Bone Grafting of Medial Malleolar Nonunion and Partial Fibulectomy: A Comprehensive Surgical Guide

Key Takeaway
Medial malleolar nonunions present significant biomechanical challenges, often requiring meticulous bone grafting and rigid internal fixation. This comprehensive surgical guide details the Banks technique for wedge-shaped cancellous grafting, alongside the strategic use of partial fibulectomy to promote tibial union. By mastering these evidence-based approaches, orthopedic surgeons can effectively restore ankle joint congruity, optimize axial loading, and achieve successful clinical outcomes in complex nonunion cases.
Comprehensive Introduction and Patho-Epidemiology
Nonunion of the medial malleolus and the tibial shaft represents a profound orthopedic challenge, fundamentally compromising the stability, congruity, and load-bearing capacity of the lower extremity. The medial malleolus serves as the primary osseous buttress against medial talar excursion and is the critical attachment epicenter for the robust deltoid ligament complex. When a fracture in this precise anatomical region fails to unite, the resultant persistent shear forces, exacerbated by the relentless intrusion of synovial fluid into the fracture gap, severely and chronically inhibit osteogenesis. This leads to the formation of a synovial pseudarthrosis, a recalcitrant biological environment that is highly resistant to conservative management and necessitates definitive surgical intervention.
The epidemiology of medial malleolar nonunions suggests an incidence rate ranging from 5% to 15% following both operatively and non-operatively managed ankle fractures. The risk is exponentially magnified in cases characterized by inadequate initial reduction, the interposition of periosteum or the posterior tibial tendon, or the use of inappropriate fixation constructs that fail to neutralize rotational and shear forces. Concurrently, tibial shaft fractures exhibit a nonunion rate of up to 10-12%, heavily influenced by the severity of the initial soft tissue injury, the degree of comminution, and the vascular integrity of the surrounding soft tissue envelope. The development of a nonunion in these areas is not merely a failure of bone healing but a complex cascade of mechanical instability and biological exhaustion.
In the context of the tibial shaft, the patho-epidemiology is further complicated by the biomechanical relationship between the tibia and the fibula. When both bones are fractured, the fibula, benefiting from a smaller cross-sectional area and a highly vascularized, robust muscular envelope, almost universally heals faster than the tibia. Once consolidated, this intact fibula transforms into a rigid, load-bearing strut. This strut effect fundamentally alters the strain environment of the healing tibia, shielding it from the physiological axial loads necessary to stimulate secondary bone healing via Wolff’s Law. The deprivation of cyclic micromotion and axial compression drives the tibial fracture site toward fibrous tissue interposition rather than robust callus formation.
Surgical intervention is definitively indicated for symptomatic nonunions, progressive valgus or varus deformities, or impending post-traumatic osteoarthritis. The primary objectives of operative management are multifaceted: the complete eradication of the fibrous pseudarthrosis, the restoration of vital osteoinductive and osteoconductive properties through meticulous autologous bone grafting, and the achievement of absolute mechanical stability via rigid internal fixation. This comprehensive masterclass details the highly effective Banks technique for bone grafting medial malleolar nonunions, advanced biological augmentation strategies, and the critical, biomechanically sound role of partial fibulectomy in managing concurrent tibial shaft nonunions.
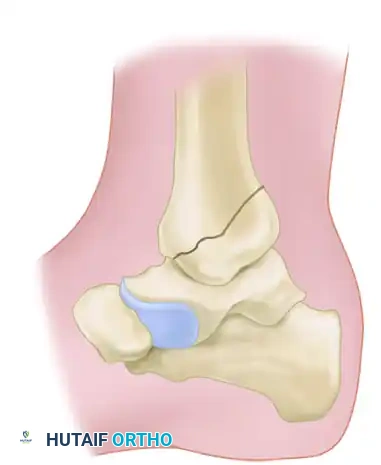
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy of the medial ankle and the lower leg is an absolute prerequisite for executing these complex reconstructive procedures safely and effectively. The medial malleolus is the distal continuation of the medial tibial cortex, forming the medial articular facet of the ankle mortise. It is intimately associated with the deltoid ligament, a multifascicular structure comprising superficial and deep layers. The deep deltoid ligament is the primary stabilizer against lateral talar shift and external rotation. Preservation of the deltoid ligament's attachment to the nonunion fragment is paramount; devascularization or iatrogenic detachment during surgical exposure will precipitate catastrophic ankle instability and further compromise the fragment's precarious blood supply.
The vascular anatomy of the medial malleolus is primarily supplied by the anterior medial malleolar artery (a branch of the anterior tibial artery) and the posterior medial malleolar artery (a branch of the posterior tibial artery). These vessels form an intricate anastomotic network over the medial malleolus. In a nonunion scenario, this vascular network is often disrupted or encased in dense, avascular scar tissue. The surgical approach must therefore be meticulously planned to elevate full-thickness fascioperiosteal flaps, preserving the microvascular supply to the bone fragments. Furthermore, the great saphenous vein and the saphenous nerve course anterior to the medial malleolus; iatrogenic injury to these structures can result in debilitating neuromas and compromised venous return, significantly complicating postoperative recovery.
Biomechanically, the talocrural joint is a highly constrained, congruent articulation that tolerates incredibly high peak loads—often exceeding five times body weight during normal ambulation. Classic biomechanical studies by Ramsey and Hamilton demonstrated that a mere 1 millimeter of lateral talar shift results in a staggering 42% decrease in tibiotalar contact area. This exponential increase in peak contact stresses rapidly accelerates the degeneration of articular cartilage, culminating in severe post-traumatic osteoarthritis. The medial malleolus is the critical impediment to this lateral shift. A nonunion here allows dynamic instability, where the talus subluxates laterally under cyclical loading, creating a persistent shear environment at the fracture site that entirely precludes osteoblast bridging.
Regarding the tibial-fibular complex, the biomechanics are governed by principles of load sharing and dynamic compression. In a healthy limb, the fibula transmits approximately 15% to 17% of the axial load applied to the lower extremity. However, in the presence of a tibial nonunion with a healed or intact fibula, the fibula assumes a disproportionate amount of this load. This creates a "strut effect," effectively holding the tibial fragments apart and preventing the interfragmentary compression required for primary or secondary bone healing. Destabilizing this strut through a strategically executed partial fibulectomy alters the biomechanical environment, re-establishing the tibia as the primary load-bearing column and allowing physiological axial forces to compress the nonunion site, thereby catalyzing osteogenesis.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for a medial malleolar nonunion or to perform a partial fibulectomy for a tibial nonunion requires a nuanced understanding of patient-specific factors, radiographic parameters, and the underlying biological environment. Careful patient selection is the cornerstone of surgical success.
| Parameter | Indications | Contraindications |
|---|---|---|
| Medial Malleolar Nonunion (Banks Technique) | - Symptomatic nonunion > 6 months post-injury. - Radiographic evidence of pseudarthrosis. - Dynamic lateral talar shift on stress views. - Medial-sided ankle pain with weight-bearing. - Impending post-traumatic osteoarthritis. |
- Absolute: Active deep infection of the ankle joint. - Absolute: Charcot neuroarthropathy (requires different reconstructive principles). - Relative: Severe, end-stage tibiotalar osteoarthritis (may require arthrodesis instead). - Relative: Critical limb ischemia or severe peripheral vascular disease. - Relative: Fragment too small/comminuted to accept a 4.5mm lag screw. |
| Partial Fibulectomy (for Tibial Nonunion) | - Aseptic tibial shaft nonunion with an intact/healed fibula. - Delayed union of the tibia where the fibula is preventing compression. - Minor angular deformities (varus/valgus) correctable by closed manipulation after fibular release. - Need to stimulate osteogenesis without opening the primary tibial fracture site. |
- Absolute: Synovial pseudarthrosis of the tibia (requires open debridement and grafting). - Absolute: Gap nonunion of the tibia > 1 cm (requires structural grafting/bone transport). - Absolute: Active osteomyelitis of the tibia (requires staged management). - Relative: Severe osteopenia where the fibula is the only stable strut preventing massive collapse. - Relative: Non-compliant patient unable to follow weight-bearing protocols. |
Indications for the Banks technique are primarily driven by the presence of persistent pain and mechanical instability. Patients typically present with a chronic limp, localized swelling, and an inability to return to pre-injury activity levels. Radiographically, the presence of sclerotic fracture margins, a persistent radiolucent gap, and the absence of bridging trabeculae at least six months post-injury confirm the diagnosis. The procedure is highly indicated when the articular cartilage of the ankle mortise is relatively preserved, as the Banks technique is fundamentally a joint-sparing, restorative operation.
Conversely, contraindications must be strictly respected to avoid catastrophic failures. Active deep infection is an absolute contraindication to immediate internal fixation and autologous bone grafting; such cases require aggressive debridement, removal of hardware, and the implementation of staged protocols such as the Masquelet technique. Severe peripheral vascular disease or uncontrolled diabetes mellitus with profound neuropathy (Charcot arthropathy) significantly increases the risk of wound dehiscence, deep infection, and failure of fixation. In cases where the medial malleolar fragment is severely comminuted or osteoporotic, achieving rigid interfragmentary compression with a lag screw may be impossible, necessitating alternative strategies such as tension band wiring or primary tibiotalar arthrodesis.
For partial fibulectomy, the ideal candidate has an oligotrophic or hypertrophic tibial nonunion where the biological capacity for healing is present, but the mechanical environment is inhibitory due to the intact fibula. It is contraindicated in atrophic nonunions with massive bone loss or true synovial pseudarthroses, as these conditions lack the necessary biological substrate (osteoprogenitor cells and vascularity) to heal simply by restoring axial compression. In these complex scenarios, open debridement, rigid stabilization (often with intramedullary nailing or circular external fixation), and massive biological augmentation are mandated.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock of complex nonunion surgery. The clinical evaluation must go beyond the localized injury to assess the entire lower extremity axis, soft tissue envelope, and neurovascular status. The surgeon must evaluate the quality of the skin over the medial malleolus and the anterior tibia, noting any previous surgical incisions, skin grafts, or areas of compromised vascularity that could dictate the surgical approach. A comprehensive assessment of the patient's nutritional status (albumin, prealbumin, Vitamin D levels) and optimization of medical comorbidities (glycemic control, smoking cessation) are critical steps in the preoperative phase to maximize the biological potential for bone healing.
Radiographic assessment demands a standardized, high-quality imaging protocol. Standard weight-bearing anteroposterior (AP), lateral, and mortise radiographs of the ankle and full-length orthogonal views of the tibia and fibula are mandatory. A nonunion is radiographically defined by the persistence of a radiolucent fracture line, sclerotic fracture margins, and the absence of bridging trabeculae. Preoperative computed tomography (CT) is highly recommended and considered the gold standard for nonunion evaluation. A CT scan with fine sagittal and coronal reformats provides a three-dimensional understanding of the nonunion morphology, the exact volumetric size of the distal fragment, and the presence of any intra-articular step-off or subchondral cystic changes. This high-resolution imaging is critical for preoperative templating, allowing the surgeon to precisely map the trajectory of the lag screws and calculate the volume of cancellous graft required.
Templating is an active process that involves superimposing digital templates over the preoperative radiographs. For the Banks technique, the surgeon must determine the optimal entry point and trajectory for the 4.5 mm partially threaded cancellous lag screw to ensure it engages the dense metaphyseal bone of the distal tibia without breaching the articular surface. For the partial fibulectomy, the exact level of the fibular resection must be planned. The resection is typically performed at the middle to distal third junction, ensuring it is distant from the common peroneal nerve proximally and the syndesmosis distally. The templated resection length must be a minimum of 2.5 cm to prevent premature re-union of the fibula.
Positioning and anesthesia are coordinated to optimize surgical exposure and patient safety. The patient is placed in the supine position on a fully radiolucent operating table to facilitate unimpeded fluoroscopic imaging in multiple planes. General anesthesia or a robust regional block (spinal or epidural) is administered. A well-padded thigh tourniquet is applied to ensure a bloodless surgical field, which is essential for identifying the avascular fibrous tissue and protecting delicate neurovascular structures. A bump may be placed under the ipsilateral hip to correct natural external rotation, bringing the medial malleolus and the anterior tibia into a neutral, easily accessible position. The ipsilateral iliac crest should also be prepped and draped in the surgical field in the event that a larger volume of structural bone graft is required unexpectedly.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the Banks technique and partial fibulectomy demands precision, respect for soft tissues, and a deep understanding of osteosynthesis principles. The following steps detail the operative sequence for addressing a medial malleolar nonunion augmented with autologous graft.
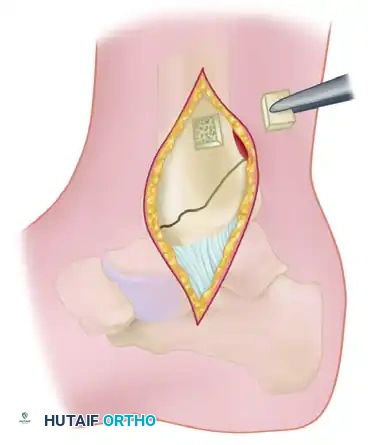
Surgical Approach and Exposure
A medial longitudinal incision, approximately 10 cm in length, is made centered precisely over the medial malleolus.
Careful subcutaneous dissection is performed to identify, mobilize, and protect the great saphenous vein and the saphenous nerve, which typically course anterior to the medial malleolus. Retraction of these structures must be gentle to prevent neurapraxia. The incision is carried down sharply through the periosteum. Full-thickness fascioperiosteal flaps are elevated using a Cobb elevator to expose the nonunion site, taking immense care not to strip the deltoid ligament from the distal fragment, as this would completely devascularize the bone.
Preparation of the Nonunion Site
The fibrous pseudarthrosis tissue interposed between the fracture fragments is meticulously excised using a combination of small curettes, a surgical scalpel, and a pituitary rongeur.

Once the nonunion is thoroughly debrided of all soft tissue, the sclerotic, avascular bone ends must be freshened to expose healthy, bleeding bone (the "paprika sign"). Using a sharp, narrow osteotome or a high-speed burr under continuous saline irrigation, bone is removed to create a distinct wedge-shaped defect.
The apex of this wedge must be directed precisely toward the articular surface of the ankle joint. It is absolutely imperative that damage to the articular cartilage is minimized or completely avoided. Preserving the articular hinge maintains joint congruity while allowing access for the graft.
Harvesting the Cancellous Bone Graft
To obtain the necessary autologous graft, a cortical window is created in the tibial metaphysis at the proximal extent of the surgical wound.
Using a thin osteotome or an oscillating saw, a square piece of cortical bone (approximately 1.5 x 1.5 cm) is carefully removed. The edges of this cortical window should be undercut. This crucial technique allows the cortical piece to be securely replaced later, acting like a "manhole cover" that will not fall into the medullary canal. Through this metaphyseal window, a curette is used to harvest a generous volume of rich, osteoprogenitor-laden cancellous bone from the distal tibial metaphysis.
Reduction, Fixation, and Grafting
The medial malleolar fragment is meticulously restored to its anatomical position, ensuring perfect restoration of the articular mortise under direct vision and fluoroscopic guidance. It is held gently but securely with a pointed reduction forceps (towel clip).

The wedge-shaped defect at the nonunion site is then densely packed with the harvested cancellous bone. The osteoinductive and osteoconductive properties of this autograft are essential for bridging the pseudarthrosis gap. Once the graft is firmly packed, the fragment is rigidly fixed. A 4.5 mm partially threaded cancellous lag screw (typically 4.0 to 5.0 cm in length) is inserted from the tip of the medial malleolus. The trajectory is directed proximally and slightly laterally into the dense metaphyseal bone of the tibia, achieving robust interfragmentary compression across the grafted nonunion site. Anti-rotation stability can be augmented with a parallel 2.0 mm Kirschner wire or a smaller 3.5 mm screw if the fragment size permits.
Partial Fibulectomy for Tibial Nonunion
When a concurrent tibial nonunion is present and driven by the strut effect of the fibula, a partial fibulectomy is performed.

Preoperative radiograph demonstrating a recalcitrant nonunion. The intact fibula is preventing axial compression of the tibia.

Radiograph showing failure to produce union by a sliding inlay graft. Note that the fibula remains intact, acting as a load-bearing strut and preventing tibial apposition.
A lateral approach is utilized over the middle to distal third of the fibula, meticulously avoiding the superficial peroneal nerve. The periosteum is incised and elevated circumferentially. Using an oscillating saw, a full-thickness segment of the fibula is resected. The resected segment must be precisely 2.5 cm long. Removal of a smaller segment is a catastrophic technical error; it allows the fibula to rapidly heal before the tibia has achieved solid union, immediately recreating the pathological strut effect.
Immediately following the fibular resection, the tibia must be carefully aligned by closed manipulation. Because the lateral buttress has been removed, there is a distinct risk of the tibia collapsing into a varus deformity.

Four years after the application of dual onlay grafts and osteotomy of the fibula. Note that the fibula now overlaps, allowing the tibia to compress and heal.

Final radiographic follow-up demonstrating solid union of the tibial shaft following successful fibular release and grafting.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the management of nonunions is fraught with potential complications. The compromised biological envelope and the chronicity of the condition inherently elevate the risk profile compared to acute fracture fixation. Surgeons must be hyper-vigilant in identifying early signs of failure and possess a robust armamentarium for salvage management.
| Complication | Estimated Incidence | Salvage Management Strategy |
|---|---|---|
| Superficial/Deep Infection | 3% - 8% | Superficial: Aggressive oral/IV antibiotics, local wound care. Deep: Immediate operative irrigation and debridement, hardware removal if loose, placement of antibiotic-impregnated PMMA spacer (Masquelet Stage 1), and culture-directed IV antibiotics. |
| Persistent Nonunion / Hardware Failure | 5% - 10% | Revision osteosynthesis. For medial malleolus: consider tension band wiring or primary tibiotalar arthrodesis if bone stock is depleted. For tibia: re-reaming and exchange nailing to a larger diameter nail, or application of a fine-wire circular external fixator (Ilizarov/Taylor Spatial Frame) with compression. |
| Varus Collapse (Post-Fibulectomy) | 4% - 7% | Requires immediate correction. If recognized early in a cast, wedging the cast may suffice. If rigid or progressive, requires operative intervention with intramedullary nailing or external fixation of the tibia to restore and maintain mechanical alignment. |
| Nerve Injury (Saphenous / Superficial Peroneal) | 2% - 5% | Mostly transient neurapraxia resolving with observation and gabapentinoids. If a neuroma forms and is recalcitrant to conservative care, surgical exploration, neuroma excision, and targeted muscle reinnervation (TMR) or burying the nerve end into deep muscle/bone is indicated. |
Infection is arguably the most devastating complication, particularly in the presence of internal hardware and avascular bone. The incidence is higher in patients with medical comorbidities such as diabetes or a history of smoking. If a deep infection occurs, the principles of the induced membrane (Masquelet) technique become paramount. The first stage involves radical debridement of all infected and necrotic bone, removal of hardware, and the insertion of an antibiotic-impregnated polymethylmethacrylate (PMMA) spacer. This spacer sterilizes the local environment and induces a highly vascularized pseudosynovial membrane. After 6 to 8 weeks, the second stage involves removing the spacer and filling the void with massive amounts of autograft (often harvested via the Reamer-Irrigator-Aspirator [RIA] technique) and rigid restabilization.
Hardware failure and persistent nonunion typically result from inadequate initial debridement of the pseudarthrosis, insufficient interfragmentary compression, or premature weight-bearing. If the medial malleolar lag screw pulls out or breaks, the joint becomes dynamically unstable. Salvage in this scenario depends heavily on the remaining bone stock. If sufficient bone exists, revision with a larger diameter screw or a tension band construct is attempted. If the fragment is severely comminuted or avascular necrosis has set in, a primary tibiotalar arthrodesis is often the most reliable method to provide a painless, stable, plantigrade foot.
Varus collapse following a partial fibulectomy is a direct biomechanical consequence of removing the lateral stabilizing strut. The tibia, particularly if the nonunion is in the distal third, has a natural tendency to fall into varus under axial load. This highlights the critical importance of meticulous postoperative casting and close radiographic monitoring. If varus collapse occurs and exceeds acceptable parameters (typically > 5 degrees), it must be aggressively managed. Closed wedging of the cast can be attempted in the early phases. However, if the deformity is progressive, operative stabilization of the tibia—usually via intramedullary nailing—is required to physically hold the mechanical axis while allowing axial compression.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is as critical to the success of the procedure as the surgical execution itself. The protocol must be meticulously phased, balancing the biomechanical need to protect the fragile initial osteosynthesis with the biological requirement for progressive mechanical loading to stimulate osteogenesis. The rehabilitation strategy differs significantly depending on whether the patient underwent an isolated medial malleolar grafting or a partial fibulectomy for a tibial nonunion.
For the isolated medial malleolar bone grafting (Banks technique), Phase 1 (Maximum Protection) spans from weeks 0 to 6. Immediately postoperatively, the ankle is immobilized in a well-padded short-leg cast or a rigid posterior splint in neutral dorsiflexion. The patient is instructed to remain strictly non-weight-bearing. This absolute offloading is critical to prevent shear forces across the articular surface from displacing the grafted fragment or causing pull-out of the lag screw before the cancellous graft has begun to incorporate. Elevation and strict edema control are emphasized to protect the vulnerable medial soft tissue envelope.
Phase 2 (Controlled Loading) for the medial malleolus begins at 6 weeks, contingent upon radiographic evidence of early graft incorporation and the absence of hardware complication. The patient is transitioned to a controlled ankle motion (CAM) boot. Progressive partial weight-bearing is initiated, starting at 25% of body weight and increasing gradually. Concurrently, active and active-assisted range-of-motion (ROM) exercises for the ankle and subtalar joints are commenced to prevent arthrofibrosis and restore the gliding mechanics of the flexor tendons. Phase 3 (Return to Function), starting around 10 to 12 weeks, involves weaning from the CAM boot, initiating proprioceptive training, and progressive strengthening of the gastroc-soleus and anterior compartment musculature.
Conversely, the postoperative protocol for partial fibulectomy relies heavily on immediate, controlled mechanical loading. Phase 1 involves the application of a straight, well-molded long-leg walking cast immediately postoperatively. The purpose of this cast is not to offload the limb, but to control angular alignment and strictly prevent the varus collapse that the tibia is prone to after the lateral fibular buttress is removed. Full weight-bearing is strongly encouraged immediately as tolerated by the patient. The cyclic axial load generated during ambulation is the primary mechanical catalyst for osteogenesis at the tibial nonunion site, directly adhering to Wolff’s Law.
The long-leg cast is typically maintained for 4 to 6 weeks, followed by a transition to a functional fracture brace (Sarmiento brace) or a short-leg cast, depending on the level of the tibial nonunion and the stability achieved. Radiographs are obtained at 2-week intervals initially to monitor alignment and ensure no progressive varus deformity is occurring. Once bridging callus is definitively observed across the tibial nonunion site, the brace is discontinued, and aggressive physical therapy focuses on restoring knee and ankle kinematics, normalizing gait mechanics, and rebuilding the atrophied lower extremity musculature.
Summary of Landmark Literature and Clinical Guidelines
The surgical strategies detailed in this masterclass are deeply rooted in decades of rigorous biomechanical research and clinical outcome studies. A thorough understanding of this landmark literature is essential for the academic orthopedic surgeon to justify surgical decision-making and adhere to evidence-based clinical guidelines.
The biomechanical imperative for anatomical restoration of the medial malleolus was established by the seminal work of Ramsey and Hamilton in 1976. Their highly cited cadaveric study demonstrated that a 1 mm lateral shift of the talus results in a 42% reduction in tibiotalar contact area. This singular finding fundamentally shifted the orthopedic paradigm toward aggressive, rigid internal fixation of the ankle mortise, underscoring why a medial malleolar nonunion—which inherently allows dynamic lateral talar shift—is a catastrophic precursor to post-traumatic osteoarthritis and mandates surgical correction.
The specific technique of joint-sparing, wedge-defect cancellous bone grafting for medial malleolar nonunions was popularized by Banks. His original descriptions highlighted the biological necessity of removing the avascular pseudarthrosis while maintaining the articular hinge to preserve joint congruity. Modern clinical guidelines from the Orthopaedic Trauma Association (OTA) and the American Academy of Orthopaedic Surgeons (AAOS) continue to support autologous cancellous bone grafting from the proximal tibia or iliac crest, combined with rigid lag screw fixation, as the gold standard for symptomatic, aseptic medial malleolar nonunions.
Regarding the management of tibial nonunions, the inhibitory "strut effect" of the intact fibula was comprehensively described by Sørensen. His clinical series demonstrated that destabilizing the fibula allows the dynamic axial compression necessary to convert an oligotrophic or hypertrophic nonunion into a healing fracture. Current guidelines emphasize that partial fibulectomy is a highly effective, low-morbidity procedure, achieving union rates exceeding 75% when utilized correctly. However, modern literature also heavily caveats this technique, stressing that it must be combined with strict postoperative weight-bearing protocols and is contraindicated in true atrophic or synovial pseudarthroses, where advanced biological augmentation (such as the Masquelet technique or the use of Reamer-Irrigator-Aspirator [RIA] autograft combined with rh-BMP2) remains the definitive standard of care.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons in surgical preparation and board reviews (AAOS, FRCS, Arab Board).
