Comprehensive Surgical Management of Bimalleolar Ankle Fractures

Key Takeaway
Bimalleolar ankle fractures disrupt the medial and lateral stabilizing structures of the tibiotalar joint, significantly altering joint kinematics. Operative intervention is typically required to restore articular congruity and prevent post-traumatic arthrosis. Surgical timing is critical, dictated by soft tissue envelopes, with definitive fixation performed either within the first 12 hours or delayed 2 to 3 weeks to allow swelling to subside.
Comprehensive Introduction and Patho-Epidemiology
Bimalleolar ankle fractures represent a profound structural and biomechanical disruption of both the medial and lateral stabilizing complexes of the tibiotalar joint. As one of the most frequently encountered lower extremity fractures in orthopedic traumatology, these injuries carry significant potential for long-term morbidity if not managed with meticulous surgical precision. The tibiotalar joint operates as a highly congruent, weight-bearing hinge; it possesses a unique articular geometry that demands absolute anatomic restoration. Even minor residual displacements or subtle rotational malalignments can precipitate catastrophic alterations in joint kinematics, leading to rapid and irreversible articular cartilage degradation.
The epidemiology of bimalleolar ankle fractures demonstrates a classic bimodal distribution. The first peak occurs in young, active males, typically resulting from high-energy mechanisms such as athletic trauma, motor vehicle collisions, or falls from significant height. These injuries are frequently associated with severe soft tissue compromise, highly comminuted fracture patterns, and concomitant syndesmotic disruption. The second, more rapidly expanding demographic peak involves elderly females, predominantly secondary to low-energy twisting injuries in the setting of osteoporosis. In this osteopenic population, the fracture morphology often presents unique challenges, including poor bone stock for implant purchase, highly comminuted lateral malleolar fractures, and an increased risk of postoperative hardware failure or loss of reduction.
Pathophysiologically, bimalleolar fractures are most accurately conceptualized through the lens of rotational mechanisms, as classically described by the Lauge-Hansen classification system. The vast majority of these injuries follow a Supination-External Rotation (SER) or Pronation-External Rotation (PER) pattern. In an SER injury, the sequence of failure typically begins laterally with disruption of the anterior inferior tibiofibular ligament (AITFL), progresses to a short oblique fracture of the fibula, tears the posterior capsule or posterior malleolus, and ultimately culminates in a transverse avulsion fracture of the medial malleolus or a complete rupture of the deltoid ligament complex. Understanding this sequential energy transfer is absolutely paramount for the operating surgeon, as it dictates not only the fracture morphology but also the required sequence of surgical reduction and fixation.
The economic and functional burden of bimalleolar ankle fractures is substantial. When treated non-operatively, the inherent instability of the bimalleolar injury pattern frequently leads to loss of reduction within the cast, subsequent talar subluxation, and inevitable post-traumatic arthrosis. Consequently, Open Reduction and Internal Fixation (ORIF) has been universally established as the gold standard of treatment. The primary surgical imperatives are clear: restore precise anatomic alignment of the fibula to recreate the lateral buttress, meticulously repair the medial stabilizing structures, stabilize the syndesmotic mortise if necessary, and establish a rigid construct that permits early functional rehabilitation.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of ankle anatomy and biomechanics is the foundational prerequisite for successful surgical intervention. The ankle mortise is a dynamic, multi-ligamentous bony ring composed of the distal tibia (the plafond and medial malleolus), the distal fibula (lateral malleolus), and the talus. The talar dome is trapezoidal, being wider anteriorly than posteriorly. During dorsiflexion, this wider anterior segment engages the mortise, providing maximal bony stability. Conversely, in plantarflexion, the narrower posterior talus occupies the mortise, rendering the joint highly dependent on its ligamentous constraints for stability.
The medial malleolus is divided anatomically into the anterior and posterior colliculi, separated by the intercollicular groove. This distinction is surgically critical because of the differential attachments of the deltoid ligament complex. The superficial deltoid ligament, which resists hindfoot eversion, attaches primarily to the anterior colliculus. However, the deep deltoid ligament—the primary restraint to lateral talar excursion and external rotation—originates from the intercollicular groove and the posterior colliculus. Traumatic avulsions of the anterior colliculus alone may leave the deep deltoid intact, whereas fractures extending into or through the posterior colliculus invariably destabilize the entire medial complex. During surgical approach, aggressive periosteal stripping of the medial malleolus must be strictly avoided to preserve the vascular supply to these critical ligamentous origins.
The lateral malleolus serves as the crucial lateral buttress of the ankle mortise. The distal fibula is tethered to the tibia via the syndesmotic ligament complex, which includes the AITFL, the posterior inferior tibiofibular ligament (PITFL), the transverse tibiofibular ligament, and the interosseous membrane. The fibula sits within the fibular incisura of the distal tibia. Anatomic restoration of fibular length, rotation, and alignment is the absolute cornerstone of ankle fracture management. The talus faithfully follows the lateral malleolus; if the fibula is permitted to heal in a shortened or externally rotated position, the talus will remain laterally subluxated, leading to devastating joint degeneration.
The biomechanical intolerance of the ankle joint to malalignment is well documented in classic orthopedic literature. The seminal biomechanical studies by Ramsey and Hamilton demonstrated that a mere 1 mm lateral shift of the talus reduces the tibiotalar contact area by an astonishing 42%. This exponential decrease in contact area leads to a proportional and drastic increase in peak articular cartilage contact stresses. Because the cartilage of the ankle joint is relatively thin compared to the knee or hip, it is exceptionally vulnerable to these concentrated shear and compressive forces. Therefore, the surgical margin for error in bimalleolar fractures is effectively zero; achieving a congruent mortise with equal medial, lateral, and superior clear spaces on postoperative orthogonal radiographs is non-negotiable.
Exhaustive Indications and Contraindications
The decision-making process for operative intervention in bimalleolar ankle fractures requires a nuanced synthesis of fracture morphology, patient physiology, and soft tissue integrity. While ORIF is the definitive standard of care for displaced bimalleolar fractures, the timing and appropriateness of surgery must be individualized. The soft tissue envelope surrounding the ankle is notoriously thin, with minimal subcutaneous fat or muscle bulk to protect underlying neurovascular structures and surgical implants.
The management of periarticular ankle fractures is heavily dictated by the condition of this soft tissue envelope. Operative treatment is generally limited to two distinct time windows: the "Early" window (less than 12 to 24 hours post-injury) and the "Late" window (10 to 21 days post-injury). If the surgical team can intervene before the onset of massive soft tissue edema, early ORIF is highly advantageous, associated with briefer hospitalizations and diminished postoperative pain. However, if this early window is missed, operating through severely edematous tissue, fracture blisters, or compromised skin exponentially increases the risk of catastrophic wound dehiscence and deep infection. In such delayed scenarios, immediate closed reduction of the fracture-dislocation and application of a well-padded plaster splint are absolutely mandatory to prevent irreversible pressure necrosis of the skin.
| Category | Specific Criteria / Condition | Clinical Rationale and Surgical Implications |
|---|---|---|
| Absolute Indications | Open Fractures | Requires emergent irrigation, debridement, and stabilization to prevent deep joint infection and osteomyelitis. |
| Absolute Indications | Displaced Bimalleolar Fractures | Any displacement > 2mm, lateral talar shift, or widening of the medial clear space dictates surgical restoration of the mortise. |
| Absolute Indications | Irreducible Fracture-Dislocations | Soft tissue interposition (e.g., posterior tibial tendon or deltoid ligament) preventing closed reduction requires open extraction and fixation. |
| Absolute Indications | Concomitant Syndesmotic Injury | Bimalleolar equivalent injuries with syndesmotic diastasis require stabilization to prevent chronic instability and arthrosis. |
| Relative Indications | Severe Osteoporosis | Requires specialized fixation techniques (locking plates, intramedullary augmentation) but still benefits from anatomic restoration. |
| Absolute Contraindications | Active Local Infection | Operating through infected tissue guarantees deep hardware infection; requires temporizing external fixation if unstable. |
| Absolute Contraindications | Non-Ambulatory Patient | Bedbound patients or those with severe dementia who cannot participate in rehab may be managed with cast immobilization, accepting malunion. |
| Absolute Contraindications | Unstable Medical Comorbidities | Recent myocardial infarction, severe uncontrolled heart failure, or critical illness precluding safe anesthesia administration. |
| Relative Contraindications | Severe Soft Tissue Edema / Blisters | Requires delay of definitive ORIF (10-21 days) until the "wrinkle test" is positive to prevent wound dehiscence. |
| Relative Contraindications | Severe Peripheral Neuropathy (Charcot) | High risk of hardware failure and nonunion; requires ultra-rigid fixation, extended non-weight-bearing, and potential primary arthrodesis. |
When surgery is delayed due to soft tissue compromise, the "wrinkle test"—the reappearance of normal skin lines when the ankle is gently dorsiflexed or everted—is the most reliable clinical indicator that swelling has subsided sufficiently to proceed with ORIF. Hemorrhagic fracture blisters indicate deep dermal injury and should be strictly avoided during surgical incisions, whereas clear fluid-filled blisters represent superficial epidermal separation and may be carefully incorporated into the incision if absolutely necessary, though avoidance is always preferred.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the hallmark of the master orthopedic surgeon. Evaluation begins with high-quality, orthogonal plain radiographs: Anteroposterior (AP), Lateral, and Mortise views. The mortise view, obtained with the leg internally rotated 15 to 20 degrees, is critical for assessing the medial clear space, the tibiofibular overlap, and the talocrural angle. A medial clear space greater than 4 mm, or one that is asymmetric compared to the superior clear space, is pathognomonic for lateral talar shift and deltoid ligament incompetence.
While plain radiographs are sufficient for standard bimalleolar patterns, the threshold for obtaining a preoperative Computed Tomography (CT) scan should be exceedingly low. CT imaging is invaluable for identifying occult articular comminution, evaluating the size and trajectory of posterior malleolar fragments (which are frequently present in presumed "bimalleolar" injuries, rendering them trimalleolar), and assessing the presence of marginal impaction of the tibial plafond. Preoperative templating utilizing digital software allows the surgeon to anticipate implant sizes, plate lengths, and optimal screw trajectories, thereby minimizing intraoperative delays and reducing fluoroscopy time.
Patient positioning and operating room setup must be optimized to facilitate unhindered access to both malleoli and seamless fluoroscopic imaging. The patient is typically positioned supine on a radiolucent operating table. A well-padded bump is placed under the ipsilateral hip to internally rotate the lower extremity, bringing the lateral malleolus anteriorly and neutralizing the natural external rotation of the limb. This allows for direct visualization of the fibula while maintaining access to the medial malleolus by simply externally rotating the hip intraoperatively.
A sterile pneumatic tourniquet is applied to the proximal thigh to provide a bloodless surgical field, though it should be used judiciously, particularly in elderly patients with peripheral vascular disease. The C-arm fluoroscopy unit is brought in from the contralateral side of the table, positioned perpendicular to the operative leg. The monitor must be placed in the direct line of sight of the primary surgeon. Prior to skin incision, the surgeon must confirm that perfect AP, Mortise, and Lateral fluoroscopic views can be obtained without obstruction from the table pedestal or the contralateral limb. Prophylactic intravenous antibiotics (typically a first-generation cephalosporin) are administered within 60 minutes prior to tourniquet inflation.
Step-by-Step Surgical Approach and Fixation Technique
The surgical sequence in bimalleolar fractures generally begins with the lateral malleolus. Restoring the length and rotation of the fibula corrects the lateral talar shift and provides a template against which the medial malleolus can be accurately reduced.
Operative Techniques: Lateral Malleolus
The lateral malleolus is approached via a direct lateral or slightly posterolateral longitudinal incision. The posterolateral approach is often preferred as it provides excellent access to the posterior margin of the fibula for antiglide plating and allows for future access to the posterior malleolus if necessary. Dissection is carried down through the subcutaneous tissue, with meticulous care taken to identify and protect the superficial peroneal nerve proximally and the sural nerve distally. Full-thickness fasciocutaneous flaps must be maintained to preserve skin viability.
The fracture site is exposed, and the hematoma is evacuated. The fracture ends are gently debrided with a curette, and the interdigitation of the cortical edges is carefully analyzed. Reduction is typically achieved using a combination of longitudinal traction, internal rotation, and the application of pointed reduction forceps. Anatomic reduction is confirmed visually by matching the cortical interdigitations and fluoroscopically by restoring the Shenton line of the ankle.
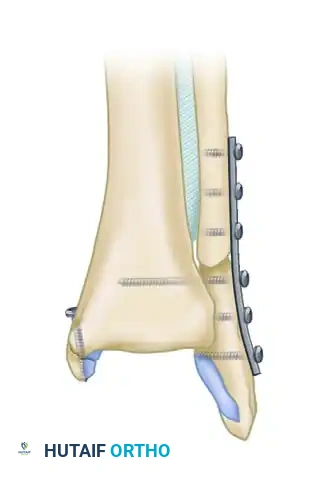
Once reduced, fixation is achieved based on fracture morphology. For standard oblique or spiral fractures (Danis-Weber B), a 3.5-mm cortical lag screw is placed perpendicular to the fracture plane to achieve interfragmentary compression. This is subsequently protected by a one-third tubular plate applied in a neutralization fashion on the lateral or posterolateral surface of the fibula. In highly selected, younger patients with simple oblique fractures and excellent bone quality, a lag screw-only technique utilizing two or three parallel screws may be employed to minimize soft tissue irritation. Conversely, in elderly patients with osteopenic bone, standard constructs frequently fail. In these scenarios, augmenting the plate fixation with an intramedullary Kirschner wire or utilizing anatomically contoured locking plates is highly recommended to increase the construct's resistance to bending and torsional forces.
Operative Techniques: Medial Malleolus
Following fibular fixation, attention is directed to the medial malleolus. A longitudinal or slightly curvilinear incision is made centered over the medial malleolus, curving anteriorly at its distal extent. The great saphenous vein and the accompanying saphenous nerve are carefully identified and retracted anteriorly. The fracture site is exposed, and it is imperative to inspect the tibiotalar joint space. Frequently, a flap of periosteum or a portion of the deltoid ligament is invaginated into the fracture site, precluding anatomic reduction. This interposed tissue must be meticulously extracted using a Freer elevator or a small sharp hook.
The medial malleolar fragment is reduced using a pointed reduction clamp, ensuring that the articular cartilage of the mortise is perfectly congruent. The choice of fixation is strictly dictated by the size, morphology, and comminution of the fragment.
1. Large Fragments:
Large, solid medial malleolar fragments are typically fixed with a single or double lag screw technique. Two 4.0-mm partially threaded cancellous screws are preferred to provide compression and control rotation. The screws are directed perpendicularly to the fracture line, typically aiming slightly anteriorly to avoid the posterior tibial tendon and the subtalar joint.
2. Small Fragments:
Smaller fragments present a risk of iatrogenic comminution if two screws are attempted. In these cases, the fragment can be securely fixed with one 4.0-mm partially threaded cancellous lag screw to provide compression, supplemented by one parallel Kirschner wire (K-wire) to prevent rotational displacement.
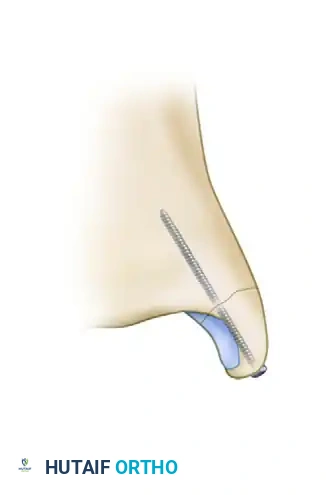
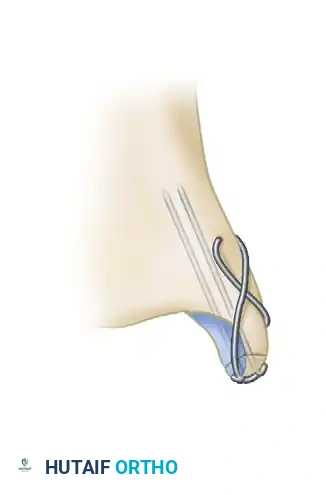
3. Comminuted or Very Small Fragments:
Fragments that are too small, severely osteopenic, or highly comminuted for standard screw fixation are best stabilized using a tension band wiring technique. This construct involves the placement of two parallel K-wires across the fracture site, followed by a figure-of-eight stainless steel wire. This biomechanically superior technique converts the tensile forces exerted by the deltoid ligament during ankle motion into dynamic compressive forces across the fracture site.
4. Vertical Fractures:
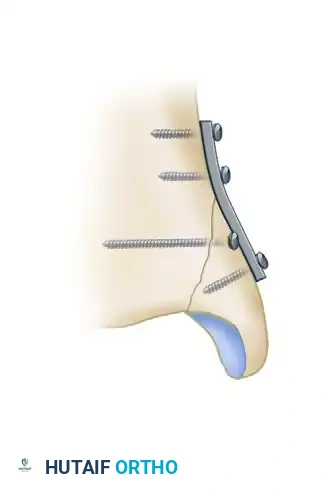
Vertical shear fractures of the medial malleolus, classically associated with Supination-Adduction (SAD) injuries, require a fundamentally different biomechanical approach. Standard vertically oriented screws will not provide adequate compression across a vertical fracture plane and may cause the fragment to slide proximally. These injuries require horizontally directed lag screws or, more effectively, antiglide plating techniques applied to the medial cortex.
Biomechanical studies by Dumigan et al. have unequivocally demonstrated that the fixation of vertical medial malleolar fractures with neutralization or antiglide plating is biomechanically advantageous. This construct provides superior resistance to vertical shear forces compared to screw fixation alone, ensuring maintenance of reduction during the critical early healing phase.
Following fixation of both malleoli, the syndesmosis must be rigorously evaluated using the external rotation stress test (the "Cotton test") under live fluoroscopy. If the medial clear space widens during external rotation stress, syndesmotic instability is present, and stabilization utilizing syndesmotic screws or dynamic suture button constructs is mandated.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the operative management of bimalleolar ankle fractures carries a recognized profile of complications. The delicate soft tissue envelope, the complex biomechanics of the ankle mortise, and the increasing prevalence of medical comorbidities in the trauma population all contribute to postoperative morbidity. A comprehensive understanding of these complications, their expected incidence, and appropriate salvage strategies is essential for the operating surgeon.
Wound complications are the most frequently encountered adverse events, particularly in patients with diabetes, peripheral vascular disease, or those who use tobacco. Superficial wound dehiscence or marginal necrosis can often be managed with local wound care and oral antibiotics. However, deep surgical site infections involving the osteosynthesis hardware represent a limb-threatening complication. Immediate aggressive surgical debridement, hardware retention (if the fracture is not yet united and the hardware remains stable), and targeted intravenous antibiotic therapy are required. If the hardware is loose or the infection is refractory, the implants must be removed, and the ankle may require stabilization via a spanning external fixator.
| Complication | Estimated Incidence Rate | Clinical Presentation and Salvage Management Strategy |
|---|---|---|
| Superficial Wound Infection / Dehiscence | 5% - 10% | Presents as erythema, delayed healing, or minor eschar. Managed with local wound care, oral antibiotics, and strict elevation. Rarely requires operative intervention. |
| Deep Surgical Site Infection | 1% - 3% (Higher in Diabetics) | Purulent drainage, severe pain, systemic signs. Requires emergent operative irrigation and debridement (I&D). Hardware retained if stable; removed and replaced with external fixation if loose. |
| Post-Traumatic Osteoarthritis | 10% - 40% (Depends on energy and reduction) | Chronic pain, stiffness, and radiographic joint space narrowing months to years post-op. Salvage includes activity modification, bracing, Total Ankle Arthroplasty (TAA), or Tibiotalar Arthrodesis. |
| Symptomatic Hardware Prominence | 15% - 30% | Localized pain and irritation over the medial or lateral malleolus, particularly with footwear. Managed conservatively with padding; definitive salvage is elective hardware removal after robust radiographic union (typically >1 year). |
| Nonunion / Delayed Union | 2% - 5% | Persistent pain at fracture site, lack of bridging callus on X-ray at 6 months. Salvage involves revision ORIF, bone grafting (autograft or orthobiologics), and potentially switching to stiffer constructs (locking plates). |
| Malunion / Syndesmotic Malreduction | 5% - 15% | Asymmetric clear spaces on X-ray, chronic instability, rapid cartilage wear. Requires complex reconstructive osteotomies, syndesmotic revision, or early arthrodesis if cartilage damage is already severe. |
| Complex Regional Pain Syndrome (CRPS) | 2% - 4% | Disproportionate pain, allodynia, skin color/temperature changes, profound stiffness. Requires immediate aggressive physical therapy, neuropathic pain modulators (gabapentin), and sympathetic nerve blocks. |
Post-traumatic osteoarthritis is the most devastating long-term complication, directly correlating with the initial energy of the injury, the presence of articular comminution, and the precision of the surgical reduction. Even with perfect anatomic restoration, the initial impact of the talus against the tibial plafond causes irreversible chondrocyte apoptosis. Patients must be counseled preoperatively regarding this risk. When conservative measures fail, salvage options include ankle arthrodesis, which provides excellent pain relief at the cost of joint mobility, or total ankle arthroplasty in appropriately selected, lower-demand patients.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation of bimalleolar ankle fractures is a delicate balance between protecting the surgical osteosynthesis and preventing the profound joint stiffness and muscle atrophy that accompany prolonged immobilization. The protocol must be strictly tailored to the rigidity of the fixation achieved intraoperatively, the patient's bone quality, and their compliance capacity.
Phase I: Maximum Protection and Edema Control (Weeks 0-2)
Immediately following surgery, the ankle is immobilized in a bulky, well-padded Jones dressing reinforced with a posterior plaster splint. The ankle is positioned in neutral dorsiflexion to prevent Achilles tendon contracture. The patient is made strictly non-weight-bearing (NWB) on the operative extremity. The paramount goals of this phase are wound healing, hematoma organization, and aggressive edema control. The patient is instructed to elevate the limb strictly above the level of the heart for 23 hours a day. Pain is managed with a multimodal analgesic regimen.
Phase II: Early Mobilization and Soft Tissue Maturation (Weeks 2-6)
At the two-week postoperative mark, the initial splint is removed, and the surgical incisions are meticulously inspected. Sutures or staples are removed if the wound is fully epithelialized. If the intraoperative fixation was deemed rigid and the bone quality is adequate, the patient is transitioned into a removable controlled ankle motion (CAM) boot. This marks a critical transition: the patient is instructed to remove the boot multiple times daily to initiate early active range of motion (AROM) exercises, focusing on pure sagittal plane dorsiflexion and plantarflexion. Inversion and eversion are strictly prohibited to protect the malleolar fixation. Weight-bearing status generally remains NWB, although some modern protocols permit touch-down weight-bearing (TDWB) to stimulate proprioception, strictly at the surgeon's discretion.
Phase III: Progressive Weight-Bearing and Strengthening (Weeks 6-12)
At six weeks, orthogonal radiographs are obtained to assess for early bridging callus and maintenance of the mortise reduction. Upon radiographic confirmation of early clinical union, the patient begins a progressive weight-bearing protocol. This typically advances from 25% partial weight-bearing to full weight-bearing in the CAM boot over a period of 2 to 4 weeks. Formal physical therapy is initiated. The rehabilitation focus shifts to restoring full active and passive range of motion, initiating isometric and isotonic strengthening of the peroneal and posterior tibial musculature, and aggressive proprioceptive retraining using balance boards. Achilles tendon stretching is emphasized to normalize gait mechanics.
Phase IV: Return to Function and Advanced Rehabilitation (Weeks 12+)
By 12 weeks, most patients demonstrate robust radiographic union and are transitioned out of the CAM boot into a supportive athletic shoe, often utilizing an ankle lacer brace for transitional support. Physical therapy advances to sport-specific or occupation-specific training, including plyometrics, dynamic cutting maneuvers, and endurance training. Patients must be counseled that maximal medical improvement following a bimalleolar ankle fracture frequently requires 12 to 18 months, and residual mild swelling or stiffness after vigorous activity is an expected long-term sequela.
Summary of Landmark Literature and Clinical Guidelines
The contemporary surgical management of bimalleolar ankle fractures is firmly rooted in decades of rigorous biomechanical research and clinical outcomes studies. A thorough command of this landmark literature is essential for the academic orthopedic surgeon.
The most frequently cited biomechanical foundation for anatomic reduction remains the work of Ramsey and Hamilton (1976). Their cadaveric study quantitatively demonstrated the catastrophic effect of lateral talar shift, proving that a 1 mm displacement reduces tibiotalar contact area by 42%. This single study forms the absolute justification for the aggressive operative management of displaced ankle mortise injuries.
The Lauge-Hansen Classification (1950) remains the definitive framework for understanding the pathomechanics of ankle fractures. By categorizing injuries based on foot position (Supination vs. Pronation) and the direction of the deforming force (Adduction, External Rotation, Abduction), Lauge-Hansen provided surgeons with a predictive model for soft tissue injury and a roadmap for reversing the mechanism of injury during closed or open reduction.
Regarding surgical timing, the work of Carr et al. and subsequent meta-analyses have codified the "early versus late" paradigm. These studies validate that ORIF performed within the first 24 hours yields equivalent long-term functional outcomes to delayed surgery, but significantly reduces hospital length of stay and early postoperative pain. Conversely, operating during the peak inflammatory phase (days 2-7) is universally condemned in the literature due to unacceptably high rates of wound necrosis and deep infection.
The biomechanical superiority of specific fixation constructs has been extensively validated. Dumigan et al. provided the definitive evidence that vertical shear fractures of the medial malleolus (SAD injuries) are inadequately stabilized by standard lag screws, mandating the use of antiglide plating to resist shear forces. Similarly, the use of intramedullary augmentation for osteopenic fibular fractures has been supported by numerous clinical series demonstrating a marked reduction in hardware failure rates among the elderly population.
In conclusion, the successful management of bimalleolar ankle fractures requires the surgeon to seamlessly integrate profound anatomical knowledge, respect for the Lauge-Hansen pathomechanics, and meticulous surgical execution. By adhering to these established biomechanical principles and evidence-based protocols, the orthopedic surgeon can reliably restore the complex kinematics of the ankle mortise, thereby preserving joint longevity and restoring optimal function to the patient.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons in surgical preparation and board reviews (AAOS, FRCS, Arab Board).

Chapter Index
- Comprehensive Introduction and Patho-Epidemiology
- Detailed Surgical Anatomy and Biomechanics
- Exhaustive Indications and Contraindications
- Pre-Operative Planning, Templating, and Patient Positioning
- Step-by-Step Surgical Approach and Fixation Technique
- Complications, Incidence Rates, and Salvage Management
- Phased Post-Operative Rehabilitation Protocols
- Summary of Landmark Literature and Clinical Guidelines
Back to Master Guide