Operative Fixation of the Lateral Malleolus: Surgical Guide
Key Takeaway
Anatomical reduction and stable internal fixation of the lateral malleolus are paramount in restoring the ankle mortise. This guide details the operative management of lateral malleolar fractures, emphasizing surgical sequencing in bimalleolar patterns, lateral and posterolateral approaches, and precise lag screw techniques. By restoring fibular length and rotation, surgeons re-establish the critical lateral buttress of the ankle joint, optimizing functional outcomes and minimizing post-traumatic arthrosis.
Comprehensive Introduction and Patho-Epidemiology
Ankle fractures represent one of the most frequently encountered injuries in orthopedic traumatology, accounting for approximately 10% of all fractures evaluated in emergency departments and exhibiting an incidence rate of roughly 187 per 100,000 individuals annually. The epidemiological profile of these injuries demonstrates a classic bimodal distribution. The first peak occurs in young, active males, typically resulting from high-energy mechanisms such as athletic trauma, motor vehicle collisions, or falls from significant heights. The second, increasingly prominent peak involves older females, where low-energy torsional forces acting upon osteoporotic bone lead to complex fracture patterns. As the global population ages, the incidence of fragility-related ankle fractures continues to rise, presenting unique challenges regarding bone quality, soft tissue envelope viability, and the imperative for early mobilization.
The lateral malleolus, representing the distal continuation of the fibula, is the cornerstone of the ankle mortise. Its anatomical integrity is absolutely paramount for maintaining the congruency of the tibiotalar articulation. Fractures of the lateral malleolus are most commonly classified using the Danis-Weber system, which categorizes fractures based on their location relative to the distal tibiofibular syndesmosis (Type A: infrasyndesmotic, Type B: trans-syndesmotic, Type C: suprasyndesmotic). Alternatively, the Lauge-Hansen classification provides a more mechanistic understanding, detailing the position of the foot at the time of injury (supination or pronation) and the direction of the deforming force (external rotation, adduction, or abduction). The Supination-External Rotation (SER) mechanism is the most prevalent, accounting for up to 70% of all ankle fractures, sequentially injuring the anterior inferior tibiofibular ligament (AITFL), the lateral malleolus, the posterior inferior tibiofibular ligament (PITFL) or posterior malleolus, and finally the medial malleolus or deltoid ligament.
Historically, the management of lateral malleolar fractures was predominantly non-operative, relying on closed reduction and prolonged cast immobilization. However, the evolution of modern orthopedic principles, pioneered by the Arbeitsgemeinschaft für Osteosynthesefragen (AO) foundation, has unequivocally demonstrated that non-operative management of unstable ankle fractures frequently leads to malunion, chronic instability, and accelerated post-traumatic arthrosis. The contemporary standard of care dictates that any displacement of the talus within the mortise, or any shortening/rotation of the fibula, mandates precise operative intervention. The primary objective of operative fixation is the absolute anatomical restoration of the lateral column, which indirectly reduces the talus, restores normal joint kinematics, and permits early functional rehabilitation.
Detailed Surgical Anatomy and Biomechanics
The ankle joint is a highly congruent, weight-bearing hinge joint that relies heavily on the precise anatomical relationship between the talus, the distal tibia, and the distal fibula. The lateral malleolus acts as the critical lateral buttress of the ankle mortise, containing the talus within the tibial plafond. The distal fibula is housed within the incisura fibularis of the distal tibia, a concave facet that provides inherent bony stability. This articulation is further stabilized by the syndesmotic ligamentous complex, comprising the AITFL, the PITFL, the transverse tibiofibular ligament, and the robust interosseous membrane. Inferiorly, the lateral collateral ligamentous complex—consisting of the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL)—tethers the distal fibula to the hindfoot, orchestrating complex multi-planar stability.
Biomechanical studies have classically demonstrated the unforgiving nature of the tibiotalar articulation. The landmark cadaveric studies by Ramsey and Hamilton (1976) illustrated that even a 1-millimeter lateral shift of the talus can decrease the tibiotalar contact area by up to 42%. This drastic reduction in surface area leads to exponentially increased peak contact stresses across the articular cartilage, precipitating the rapid onset of post-traumatic osteoarthritis. Furthermore, Yablon et al. established that the talus faithfully follows the lateral malleolus; therefore, any residual shortening, external rotation, or lateral translation of the fibula will result in a corresponding subluxation of the talus.
The fibula is not merely a static buttress; it is a dynamic weight-bearing structure. During the stance phase of the gait cycle, the fibula transmits approximately 16% to 17% of the total axial load applied to the lower extremity. This load transmission increases significantly with ankle dorsiflexion as the wider anterior dome of the talus engages the mortise, tensioning the syndesmosis and externally rotating the fibula slightly. Consequently, operative fixation must not only restore static anatomy but must also possess sufficient mechanical rigidity to withstand these dynamic torsional and axial forces during the critical early phases of bone healing. Failure to restore the exact length of the fibula disrupts this intricate load-sharing mechanism, overloading the medial compartment and the deltoid ligament.
Exhaustive Indications and Contraindications
The decision to proceed with operative fixation of the lateral malleolus hinges on a meticulous assessment of mortise stability. The overarching indication for surgery is any fracture pattern that disrupts the congruency of the tibiotalar joint. Isolated lateral malleolus fractures with no medial injury (stable Weber B / Lauge-Hansen SER II) can often be managed non-operatively. However, if there is clinical or radiographic evidence of medial-sided injury—such as a medial malleolus fracture or a complete rupture of the deltoid ligament (bimalleolar equivalent)—operative intervention is strictly indicated. The integrity of the deltoid ligament is routinely assessed via a gravity stress radiograph or a manual external rotation stress test. A medial clear space exceeding 4 millimeters, or a space greater than the superior clear space, is pathognomonic for deltoid incompetence and mandates fibular osteosynthesis to restore the lateral buttress.
All Weber C (suprasyndesmotic) fractures are inherently unstable due to the disruption of the syndesmotic complex and require operative fixation of the fibula followed by syndesmotic stabilization. Bimalleolar and trimalleolar fractures are absolute indications for surgery, as the multi-column disruption precludes maintenance of reduction via closed means. Open fractures, fractures associated with vascular compromise, and fractures in the polytrauma patient requiring early mobilization also represent absolute indications for immediate or staged operative intervention. In cases of severe soft tissue compromise (e.g., fracture blisters, massive edema), a staged protocol utilizing temporary external fixation spanning the ankle joint is indicated until the soft tissue envelope permits safe definitive internal fixation.
Contraindications to operative fixation must be carefully weighed against the near-certainty of poor functional outcomes with non-operative management of unstable fractures. Absolute contraindications include active deep infection at the surgical site and critically ischemic limbs where surgical incisions would inevitably lead to necrosis and amputation. Relative contraindications require nuanced clinical judgment. Patients with severe peripheral neuropathy, particularly those with Charcot neuroarthropathy, are at an extraordinarily high risk for hardware failure, nonunion, and ulceration. In such populations, conventional fixation may be insufficient, and augmented techniques (e.g., multi-planar locking plates, tibiotalocalcaneal arthrodesis nails, or fine-wire circular external fixators) must be considered. Similarly, non-ambulatory patients or those with profound medical comorbidities precluding safe anesthesia may be managed non-operatively, accepting the resultant malunion in favor of preserving life.
| Clinical Scenario | Indication Status | Rationale and Considerations |
|---|---|---|
| Weber B with Medial Clear Space >4mm | Absolute Indication | Indicates deltoid ligament rupture (bimalleolar equivalent). Fibular fixation is required to pull the talus laterally and restore mortise congruency. |
| Bimalleolar / Trimalleolar Fractures | Absolute Indication | Complete loss of mortise stability. High risk of early arthrosis and chronic subluxation if managed non-operatively. |
| Weber C (Suprasyndesmotic) Fractures | Absolute Indication | Inherent syndesmotic disruption. Requires fibular length restoration followed by syndesmotic screw or suture-button fixation. |
| Open Fractures of the Ankle | Absolute Indication | Requires emergent irrigation, debridement, and stabilization to prevent deep infection and protect neurovascular structures. |
| Severe Peripheral Vascular Disease (PVD) | Relative Contraindication | High risk of wound necrosis and amputation. Requires vascular surgery consultation and optimization prior to any incision. |
| Active Local Soft Tissue Infection | Absolute Contraindication | Hardware placement in an infected field guarantees biofilm formation and catastrophic failure. |
| Severe Neuropathy / Charcot Arthropathy | Relative Contraindication | Standard AO fixation frequently fails. Requires super-constructs, prolonged immobilization, or primary arthrodesis techniques. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the foundation of successful orthopedic trauma surgery. Standard radiographic evaluation must include orthogonal views: a true anteroposterior (AP), a lateral, and a mortise view. The mortise view is obtained by internally rotating the leg approximately 15 to 20 degrees, which aligns the x-ray beam perpendicular to the transmalleolar axis, thereby profiling the entire articular space without fibular overlap. The surgeon must meticulously assess these images for fibular shortening (evaluating the Shenton's line of the ankle or the "dime sign" at the distal tip of the fibula), the presence of comminution, and the exact morphology of the fracture lines to determine the trajectory for interfragmentary lag screws.
In contemporary practice, the threshold for obtaining a preoperative computed tomography (CT) scan has lowered significantly. CT imaging is highly recommended for all trimalleolar fractures, fractures with suspected articular impaction (die-punch fragments), or cases with complex comminution. CT allows for the precise evaluation of the posterior malleolus, classifying it according to the Haraguchi or Bartoníček systems, which dictates whether a posterolateral approach is required for direct posterior fixation. Preoperative templating, whether digital or on hard-copy radiographs, allows the surgeon to anticipate the required plate length, the number of cortices needed for adequate fixation proximal and distal to the fracture, and the optimal trajectory for syndesmotic positioning if required.
Patient positioning is critical for optimizing surgical access and facilitating unhindered intraoperative fluoroscopy. The patient is placed supine on a fully radiolucent operating table. A sandbag or gel bump is placed under the ipsilateral hip to internally rotate the leg. This maneuver neutralizes the natural external rotation of the lower extremity, bringing the lateral malleolus directly anterior and parallel to the floor, which greatly facilitates the surgical approach and hardware placement. A well-padded pneumatic tourniquet is applied to the proximal thigh to ensure a bloodless surgical field, optimizing visualization of the delicate articular structures and fracture lines. The C-arm fluoroscopy unit is positioned on the contralateral side of the table, draped sterilely, and must be capable of freely rotating between AP, mortise, and lateral projections without compromising the sterile field or requiring the surgeon to alter the leg's position drastically.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of lateral malleolar fixation requires a deep understanding of soft tissue handling, fracture mechanics, and precise implant application. The sequence of fixation in complex trauma is a critical strategic decision. Standard orthopedic doctrine dictates reducing and internally fixing the lateral malleolus before the medial side. By restoring fibular length and rotation first, the surgeon utilizes the intact syndesmotic or lateral collateral ligaments to indirectly reduce the talus, which then acts as a template for medial malleolar reduction. However, a critical exception exists: in the presence of severe lateral comminution, attempting to restore fibular length first can lead to iatrogenic malreduction. In such cases, fixing a simple medial malleolar fracture first perfectly positions the talus, allowing the surgeon to use the talus to gauge the correct length and rotation of the comminuted fibula.
The Direct Lateral Approach
The direct lateral longitudinal incision is the workhorse approach for the vast majority of lateral malleolar fractures. A longitudinal incision, typically 10 to 15 centimeters in length, is made directly over the lateral aspect of the fibula, extending distally to the tip of the lateral malleolus. The surgeon must be acutely aware of the superficial peroneal nerve, which crosses the fibula from anterior to posterior approximately 10 to 12 cm proximal to the distal tip. Dissection must remain strictly subfascial or supraperiosteal. The periosteum is incised longitudinally directly over the fracture site and elevated minimally—only enough to expose the fracture edges and allow for anatomical reduction. Excessive periosteal stripping devitalizes the cortical bone fragments, strips the blood supply provided by the surrounding muscle envelope, and drastically increases the risk of delayed union or nonunion.
The Posterolateral Approach
Alternatively, a posterolateral incision is utilized when a posterior antiglide plating technique is planned or when a posterior malleolar fracture must be addressed concurrently. The incision is placed midway between the posterior border of the fibula and the lateral border of the Achilles tendon. Blunt dissection through the subcutaneous tissues must identify and protect the sural nerve and the short saphenous vein, which are typically retracted laterally. The deep fascia is incised, and the plane is developed between the peroneal tendons (retracted laterally) and the flexor hallucis longus (retracted medially). This internervous plane provides excellent, direct access to the posterior surface of the fibula and the posterior malleolus, allowing for concurrent fixation of both structures through a single surgical window.
Lag Screw and Neutralization Plating
For simple, oblique fractures (e.g., classic Weber B patterns) where the bone stock is robust and there is no comminution, interfragmentary compression is the biomechanical gold standard. The fracture is anatomically reduced using a pointed reduction forceps. If the fracture obliquity allows, one or two 3.5 mm or 2.7 mm cortical lag screws are inserted from anterior to posterior. A 3.5 mm glide hole is drilled in the near cortex, followed by a 2.5 mm thread hole in the far cortex using a drill sleeve. The near cortex is countersunk to prevent the screw head from causing stress concentrations. The screws must fully engage the posterior cortex but must not protrude excessively, as prominent hardware will impinge upon the peroneal tendon sheaths, leading to severe tenosynovitis or rupture. Following lag screw insertion, a neutralization plate (typically a one-third tubular plate or an anatomically contoured locking plate) is applied to the lateral or posterolateral aspect of the fibula to protect the lag screws from torsional, bending, and shear forces during the healing phase.
Intramedullary Fixation Techniques
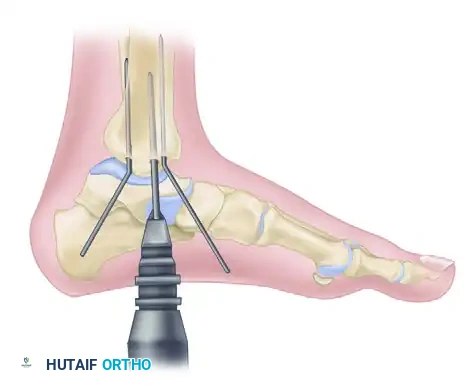
In scenarios where the fracture is strictly transverse (e.g., certain Weber A or high Weber C patterns), interfragmentary lag screw fixation is geometrically impossible. Furthermore, in elderly patients with severe osteoporosis or compromised soft tissue envelopes where extensive plating poses a high risk of wound dehiscence, intramedullary fixation offers a minimally invasive alternative. Techniques utilizing modern fibular nails involve a small incision at the tip of the lateral malleolus. The medullary canal is accessed by carefully splitting the fibers of the calcaneofibular ligament (CFL) longitudinally. The entry point must be perfectly centralized on the distal tip of the fibula in both the AP and lateral planes to prevent angular malalignment. The canal is reamed, and the intramedullary device is advanced across the fracture site under fluoroscopic guidance. Proximal and distal interlocking screws are then placed percutaneously to provide length and rotational stability.
Concurrent Medial Malleolar Fixation
Once the lateral column is definitively stabilized, attention is directed to the medial malleolus to restore the medial articular surface and the competence of the deltoid ligament complex. The medial malleolus is exposed via a standard anteromedial or direct medial incision. The fracture site is debrided of interposed periosteum or hematoma. The fragment is anatomically reduced and provisionally held with a pointed reduction forceps.
The standard AO technique utilizes partially threaded cancellous screws to achieve robust interfragmentary compression. The distal fragment is held reduced with two smooth Kirschner wires (K-wires) driven from the tip of the medial malleolus, perpendicular to the fracture plane, into the distal tibial metaphysis. These wires provide rotational control and provisional stability.
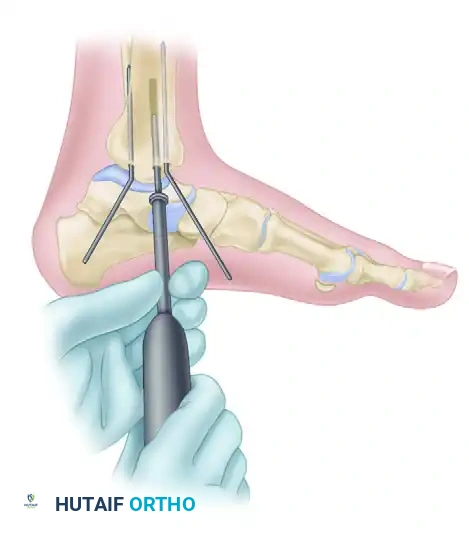
FIGURE 54-6 A: AO technique for internal fixation of the medial malleolus. A 3.2 mm hole is drilled while the distal fragment is held anatomically reduced with two Kirschner wires, which are bent to stay out of the way of the drill. The length of the hole is then measured using a depth gauge.
A 3.2 mm drill bit is used to drill the core trajectory for a 4.0 mm partially threaded cancellous screw. The length is meticulously measured. In cases of dense, young bone, tapping may be required; however, in osteoporotic bone, insertion of the malleolar screw without tapping is highly preferred to maximize thread purchase, radial impaction of the cancellous bone, and ultimate pull-out strength.
FIGURE 54-6 B: Insertion of the malleolar screw without tapping. The Kirschner wires are removed only after the screw is fully tightened and compression is achieved.
A single screw provides excellent compression but poor rotational stability. Therefore, two parallel 4.0 mm cancellous screws are standardly utilized. If the fragment is small, comminuted, or osteoporotic, a tension band compression wiring technique is employed. This construct utilizes two parallel K-wires and a figure-of-eight stainless steel wire loop to convert the distracting forces of the deltoid ligament into dynamic compressive forces at the fracture site during early mobilization.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, operative fixation of the lateral malleolus carries a distinct complication profile, primarily dictated by the precarious nature of the soft tissue envelope surrounding the ankle joint. The lateral malleolus is subcutaneous, with virtually no intervening muscle or adipose tissue to provide vascular coverage. Consequently, wound healing complications are the most frequently encountered adverse events, particularly in high-risk populations such as diabetics, smokers, and the elderly.
Wound dehiscence and superficial surgical site infections occur in approximately 3% to 5% of cases, while deep infections requiring surgical debridement and potential hardware removal occur in 1% to 2%. Prevention requires meticulous handling of the skin edges, avoiding excessive retraction, utilizing full-thickness fasciocutaneous flaps, and ensuring tension-free closure. If a deep infection develops, aggressive operative debridement, targeted intravenous antibiotic therapy, and retention of the hardware (if stable) until clinical union is achieved is the standard salvage protocol. If the hardware is loose or the bone is frankly necrotic, the hardware must be explanted, and stability maintained via external fixation.
Hardware prominence is a highly prevalent complication, reported in up to 30% of patients. The lateral plates and screw heads frequently cause mechanical irritation, particularly in thin patients or athletes wearing rigid footwear such as ski boots or ice skates. Utilizing low-profile anatomical plates and meticulously countersinking screw heads mitigates this risk. Routine hardware removal is generally not recommended due to the risk of nerve injury and refracture; however, symptomatic hardware can be removed after complete radiographic consolidation (typically 9 to 12 months post-operatively).
Malunion and nonunion are catastrophic mechanical failures. Failure to restore the exact length and rotation of the fibula results in a widened ankle mortise, leading to rapid, irreversible joint degeneration. Intraoperative mortise views must be scrutinized to ensure the "dime sign" is restored and the medial clear space is perfectly equal to the superior clear space. If a malunion is identified post-operatively, a complex reconstructive fibular osteotomy, often requiring structural bone grafting and revision plating, is mandated to salvage the joint. Nerve injuries, specifically to the superficial peroneal nerve (lateral approach) or sural nerve (posterolateral approach), result in painful neuromas or sensory deficits in up to 5% of cases. Gentle retraction and strict adherence to internervous planes are mandatory for avoidance.
| Complication | Estimated Incidence | Avoidance Strategy and Salvage Management |
|---|---|---|
| Wound Dehiscence / Superficial Infection | 3% - 5% | Avoidance: Gentle soft tissue handling, full-thickness flaps, delay surgery until edema subsides (wrinkle sign). Salvage: Local wound care, oral antibiotics. |
| Deep Surgical Site Infection | 1% - 2% | Avoidance: Strict sterile technique, prophylactic antibiotics, optimization of host factors (HbA1c). Salvage: Emergent I&D, IV antibiotics, retain stable hardware until union, or switch to external fixation. |
| Symptomatic Hardware Prominence | 15% - 30% | Avoidance: Use low-profile or 1/3 tubular plates, countersink lag screws, avoid excessively long posterior screws. Salvage: Hardware explantation after 9-12 months once radiographic union is confirmed. |
| Fibular Malunion (Shortening/Rotation) | 2% - 5% | Avoidance: Anatomic reduction, use of the talus as a template, intraoperative assessment of Shenton's line. Salvage: Revision surgery with fibular lengthening osteotomy and structural bone grafting. |
| Iatrogenic Nerve Injury (SPN or Sural) | 3% - 5% | Avoidance: Subfascial dissection, identify and protect nerves, avoid aggressive retraction. Salvage: Gabapentinoids, desensitization therapy, surgical neuroma excision and capping for refractory cases. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following lateral malleolar fixation must be carefully tailored to the individual patient, taking into account the bone quality, the mechanical rigidity of the fixation construct, the status of the syndesmosis, and patient compliance. The historical paradigm of prolonged cast immobilization has been largely supplanted by protocols emphasizing early functional mobilization to optimize cartilage nutrition, prevent capsular contracture, and accelerate return to function.
Phase I (0-2 Weeks): Tissue Protection and Edema Control
Immediately post-operatively, the ankle is immobilized in a well-padded short leg splint or a bulky Jones dressing in neutral dorsiflexion. The patient is instructed to maintain strict non-weight-bearing status on the operative extremity. Elevation above the level of the heart and continuous cryotherapy are aggressively emphasized to manage post-operative edema, mitigate pain, and protect the healing surgical incisions. Deep vein thrombosis (DVT) prophylaxis is administered according to institutional protocols and patient risk stratification.
Phase II (2-6 Weeks): Early Motion and Protected Weight-Bearing
At the two-week mark, assuming uncomplicated wound healing, sutures or staples are removed. The patient is transitioned from the rigid splint to a removable controlled ankle motion (CAM) boot. Active range of motion (ROM) exercises, specifically focusing on sagittal plane dorsiflexion and plantarflexion, are initiated out of the boot multiple times daily. Inversion and eversion are typically restricted to protect medial/lateral ligamentous healing. Weight-bearing status remains a topic of debate; however, modern literature supports transitioning to touch-down or partial weight-bearing in the CAM boot for patients with robust, stable fixation, whereas osteoporotic patients or those with syndesmotic fixation may remain strictly non-weight-bearing for a full 6 weeks.
Phase III (6-12 Weeks): Progressive Loading and Strengthening
Clinical and radiographic evaluation is performed at the 6-week interval. If orthogonal radiographs demonstrate bridging callus and the fracture site is clinically non-tender to palpation, progressive weight-bearing is initiated, weaning from the CAM boot to an ankle brace and standard footwear over a 2-to-3-week period. Physical therapy is formalized, focusing on proprioceptive retraining (e.g., BAPS board, single-leg stance), aggressive peroneal strengthening to stabilize the lateral column, and Achilles tendon stretching to overcome any residual equinus contracture.
Phase IV (3-6 Months): Return to High-Level Function
During this final phase, the patient is transitioned to regular, unbraced footwear for all activities of daily living. Physical therapy progresses to functional, dynamic stability exercises. High-impact activities, plyometrics, and sports-specific training are gradually reintroduced as lower extremity strength, endurance, and functional dynamic stability normalize. Patients are counseled that maximal medical improvement, including the complete resolution of dependent swelling and achievement of final range of motion, may take up to 12 to 18 months post-injury.
Summary of Landmark Literature and Clinical Guidelines
The operative management of lateral malleolar fractures is underpinned by several decades of rigorous biomechanical research and high-level clinical trials. The foundational biomechanical principles were established by Ramsey and Hamilton in 1976, whose seminal paper in the Journal of Bone and Joint Surgery demonstrated the catastrophic 42% loss of tibiotalar contact area with a mere 1 mm of lateral talar shift. This study remains the most frequently cited justification for the absolute necessity of anatomic mortise restoration. Following this, Yablon et al. (1977) published their critical work identifying the lateral malleolus, rather than the medial malleolus, as the primary key to the anatomical reduction of the bimalleolar ankle fracture, shifting the surgical paradigm toward the "lateral-first" sequence of fixation.
In the modern era, clinical guidelines have focused heavily on optimizing postoperative rehabilitation and addressing syndesmotic instability. A landmark multicenter randomized controlled trial by the Canadian Orthopaedic Trauma Society (COTS) evaluated early weight-bearing and mobilization versus cast immobilization following operative fixation of ankle fractures. The study demonstrated that early mobilization in a removable brace led to significantly faster return to work and improved early functional scores without increasing the rate of hardware failure or loss of reduction, fundamentally altering postoperative protocols globally.
Furthermore, the management of concurrent syndesmotic injuries has seen a paradigm shift. Traditional rigid fixation with metallic syndesmotic screws is increasingly being challenged by dynamic fixation techniques utilizing suture-button constructs. Recent prospective randomized trials and meta-analyses have shown that suture-button fixation provides equivalent biomechanical stability to screws while allowing for physiological micromotion of the fibula, potentially reducing the rates of malreduction and eliminating the need for routine hardware removal. These evolving guidelines highlight the dynamic nature of orthopedic traumatology, where historical biomechanical truths are continuously synthesized with modern implant technology to optimize patient outcomes.
