Mastering the Surgical Management of Tibial Pilon and Unstable Ankle Fractures
Key Takeaway
Tibial pilon fractures represent a complex spectrum of distal tibia articular injuries driven by high-energy axial compression or rotational forces. Successful management requires meticulous soft tissue assessment, precise preoperative CT planning, and often a staged surgical approach. This guide details the biomechanics, AO/OTA and Rüedi-Allgöwer classifications, and step-by-step operative techniques—including spanning external fixation and delayed open reduction and internal fixation (ORIF)—to optimize functional outcomes and minimize devastating wound complications.
Comprehensive Introduction and Patho-Epidemiology
The management of unstable ankle fracture-dislocations and tibial pilon (plafond) fractures represents one of the most formidable and unforgiving challenges in the realm of orthopedic trauma surgery. These injuries encompass a remarkably broad spectrum of skeletal and soft tissue disruption, ranging from low-energy rotational fractures typically seen in athletic injuries to devastating, high-energy axial compression injuries sustained in motor vehicle collisions, industrial accidents, or falls from significant heights. The term "pilon," introduced by Destot in 1911, translates to "pestle," accurately describing the mechanism wherein the talus is driven forcefully into the distal tibial articular surface, resulting in explosive comminution and catastrophic articular cartilage damage.
Historically, the orthopedic community approached these fractures with the traditional AO principles of aggressive early open reduction and internal fixation (ORIF), prioritizing immediate anatomical restoration of the articular surface and rigid stabilization. In the context of high-energy pilon fractures, this philosophy led to disastrous outcomes. Early extensive surgical exposures through profoundly traumatized soft tissue envelopes resulted in catastrophic complications, including deep wound infections, massive flap necrosis, osteomyelitis, and, ultimately, a high rate of secondary amputation. The soft tissue envelope surrounding the distal tibia is notoriously thin, lacking robust muscle coverage and relying on a tenuous, easily compromised vascular supply.
Consequently, modern orthopedic principles dictate a profound and uncompromising respect for the soft tissue envelope, heavily favoring a staged approach to reconstruction. The contemporary paradigm—often referred to as "span, scan, and plan"—prioritizes immediate skeletal stabilization and restoration of length via external fixation, allowing the soft tissues to declare themselves and recover before any definitive internal fixation is attempted. This evolution in thought has drastically reduced the incidence of catastrophic wound complications while still allowing for meticulous articular reconstruction.
Epidemiologically, tibial pilon fractures account for approximately 1% to 10% of all lower extremity fractures and 3% to 10% of all tibial fractures. They exhibit a bimodal distribution, affecting young males involved in high-energy trauma and older individuals sustaining low-energy osteoporotic fractures. The incidence of concomitant injuries is exceptionally high in the high-energy cohort, with a significant percentage of patients presenting with polytrauma, including closed head injuries, thoracic trauma, and axial skeleton fractures. Understanding the patho-epidemiology of these injuries is the critical first step in formulating a comprehensive, patient-specific treatment algorithm that balances the competing demands of skeletal stability and soft tissue viability.
Detailed Surgical Anatomy and Biomechanics
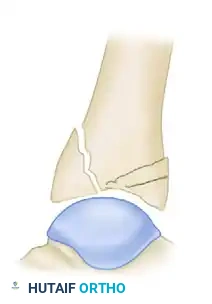
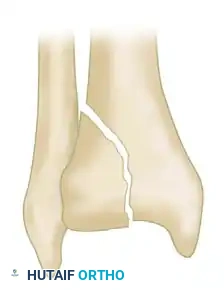
A masterful command of distal tibial anatomy and the biomechanics of injury is non-negotiable for the orthopedic surgeon attempting to reconstruct the tibial plafond. The distal tibia expands into a metaphyseal flare, transitioning from dense cortical diaphyseal bone to a cancellous metaphyseal bed supporting the articular surface. The articular surface itself is concave in both the sagittal and coronal planes, articulating with the talar dome to form a highly congruent, weight-bearing joint. The plafond is anatomically divided into three primary columns or fragments: the medial malleolus, the anterolateral (Chaput) fragment, and the posterior (Volkmann) fragment. The syndesmotic ligamentous complex binds the distal fibula within the incisura fibularis of the tibia, maintaining the integrity of the ankle mortise.
The vascular anatomy of the distal leg is organized into distinct angiosomes—three-dimensional blocks of tissue supplied by specific source arteries. The anterior tibial artery supplies the anterolateral angiosome, the posterior tibial artery supplies the medial and posteromedial angiosomes, and the peroneal artery supplies the anterolateral and posterolateral regions. Surgical incisions must be meticulously planned to respect these angiosomal boundaries. Violating multiple angiosomes or creating narrow skin bridges between parallel incisions critically compromises cutaneous perfusion, precipitating wound dehiscence and deep infection. A minimum skin bridge of 7 cm is the widely accepted standard when dual incisions are required.
The morphology of a distal tibial fracture is directly dictated by the vector and magnitude of the deforming force, as well as the position of the foot at the exact moment of impact. Low-energy rotational variants typically carry a more favorable prognosis. Lauge-Hansen described a pronation-dorsiflexion injury resulting in an oblique medial malleolar fracture, a large anterior lip fracture, a supra-articular fibular fracture, and a posterior tibial fracture. Similarly, Giachino and Hammond identified a pattern driven by external rotation, dorsiflexion, and abduction, yielding an oblique medial malleolus fracture combined with an anterolateral tibial plafond fracture. These injuries generally exhibit minimal metaphyseal comminution, large, reconstructable articular fragments, and forgiving soft tissue envelopes.
Conversely, high-energy axial compression forces drive the talus into the distal tibial articular surface acting as a biological die-punch. This results in severe articular impaction, explosive metaphyseal comminution, and diaphyseal extension. The fibula is fractured in approximately 85% of these high-energy cases, and concomitant talar chondral or osteochondral injuries are frequent. The position of the foot determines the location of maximal articular destruction: plantarflexion drives posterior comminution, neutral position causes central impaction, and dorsiflexion obliterates the anterior plafond.
Dickson, Montgomery, and Field identified a highly prognostic subset of severe pilon fractures characterized by "ground-glass" comminution—defined as more than three articular fragments smaller than 2 mm on CT scan. In their series, post-traumatic arthritis developed in 38% of ankles with ground-glass comminution, compared to 0% in those without it, underscoring the absolute biological limits of anatomical reconstruction in explosive injuries.
The AO/OTA Classification System
Accurate classification is paramount for determining prognosis, guiding surgical strategy, and facilitating academic communication. The Orthopaedic Trauma Association (OTA) system provides the most comprehensive anatomical description, dividing distal tibial fractures into three primary types:
-
Type A (Extra-articular): Fractures involving the distal metaphysis without extension into the tibiotalar joint. Subdivided into A1 (simple), A2 (wedge), and A3 (complex/multifragmentary).
-
Type B (Partial Articular): A portion of the articular surface remains in continuity with the tibial diaphysis. Subdivided into B1 (pure split), B2 (split depression), and B3 (multifragmentary depression).
-
Type C (Complete Articular): The articular surface is entirely disconnected from the diaphysis. Subdivided into C1 (articular simple, metaphysis simple), C2 (articular simple, metaphysis multifragmentary), and C3 (articular multifragmentary).
The Rüedi and Allgöwer Classification
This classic system categorizes pilon fractures based on the degree of displacement and comminution:
-
Type I: Nondisplaced cleavage fractures involving the joint surface.
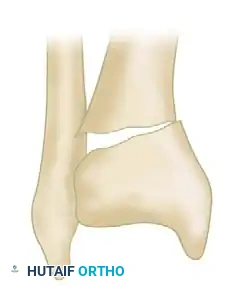
-
Type II: Cleavage-type fractures with significant displacement of the articular surface but minimal comminution.

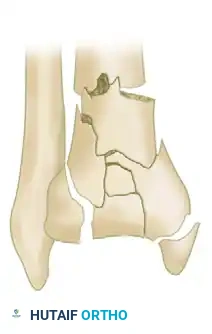
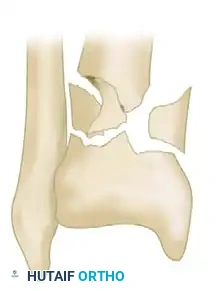
-
Type III: Severe injuries associated with extensive metaphyseal and articular comminution.

Further morphological variations include isolated split depressions and severe metaphyseal comminution, which dictate the necessity for bone grafting and robust buttress plating.


Exhaustive Indications and Contraindications
The decision-making process regarding surgical intervention for tibial pilon fractures is complex and heavily nuanced. The ultimate determinant of surgical timing and the specific operative approach is the condition of the soft tissue envelope. High-energy pilon fractures are frequently associated with severe closed soft tissue trauma or open wounds that preclude immediate internal fixation. The surgeon must meticulously evaluate vascular status, neurological function, and the presence of compartment syndrome or closed degloving injuries (Morel-Lavallée lesions).
The presence of fracture blisters is a pathognomonic indicator of severe cutaneous damage resulting from profound interstitial edema and dermal-epidermal junction shearing. Clear fluid blisters represent epidermal separation and carry a slightly better prognosis, whereas blood-filled blisters indicate deeper dermal injury, rupture of the subpapillary vascular plexus, and a significantly higher risk of full-thickness tissue necrosis if incised. Open fractures must be graded using the Gustilo-Anderson system, while closed injuries should be rigorously graded using the Tscherne classification (Grades 0-III).
Patient optimization is equally critical. Systemic factors such as active smoking, poorly controlled diabetes mellitus (HbA1c > 8.0%), severe peripheral vascular disease, and chronic alcoholism exponentially increase the risk of postoperative wound complications, deep infection, and nonunion. In certain high-risk patient populations, the risks of definitive ORIF may outweigh the benefits, necessitating alternative management strategies such as definitive circular external fixation or primary arthrodesis.
| Category | Indications / Criteria | Contraindications / High-Risk Factors |
|---|---|---|
| Immediate Surgery (Damage Control) | Open fractures (Gustilo-Anderson I-IIIC); Gross clinical instability; Vascular compromise requiring restoration of alignment; Polytrauma (Damage Control Orthopedics). | Hemodynamic instability precluding anesthesia; Unsalvageable limb (Mangled Extremity Severity Score > 7) favoring primary amputation. |
| Definitive ORIF (Delayed) | Resolution of soft tissue edema (positive "wrinkle sign"); Re-epithelialization of fracture blisters; Displaced articular fractures (>2mm step-off); Axial malalignment. | Tscherne Grade III soft tissues (absolute contraindication for early ORIF); Active local infection; Poorly controlled diabetes/vascular disease. |
| Definitive External Fixation | Severe, non-recovering soft tissue compromise; Massive bone loss; Highly non-compliant patient; Severe medical comorbidities precluding prolonged anesthesia. | Lack of surgeon expertise with circular frames; Inability of the patient to manage pin site care. |
| Primary Arthrodesis | Extreme "ground-glass" comminution of the articular surface; Pre-existing severe tibiotalar arthritis; Delayed presentation with established joint destruction. | Reconstructable articular surface in a young, active patient; Active intra-articular infection. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful pilon fracture management. Standard anteroposterior (AP), lateral, and mortise radiographs of the ankle are mandatory upon initial presentation. However, plain films drastically underestimate the complexity of articular impaction and metaphyseal comminution. Traction radiographs, obtained by applying longitudinal traction (via a calcaneal pin or a spanning external fixator) during radiography, are invaluable. They demonstrate the degree to which ligamentotaxis can reduce the fracture, highlighting the fragments that remain impacted and will require direct surgical elevation.
A fine-cut Computed Tomography (CT) scan with 2D multiplanar and 3D surface-rendered reconstructions is the absolute gold standard for preoperative planning. Crucially, the CT scan should be obtained after the application of a spanning external fixator. Scanning the limb in a distracted, length-stable state provides an accurate topographical map of the remaining impacted articular segments (the central die-punch fragments). Ligamentotaxis alone cannot elevate these central fragments because they lack soft tissue attachments. The post-fixation CT allows the surgeon to conceptualize the fracture in three dimensions, plan the exact sequence of fragment reduction, and determine the optimal surgical approach.
Digital templating is performed using the CT data to select the appropriate implants. The surgeon must anticipate the need for specific tools, including fine K-wires, dental picks, small osteotomes, femoral head allograft or synthetic bone void fillers, and a variety of pre-contoured anatomical locking plates.
Patient positioning is critical for facilitating adequate fluoroscopic imaging and surgical access. The patient is typically positioned supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to correct the natural external rotation of the lower extremity, ensuring the patella and the ankle mortise are pointing directly toward the ceiling. This neutral alignment is vital for judging rotational reduction. A sterile tourniquet is applied to the proximal thigh, though its use should be judicious to minimize ischemic insult to an already compromised soft tissue envelope. The entire leg, from the toes to the proximal thigh, is prepped and draped free to allow for intraoperative assessment of mechanical axis and limb length.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of high-energy tibial pilon fractures has universally shifted toward a Two-Stage Delayed Protocol. This paradigm acknowledges that the initial trauma inflicts a severe biological hit to the soft tissues; adding the iatrogenic trauma of immediate open surgery frequently pushes the tissues beyond their capacity to heal.
Stage 1: Damage Control External Fixation
Performed within the first 24 hours of injury, the goal of Stage 1 is to restore limb length, correct gross angular deformity, and provide rigid skeletal stability to allow soft tissue resuscitation. A spanning delta-frame external fixator is the standard construct. Two 5.0mm half-pins are placed in the anterior tibial diaphysis, well proximal to the zone of injury and out of the trajectory of future definitive plates. A centrally threaded transfixion pin is placed through the calcaneal tuberosity, avoiding the neurovascular bundle medially.
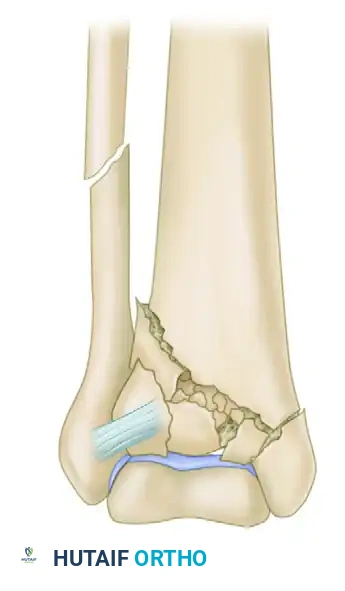
If the fibula is fractured, early ORIF of the fibula can be performed during this stage to restore the lateral column length, provided the lateral soft tissue envelope is pristine. If the lateral tissues are compromised, fibular fixation must be delayed. Once the pins are placed, the frame is assembled and longitudinal traction is applied. The frame is distracted to restore length and roughly align the metaphyseal fragments via ligamentotaxis.
In scenarios of severe instability, profound soft tissue compromise, or polytrauma where a spanning external fixator is unavailable or contraindicated (e.g., austere environments), the Childress transarticular pinning technique serves as a rapid damage-control maneuver.
Surgical Warning: Transarticular pinning violates the subtalar and tibiotalar joints and is strictly a salvage or temporary measure.
The technique involves closed reduction under fluoroscopy, followed by the insertion of a 2.8-mm smooth Steinmann pin into the midline of the plantar sole, 2.5 cm posterior to the calcaneocuboid joint. The pin is advanced through the calcaneus, across the talus, and approximately 10 cm into the distal tibial metaphysis. The pin is left protruding 1.3 cm through the skin, heavily padded, and the leg is immobilized in a well-padded cast.
Stage 2: Definitive Open Reduction and Internal Fixation
Definitive surgery is delayed for 10 to 21 days until the soft tissue envelope has recovered. The clinical indicator for readiness is the complete resolution of pitting edema, marked by the appearance of the "wrinkle sign," and the epithelialization of any fracture blisters.
1. Surgical Approaches:
The choice of approach is dictated by the location of the primary articular fracture lines identified on the post-ex-fix CT scan.
* Anterolateral Approach: Utilized for valgus deformity and anterolateral (Chaput) fragments. The incision is made in line with the fourth ray, developing the internervous interval between the Tibialis Anterior (deep peroneal nerve) and Extensor Digitorum Longus (EDL). This approach provides excellent visualization of the lateral and central plafond.
* Anteromedial Approach: Utilized for varus deformity and large medial malleolar fragments. The incision runs just lateral to the tibial crest and medial to the Tibialis Anterior tendon, preserving the saphenous nerve and vein.
* Posterolateral Approach: Utilized for large posterior (Volkmann) fragments. The interval is between the peroneal tendons and the Flexor Hallucis Longus (FHL).
2. Articular Reconstruction:
The external fixator is typically removed, and the joint capsule is opened to visualize the plafond. The reconstruction proceeds from posterior to anterior and from lateral to medial. The posterior column is reduced first to establish a stable reference point. Impacted central articular fragments (the die-punch) are meticulously elevated using an osteotome or dental pick. The articular surface is provisionally assembled using fine K-wires, utilizing the talar dome as a biological template to ensure congruity. Once anatomical reduction is confirmed fluoroscopically and visually, the fragments are secured with 2.7-mm or 3.5-mm independent lag screws, countersunk beneath the cartilage surface.
3. Metaphyseal Bone Grafting:
Elevation of impacted articular segments inevitably leaves a substantial metaphyseal void. This structural defect must be filled to support the reconstructed articular surface and prevent late subsidence. Cancellous autograft harvested from the iliac crest remains the gold standard, though structural allograft or osteoinductive/osteoconductive bone substitutes (e.g., demineralized bone matrix, calcium phosphate cements) are frequently utilized to minimize donor site morbidity.
4. Plate Fixation:
The reconstructed articular block is then mated to the tibial diaphysis. Pre-contoured anatomical locking plates are utilized to provide angular stable fixation. Minimally invasive percutaneous osteosynthesis (MIPO) techniques are highly encouraged for the diaphyseal extension to preserve the delicate periosteal blood supply. The plate is slid submuscularly along the tibial shaft, and screws are placed percutaneously.
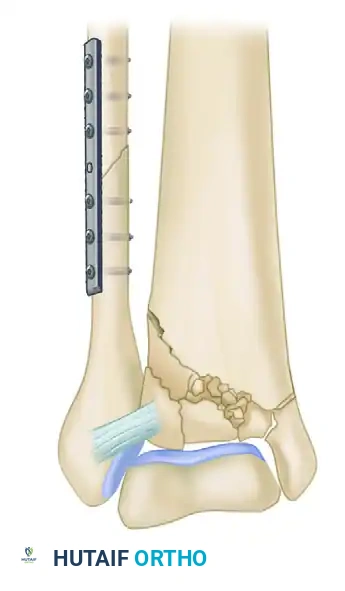

Clinical Example: Postoperative radiographs demonstrating restoration of the articular mortise, correction of the mechanical axis, and stable metaphyseal fixation using a medial locking plate and independent lag screws.
Complications, Incidence Rates, and Salvage Management
Despite meticulous adherence to staged protocols and modern surgical techniques, tibial pilon fractures carry a notoriously high complication rate. The initial energy imparted to the limb results in irreversible cellular damage to both bone and soft tissue, predisposing the patient to a cascade of potential postoperative issues.
Wound dehiscence and deep surgical site infections (SSI) remain the most dreaded early complications. The use of the two-stage protocol has reduced deep infection rates from historic highs of 30-50% down to approximately 5-10%. However, when deep infection occurs, it often necessitates aggressive serial debridements, removal of hardware, placement of antibiotic-impregnated cement spacers, and soft tissue coverage via free tissue transfer (e.g., anterolateral thigh or latissimus dorsi flaps).
Nonunion and delayed union are prevalent due to the extensive metaphyseal comminution and compromised periosteal blood supply. Metaphyseal nonunions often require revision surgery with autologous bone grafting and optimization of mechanical stability. Malunion, particularly in varus or valgus, alters the biomechanics of the ankle joint, rapidly accelerating the onset of post-traumatic osteoarthritis (PTOA).
PTOA is the most common late complication, occurring in up to 50% of high-energy pilon fractures despite anatomical articular reduction. The initial impact causes profound chondrocyte necrosis that cannot be reversed surgically. When conservative measures fail, salvage management typically involves tibiotalar arthrodesis. In cases of severe, recalcitrant infection, intractable pain, or a non-functional limb, below-knee amputation remains a viable and sometimes necessary definitive salvage option to restore patient mobility and quality of life.
| Complication | Estimated Incidence | Primary Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Superficial Wound Necrosis | 10% - 20% | Early surgical timing; Poor flap handling; Smoking; Diabetes. | Local wound care; NPWT; Delayed primary closure; Split-thickness skin grafting. |
| Deep Infection / Osteomyelitis | 5% - 10% | Gustilo-Anderson Type III open injuries; Tscherne Grade III closed injuries; Prolonged operative time. | Radical debridement; Hardware removal; Antibiotic spacers; Free tissue transfer; Suppressive antibiotics. |
| Nonunion / Delayed Union | 10% - 15% | Severe metaphyseal comminution; Periosteal stripping; Inadequate fixation rigidity; Smoking. | Revision internal fixation; Autologous iliac crest bone grafting; Bone marrow aspirate concentrate (BMAC). |
| Post-Traumatic Osteoarthritis | 30% - 50% | Initial chondrocyte necrosis; "Ground-glass" comminution; >2mm articular step-off; Malalignment. | Activity modification; Bracing; Intra-articular injections; Definitive Tibiotalar or Tibiotalocalcaneal Arthrodesis. |
| Amputation (Late) | 2% - 5% | Recalcitrant deep infection; Intractable pain; Severe neurovascular compromise. | Below-knee amputation (BKA) with customized prosthetic fitting. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation of a tibial pilon fracture is a protracted process requiring immense patient compliance and close multidisciplinary collaboration between the orthopedic surgeon and physical therapy team. The primary goals are to protect the delicate soft tissue envelope, maintain the integrity of the internal fixation, and restore functional range of motion (ROM) to the ankle and subtalar joints.
Phase I: Immediate Postoperative (Weeks 0-3)
Following definitive ORIF, wound management is paramount. Incisions must be closed meticulously without tension, utilizing modified Allgöwer-Donati sutures to preserve cutaneous perfusion. Prophylactic application of Negative Pressure Wound Therapy (NPWT) over closed incisions (ciNPT) is frequently utilized to reduce edema, mitigate seroma formation, and promote primary intention healing. The ankle is immobilized in a bulky Jones splint or a rigid posterior splint in neutral dorsiflexion to prevent equinus contracture. The patient is strictly non-weight-bearing (NWB) on the operative extremity. Deep vein thrombosis (DVT) prophylaxis is initiated per institutional protocols.
Phase II: Early Range of Motion (Weeks 3-8)
Once the surgical incisions are fully healed and sutures are removed (typically at 2 to 3 weeks), the splint is transitioned to a removable controlled ankle motion (CAM) boot. Strict NWB status is maintained. The patient is instructed to remove the boot multiple times daily to perform active and active-assisted ROM exercises of the tibiotalar and subtalar joints. Early motion is critical for cartilage nutrition, preventing intra-articular adhesions, and maximizing long-term functional outcomes. Aggressive passive stretching is avoided to prevent displacement of the articular reconstruction.
Phase III: Progressive Weight-Bearing (Weeks 8-12)
At approximately 8 to 10 weeks postoperatively, orthogonal radiographs are obtained to assess for bridging callus across the metaphyseal fracture lines and maintenance of articular congruity. If radiographic evidence of progression toward union is present, the patient may initiate progressive partial weight-bearing (PWB) in the CAM boot, typically starting at 20-30 pounds and advancing by 20 pounds weekly. Physical therapy focuses on proprioception, intrinsic foot muscle strengthening, and gait mechanics.
Phase IV: Full Weight-Bearing and Functional Restoration (Weeks 12+)
Once complete clinical and radiographic union is achieved (usually between 12 to 16 weeks), the patient is transitioned out of the CAM boot into supportive footwear. Full weight-bearing (FWB) is permitted. Rehabilitation intensifies to include closed-kinetic chain exercises, dynamic balance training, and eventually, plyometrics and work-hardening programs. Patients must be counseled that maximum medical improvement (MMI) often takes 12 to 18 months, and some degree of permanent stiffness or episodic swelling is expected.
Summary of Landmark Literature and Clinical Guidelines
The contemporary management of tibial pilon fractures is heavily informed by several landmark studies that fundamentally altered the trajectory of orthopedic trauma care. In the 1980s and early 1990s, early ORIF of high-energy (Rüedi-Allgöwer Type III / AO Type C3) pilon fractures yielded disastrous results. A seminal paper by McFerran et al. reported an unacceptable 54% local complication rate following early definitive fixation, with deep infections frequently necessitating free tissue transfer or resulting in amputation. This highlighted the biological limits of the distal tibial soft tissue envelope.
Subsequently, Watson et al. demonstrated that basing the timing of definitive treatment on the Tscherne soft tissue grade significantly improved outcomes. Their work established the foundation for the modern Two-Stage Delayed Protocol, proving that allowing the soft tissues to recover prior to definitive ORIF drastically reduced wound dehiscence and infection rates. Sirkin and Sanders further popularized this staged approach
