Minimally Invasive Plating of Tibial Pilon Fractures: A Master Surgical Guide

Key Takeaway
Minimally invasive plate osteosynthesis (MIPO) for tibial pilon fractures is a highly effective, tissue-sparing technique. By utilizing a staged protocol—initial spanning external fixation followed by delayed definitive percutaneous plating—surgeons can mitigate severe soft tissue complications. This guide details the biomechanics, surgical approaches, and step-by-step execution of MIPO, ensuring anatomic articular reduction and stable diaphyseal fixation while preserving the critical extraperiosteal vascular envelope.
Comprehensive Introduction and Patho-Epidemiology
The management of tibial pilon fractures, designated as AO/OTA type 43 injuries, remains one of the most formidable and unforgiving challenges in contemporary orthopedic trauma surgery. These fractures, involving the weight-bearing articular surface of the distal tibia (the plafond) and the critical metaphyseal-diaphyseal junction, are historically notorious for precipitating devastating complications. Early attempts at managing high-energy pilon fractures through traditional, single-stage open reduction and internal fixation (ORIF) utilizing extensile approaches yielded catastrophic rates of wound dehiscence, deep infection, and subsequent osteomyelitis. These dismal outcomes were primarily driven by a failure to respect the tenuous, highly vulnerable soft tissue envelope surrounding the distal tibia, which lacks robust muscular coverage and relies on a fragile subdermal vascular plexus.

The patho-anatomy of a tibial pilon fracture is dictated by the mechanism of injury and the position of the foot at the time of impact. High-energy axial loads, classically sustained during motor vehicle collisions or falls from significant heights, drive the talus into the distal tibia like a wedge. This imparts massive compressive forces that shatter the articular surface, frequently creating a central "die-punch" fragment, highly comminuted metaphyseal zones, and severe, instantaneous disruption of the surrounding soft tissues. Conversely, low-energy rotational mechanisms, often seen in skiing or athletic injuries, tend to produce less comminution and are characterized by spiral fracture patterns with larger, more discrete articular fragments. Regardless of the energy imparted, the fundamental challenge remains the same: the surgeon must achieve anatomic restoration of the articular congruity while preserving the extraosseous vascular supply essential for metaphyseal fracture healing.
In response to the historical failures of extensile ORIF, Minimally Invasive Plate Osteosynthesis (MIPO) has evolved into the gold-standard paradigm for the definitive management of these complex fractures. MIPO represents a profound philosophical shift from mechanical dominance to biological preservation. Driven by the widespread development of precontoured, anatomically specific locking-plate technology, modern MIPO techniques allow surgeons to bridge zones of severe comminution without the need for extensive soft tissue stripping. Specialized instrumentation, including radiolucent targeting guides and outriggers, facilitates precise percutaneous proximal fixation, minimizing iatrogenic trauma to the already compromised limb.
Epidemiologically, tibial pilon fractures account for approximately 1% to 10% of all lower extremity fractures and 3% to 10% of all tibial fractures. They predominantly affect young, active males in their third to fifth decades of life, though a secondary bimodal peak is observed in elderly osteoporotic females sustaining low-energy falls. The socioeconomic burden of these injuries is immense, as patients frequently endure prolonged periods of disability, require extensive rehabilitation, and face a high likelihood of developing post-traumatic osteoarthritis regardless of the quality of the surgical reduction. Consequently, mastering the MIPO technique is not merely an academic exercise, but a clinical imperative for the modern orthopedic traumatologist seeking to optimize functional outcomes in this challenging patient population.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the complex three-dimensional osseous anatomy and the fragile soft tissue envelope of the distal leg is the cornerstone of successful MIPO in tibial pilon fractures. The distal tibia flares out to form the metaphyseal region, terminating in the articular plafond, which is concave in both the sagittal and coronal planes. The articular surface is anatomically divided into three primary columns or fragments: the medial malleolus, the anterolateral (Chaput) fragment, and the posterolateral (Volkmann) fragment. The central portion of the plafond is particularly susceptible to impaction, creating the classic "die-punch" fragment that is devoid of soft tissue attachments and must be elevated and bone-grafted to restore joint congruity. The fibula, which is fractured in approximately 75% to 85% of pilon injuries, acts as a critical lateral buttress; its anatomic restoration is frequently the first step in reestablishing the length and rotational alignment of the entire lower leg.
The soft tissue envelope of the distal tibia is notoriously unforgiving. Unlike the proximal tibia, which is enveloped by robust muscle bellies, the distal third of the tibia is covered only by skin, subcutaneous fat, and paratenon. The arterial supply to this region is predicated on a delicate extraosseous anastomotic network derived from the anterior tibial, posterior tibial, and peroneal arteries. The anterior skin, in particular, is supplied by the anterior tibial artery via small, easily disrupted perforators. Traditional extensile approaches devascularize significant expanses of cortical bone and destroy these perforators, leading to ischemic necrosis of the skin flaps. MIPO techniques are explicitly designed to respect these angiosomes by utilizing small, strategic incisions and extraperiosteal tunneling, thereby preserving the vital periosteal and subdermal blood supply necessary to ward off infection and promote fracture union.
Neurologically, the surgeon must be acutely aware of several critical structures during percutaneous plate insertion. Medially, the saphenous nerve and the great saphenous vein course anterior to the medial malleolus and are highly vulnerable during the creation of an anteromedial extraperiosteal tunnel. Laterally and anteriorly, the superficial peroneal nerve traverses the deep fascia to become subcutaneous in the distal third of the leg, while the deep peroneal nerve and the anterior tibial artery lie deep to the extensor hallucis longus (EHL) tendon. Meticulous blunt dissection and the use of tissue protectors are mandatory to avoid catastrophic iatrogenic nerve injuries, which can result in debilitating neuromas or complex regional pain syndrome (CRPS).
Biomechanically, the MIPO approach to pilon fractures is governed by Perren’s strain theory, employing a dual philosophy of stability. The articular block requires absolute stability to facilitate primary bone healing without callus formation, which is achieved through precise anatomic reduction and interfragmentary compression using lag screws. In stark contrast, the highly comminuted metaphyseal-diaphyseal segment requires relative stability. By utilizing a long bridging locking plate, the surgeon creates a flexible construct that allows for controlled micromotion at the fracture site. This micromotion maintains interfragmentary strain within the optimal window (between 2% and 10%), thereby stimulating robust secondary bone healing via endochondral ossification and exuberant callus formation. The use of locking screws enhances the pull-out strength of the construct, particularly in osteoporotic bone, and functions as an internal fixator that does not require compression against the periosteum, further preserving cortical perfusion.
Exhaustive Indications and Contraindications
The decision to employ MIPO for a tibial pilon fracture requires a nuanced assessment of the fracture morphology, the degree of soft tissue compromise, and the physiological status of the patient. MIPO is not a panacea; it is a highly specific technique that must be applied to the correct clinical scenario to yield optimal results. The primary indication for MIPO is a high-energy AO/OTA 43-B or 43-C fracture characterized by significant metaphyseal comminution where traditional ORIF would necessitate unacceptable soft tissue stripping. It is particularly advantageous in patients with compromised healing potential, such as diabetics, chronic smokers, or those with peripheral vascular disease, where minimizing surgical trauma to the soft tissues is of paramount importance.
However, the indications for MIPO must be balanced against absolute and relative contraindications. MIPO is contraindicated in cases of severe, unrecoverable soft tissue destruction, such as high-grade open fractures (Gustilo-Anderson IIIB or IIIC) with massive degloving, where primary amputation or definitive circular external fixation (e.g., Ilizarov or Taylor Spatial Frame) may be more appropriate. Furthermore, if the articular comminution is so profound that percutaneous or limited-open reduction cannot reliably restore joint congruity, the surgeon may be forced to utilize an extensile approach once the soft tissues have healed, or opt for a primary arthrodesis in highly selected, severely damaged elderly patients.
The timing of the intervention is equally critical. MIPO is almost never indicated as an acute, day-of-injury procedure for high-energy pilon fractures. The presence of profound edema, fracture blisters (both clear and blood-filled), and ecchymosis indicates that the soft tissue envelope is under extreme physiological stress. Operating through this compromised tissue invariably leads to wound breakdown. Therefore, the presence of these signs is an absolute contraindication to immediate definitive plating, mandating a staged approach.
Below is an exhaustive summary of the indications and contraindications for the MIPO technique in tibial pilon fractures:
| Category | Specific Clinical Scenarios | Rationale / Considerations |
|---|---|---|
| Primary Indications | High-energy AO/OTA 43-B and 43-C fractures; Severe metaphyseal comminution; Osteoporotic bone requiring locked constructs. | Allows bridging of comminution without periosteal stripping; locking plates provide superior hold in poor bone stock. |
| Relative Indications | Low-energy rotational injuries with diaphyseal extension; Patients with medical comorbidities (diabetes, smoking, mild PVD). | Minimizes surgical footprint in patients prone to wound healing complications; preserves vascularity. |
| Relative Contraindications | Purely central "die-punch" impactions requiring direct visualization; Extreme articular comminution incapable of indirect reduction. | MIPO limits direct articular visualization; limited arthrotomy may be insufficient for complex articular reconstruction. |
| Absolute Contraindications | Active deep soft tissue infection; Gustilo-Anderson Type IIIB/IIIC open fractures; Non-reconstructable vascular injury; Acute presentation with severe edema/blisters. | High risk of deep infection and limb loss; definitive fixation must be delayed until soft tissue envelope is stabilized and optimized. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a MIPO procedure for a tibial pilon fracture is predetermined long before the first incision is made. The universally accepted paradigm for managing these high-energy injuries is the "Span, Scan, and Plan" protocol. This staged approach recognizes that the initial injury imparts massive trauma not only to the bone but to the surrounding soft tissue envelope. Attempting definitive fixation in the acute setting is a historic error that guarantees high rates of catastrophic complications. Therefore, the immediate goal upon presentation is damage control orthopedic surgery.
The "Span" phase involves the immediate application of a joint-spanning external fixator. This achieves several critical objectives: it restores the mechanical axis of the lower extremity, utilizes ligamentotaxis to indirectly reduce the articular fragments, unloads the compromised soft tissue envelope, and provides rigid stability to mitigate ongoing secondary soft tissue injury from mobile fracture fragments. Once the limb is spanned and resting at length, the "Scan" phase is initiated. A high-resolution, fine-cut Computed Tomography (CT) scan with 2D multiplanar reconstructions (coronal and sagittal) and 3D surface rendering is absolutely mandatory. Plain radiographs are grossly insufficient for understanding the complex spatial geometry of a shattered tibial plafond.
During the "Plan" phase, the orthopedic surgeon acts as an architect. The CT scan is meticulously analyzed to map the primary fracture lines, identify the location and size of the Chaput, Volkmann, and medial malleolar fragments, and locate any impacted central die-punch fragments. Preoperative templating software is utilized to select the appropriate implant. The surgeon must choose a precontoured locking plate that is long enough to span the zone of comminution, ensuring an adequate working length to provide relative stability. The rule of thumb dictates that the plate should have at least three, and preferably four or five, empty screw holes bridging the fracture site to optimize interfragmentary strain. Furthermore, the surgeon must plan the sequence of reduction: typically, the fibula is addressed first to restore the lateral column, followed by reconstruction of the articular block, and finally, the diaphyseal-metaphyseal bridging.


Patient positioning in the operating room must facilitate unhindered access and perfect fluoroscopic visualization. The patient is placed supine on a fully radiolucent Jackson or flat top table. A bump is placed under the ipsilateral hip to correct the natural external rotation of the lower extremity, bringing the patella and the foot into a true anteroposterior alignment. A pneumatic tourniquet is applied to the proximal thigh, though its use should be judicious to minimize ischemic time, particularly in patients with compromised vascularity. The C-arm fluoroscope is positioned on the contralateral side of the table, allowing for effortless transitions between true AP, lateral, and mortise views of the ankle without moving the injured limb. The entire leg, from the toes to the proximal thigh, including the spanning external fixator, is prepped and draped into the sterile field to allow for dynamic manipulation during the procedure.
Step-by-Step Surgical Approach and Fixation Technique
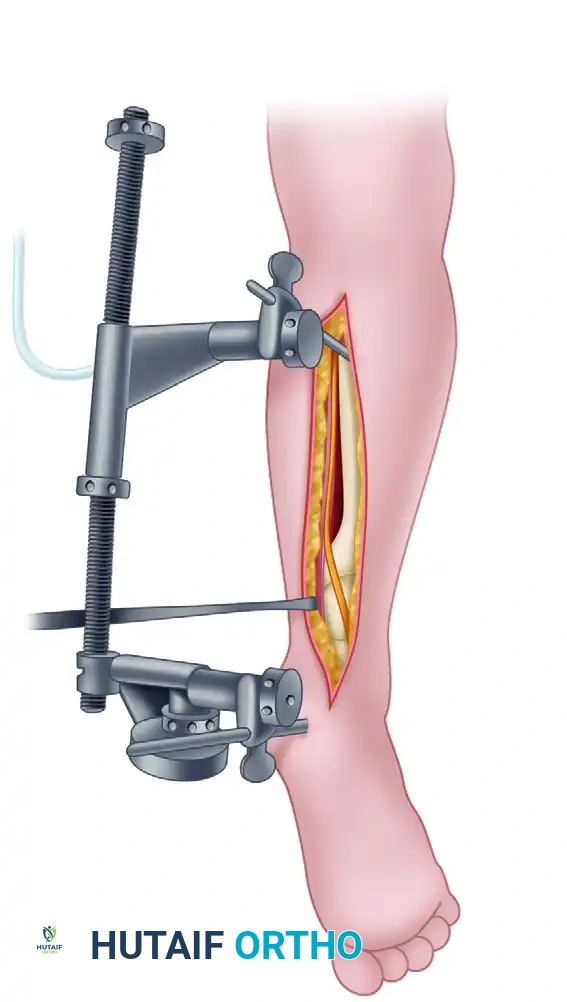
The definitive surgical management of a tibial pilon fracture via MIPO is a technically demanding, multi-staged endeavor. Stage 1, the initial damage control phase, focuses on skeletal stabilization and soft tissue resuscitation. If the lateral soft tissue envelope is pristine, the surgeon may elect to perform an open reduction and internal fixation of the fibula using a standard posterolateral approach and a one-third tubular plate. This reestablishes the lateral column and dramatically aids in the indirect reduction of the tibial articular block via ligamentotaxis. Following fibular fixation, a rigid, triangular delta-frame external fixator is constructed. Two 5.0-mm Schanz pins are placed in the safe zone of the anteromedial tibial diaphysis, and a centrally threaded transfixation pin is driven through the calcaneal tuberosity, meticulously avoiding the medial neurovascular bundle. Longitudinal traction is applied, the frame is locked, and the patient is admitted for elevation and soft tissue monitoring.
Stage 2, the definitive MIPO reconstruction, is undertaken only when the soft tissues dictate readiness—typically 10 to 21 days post-injury. The classic clinical indicators of readiness include the resolution of fracture blisters, the subsidence of pitting edema, and the presence of the "wrinkle sign" upon dorsiflexion of the ankle. The procedure begins with the removal of the external fixator and meticulous reprepping of the limb. The first operative objective is the anatomic reduction of the articular surface. Depending on the preoperative CT plan, this may be achieved percutaneously using large pointed reduction forceps (Weber clamps) and K-wires, or it may require a limited anterior arthrotomy to directly visualize the joint, elevate depressed die-punch fragments, and pack metaphyseal voids with cancellous allograft or autograft. Once the articular block is anatomically reconstructed, it is provisionally held with K-wires and definitively fixed with independent 3.5-mm or 4.0-mm lag screws, converting a complex AO/OTA 43-C fracture into a 43-A fracture.
With the articular block stabilized, the MIPO technique for the metadiaphyseal segment commences. Based on the fracture morphology, the surgeon selects an anteromedial, anterolateral, or occasionally a posterolateral approach. For an anteromedial MIPO, a 3- to 4-cm incision is made distally over the medial malleolus, carefully protecting the saphenous nerve and vein. A second small incision is made proximally at the anticipated termination of the plate. A specialized tunneling instrument, or a long Kelly clamp, is introduced through the distal incision and advanced proximally, staying strictly extraperiosteal and directly on the bone to create a safe subcutaneous corridor.

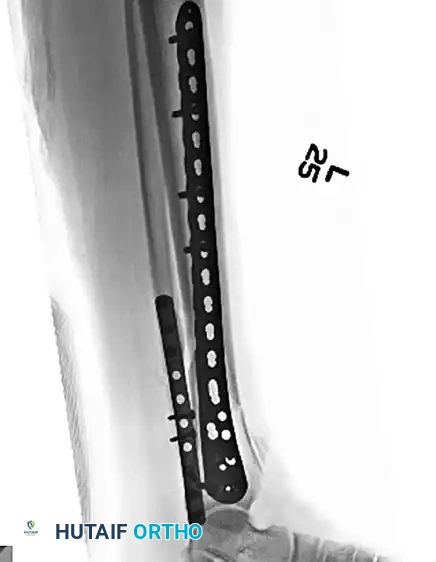
A precontoured locking plate of appropriate length is selected. A heavy non-absorbable suture (e.g., #5 Ethibond) is tied to the most proximal hole of the plate. The Kelly clamp is passed from the proximal incision, down the extraperiosteal tunnel, to grasp the suture. The plate is then smoothly pulled proximally into the tunnel under continuous fluoroscopic guidance, ensuring it sits flush against the bone without interposing soft tissue. The plate is provisionally fixed to the bone using K-wires distally and proximally. The mechanical axis (length, alignment, and rotation) is rigorously verified using fluoroscopy and clinical alignment checks (e.g., the cable method).
Once alignment is deemed perfect, definitive fixation is achieved. The distal segment is secured with at least three to four locking screws to maximize purchase in the often osteopenic metaphyseal bone. Proximally, cortical screws may be used to draw the plate to the bone, followed by locking screws to complete the rigid construct. If the fracture pattern permits, a non-locking lag screw can be placed through the plate to compress specific fracture lines, though this must not compromise the overall relative stability of the bridging construct. Final orthogonal fluoroscopic images are obtained, the wounds are copiously irrigated, and meticulous, tension-free closure is performed, frequently utilizing closed-suction drains to prevent hematoma formation and subsequent wound breakdown.

Complications, Incidence Rates, and Salvage Management
Despite the advent of MIPO and the rigid adherence to staged protocols, tibial pilon fractures remain fraught with complications. The severity of the initial trauma, combined with the fragile nature of the distal tibial soft tissue envelope, ensures that even perfectly executed surgeries carry a significant risk of morbidity. The surgeon must be hyper-vigilant in the postoperative period, as early recognition and aggressive management of complications are critical to preventing catastrophic outcomes such as limb loss.
Soft tissue complications, ranging from superficial wound dehiscence to deep, limb-threatening infections, are the most dreaded sequelae. Superficial necrosis often occurs at the margins of the surgical incisions, particularly if excessive retraction was utilized or if the incisions were made through previously blistered skin. These can often be managed with local wound care, oral antibiotics, and occasionally, negative pressure wound therapy (NPWT). However, deep infections involving the hardware or the bone (osteomyelitis) are disastrous. Management requires immediate return to the operating room for radical debridement, removal of any loose hardware (while attempting to maintain stability if the fracture is unhealed), and the placement of antibiotic-impregnated polymethylmethacrylate (PMMA) spacers. The Masquelet technique or bone transport via an Ilizarov frame may ultimately be required to manage the resulting segmental bone defects.
Nonunion and malunion are also significant concerns, occurring in approximately 5% to 15% of cases. Nonunions are particularly prevalent in the metaphyseal-diaphyseal junction if the biological environment was severely compromised or if the MIPO construct was excessively rigid (preventing the necessary micromotion for secondary healing). Hypertrophic nonunions are managed by improving mechanical stability, often by revising the plate or exchanging to an intramedullary nail if feasible. Atrophic nonunions require biological augmentation, such as autologous bone grafting (e.g., Reamer-Irrigator-Aspirator [RIA] graft from the femur) or the use of orthobiologics like Bone Morphogenetic Proteins (BMPs). Malunions, particularly varus collapse, alter the biomechanics of the ankle joint and rapidly accelerate the onset of post-traumatic osteoarthritis.
Post-traumatic osteoarthritis (PTOA) is the most common long-term complication, affecting up to 50% of patients regardless of the quality of the articular reduction. The initial impact causes irreversible chondrocyte apoptosis, leading to progressive cartilage degradation. When conservative measures (bracing, injections, NSAIDs) fail, salvage procedures become necessary. The gold standard salvage for end-stage pilon PTOA is a tibiotalar or tibiotalocalcaneal (TTC) arthrodesis, often utilizing a retrograde intramedullary nail or a rigid anterior plate. In cases of intractable infection, massive bone loss, or chronic debilitating pain, a below-knee amputation (BKA) may be the most functional and definitive salvage option, allowing the patient to return to ambulation with a modern prosthesis.
Below is a summary of common complications, their approximate incidence rates, and standard management strategies:
| Complication | Approximate Incidence | Prevention & Management Strategies |
|---|---|---|
| Superficial Wound Infection / Dehiscence | 10% - 20% | Prevention: Strict adherence to staged protocol; tension-free closure. Management: Oral antibiotics, local wound care, NPWT. |
| Deep Infection / Osteomyelitis | 5% - 15% | Prevention: Extra-periosteal tunneling; minimizing operative time. Management: Radical debridement, hardware removal (if unstable), antibiotic spacers, IV antibiotics, flap coverage. |
| Nonunion (Atrophic or Hypertrophic) | 5% - 15% | Prevention: Preserving biology via MIPO; optimizing strain. Management: Hypertrophic requires mechanical stabilization; Atrophic requires biological augmentation (bone graft, BMP). |
| Malunion (Varus/Valgus/Recurvatum) | 5% - 10% | Prevention: Meticulous intraoperative fluoroscopy; restoring fibular length. Management: Corrective osteotomy if symptomatic and joint is preserved. |
| Post-Traumatic Osteoarthritis (PTOA) | 30% - 50% | Prevention: Anatomic articular reduction (absolute stability). Management: NSAIDs, bracing, injections; Salvage via Arthrodesis or Arthroplasty (rarely indicated). |
Phased Post-Operative Rehabilitation Protocols
The surgical fixation of a tibial pilon fracture is only the first step in a prolonged journey toward functional recovery. The postoperative rehabilitation protocol is as critical as the surgery itself and must be meticulously phased to balance the competing demands of soft tissue healing, mechanical stability of the construct, and the prevention of joint stiffness. The protocol is highly individualized, dictated by the severity of the initial injury, the security of the fixation, and the patient's compliance and overall physiological status.
Phase 1: Immediate Postoperative Period (Weeks 0 - 2)
The primary goals during this phase are soft tissue protection, edema control, and pain management. Immediately following surgery, the limb is immobilized in a bulky, well-padded Jones dressing reinforced with a rigid posterior plaster splint. It is absolutely critical that the ankle is immobilized in a strictly neutral (90-degree) position to prevent the development of an equinus contracture, which can be devastating to future gait mechanics. The patient is instructed to keep the limb strictly elevated above the level of the heart to facilitate venous return and minimize swelling. The patient is designated strictly non-weight bearing (NWB) on the operative extremity. Deep vein thrombosis (DVT) prophylaxis is initiated per institutional protocols, typically utilizing low molecular weight heparin or direct oral anticoagulants.
Phase 2: Early Mobilization and Soft Tissue Healing (Weeks 2 - 6)
At the first postoperative visit (usually 10 to 14 days), the splint is removed, and the surgical incisions are meticulously inspected. If epithelialization is complete and the wounds are dry, sutures or staples are removed. If the MIPO construct is deemed mechanically robust, the patient is transitioned to a removable controlled ankle motion (CAM) boot. This marks a critical transition, as early, controlled mobilization is essential to prevent arthrofibrosis of the ankle and subtalar joints. The patient is instructed to remove the CAM boot multiple times a day to perform active and active-assisted range of motion (ROM) exercises, focusing on dorsiflexion, plantarflexion, inversion, and eversion. However, the patient must remain strictly NWB. Physical therapy is formally initiated to focus on core strengthening, upper extremity conditioning, and safe transfer techniques.
Phase 3: Progressive Weight Bearing and Callus Formation (Weeks 6 - 12)
Around the 6-week mark, new orthogonal radiographs are obtained to assess for the presence of bridging callus in the metaphyseal-diaphyseal segment and the maintenance of articular reduction. If early radiographic signs of secondary bone healing are evident, the patient may begin a progressive partial weight-bearing (PWB) protocol. This typically starts at 20% to 30% of body weight, utilizing crutches or a walker, and incrementally increases by 10% to 15% each week, guided by patient tolerance and the absence of pain. The mechanical stress of weight-bearing stimulates the piezoelectric effect, further driving osteoblastic activity and robust callus formation. ROM exercises are intensified, and gentle strengthening with resistance bands is introduced.
Phase 4: Advanced Strengthening and Return to Function (Weeks 12+)
By 10 to 12 weeks postoperatively, definitive clinical and radiographic union is typically achieved. At this stage, the patient is transitioned to full weight-bearing (FWB) in regular supportive footwear, often utilizing a custom orthotic or ankle brace for initial support. Rehabilitation shifts focus to aggressive strengthening of the gastrocnemius-soleus complex, the anterior tibialis, and the peroneal musculature. Proprioceptive training, utilizing wobble boards and uneven surfaces, is critical to restore neuromuscular control and prevent future instability. Patients must be counseled that maximal medical improvement (MMI) following a severe pilon fracture often takes 12 to 18 months, and they may experience persistent aching, weather-related pain, and mild swelling for the rest of their lives.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the MIPO technique for tibial pilon fractures is deeply rooted in decades of rigorous clinical research and a paradigm shift in orthopedic trauma philosophy. Understanding the landmark literature is essential for the modern surgeon, as it provides the evidence-based foundation for the protocols utilized today.
The historical baseline was established in the 1960s and 70s by the AO group, notably Rüedi and Allgöwer, who advocated for anatomical reduction and rigid internal fixation of all pilon fractures. While their early results in low-energy skiing injuries were promising, the application of these extensile techniques to high-energy injuries in the 1980s and 90s resulted in disastrous complication rates. Studies by Bourne et al. and McFerran et al. reported deep infection rates exceeding
