
