Ankle Fracture: Your Guide to a Fractured Ankle Injury
Key Takeaway
This topic focuses on Ankle Fracture: Your Guide to a Fractured Ankle Injury, A fracture ankle fracture ankle is a common skeletal injury, often caused by rotational mechanisms like external rotation with a supinated foot. It involves breaks in the malleoli—medial, lateral, or posterior—which form the ankle mortise. The lateral malleolus is most frequently fractured, and posterior malleolus integrity is crucial for joint stability.
Introduction and Epidemiology
Ankle fractures represent one of the most common skeletal injuries encountered by orthopedic surgeons, accounting for nearly 10% of all fractures. The incidence is estimated at 187 per 100,000 person-years, with a bimodal distribution affecting young males predominantly through high-energy trauma or sports-related injuries, and older females through low-energy falls secondary to osteoporotic bone changes. The management of these fractures demands a comprehensive understanding of ankle biomechanics, precise radiographic interpretation, and meticulous surgical technique to restore the articular congruity and dynamic stability of the tibiotalar joint.
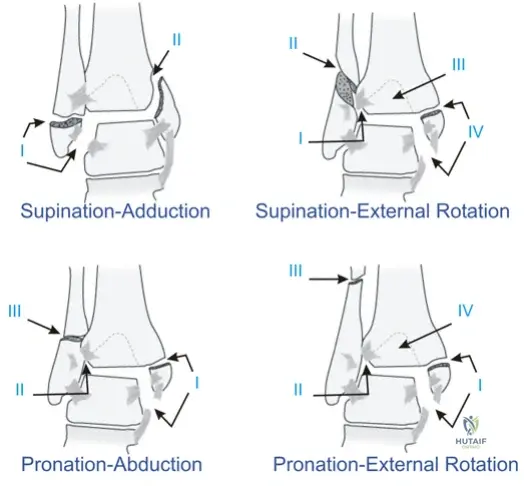
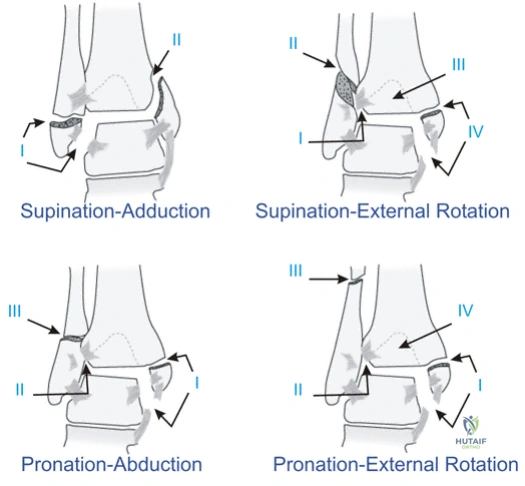
The mechanism of injury is classically rotational, dictating the predictable sequence of ligamentous and osseous failure. The Lauge-Hansen classification system remains the most robust framework for understanding these rotational mechanisms, categorized by the position of the foot at the time of injury (supination or pronation) and the deforming force applied to the talus (external rotation, adduction, or abduction). Supination-External Rotation (SER) is the most prevalent pattern, accounting for up to 70% of all ankle fractures, followed by Supination-Adduction (SA), Pronation-External Rotation (PER), and Pronation-Abduction (PA). Understanding these sequential injury patterns is paramount for both accurate diagnosis and the execution of anatomic reduction, as the surgical sequence often reverses the mechanism of injury.
Surgical Anatomy and Biomechanics
Osteology of the Ankle Joint
The ankle joint, or talocrural joint, is a highly congruent hinge joint formed by the distal tibia, the distal fibula, and the talus. The distal tibial articular surface, known as the plafond, forms the roof of the mortise. The medial malleolus represents the medial flare of the distal tibia. Its inner surface is divided by a groove that defines the anterior colliculus (the larger prominence and attachment site for the superficial deltoid ligament) and the posterior colliculus (the attachment site for the deep deltoid ligament).
The lateral malleolus is the lateral flare of the distal fibula and is the most commonly fractured structure in the ankle ring. The distal fibula lies within the incisura fibularis, a concave longitudinal groove along the distal lateral tibia that forms the osseous component of the syndesmosis. The posterior malleolus refers to the posterior flare of the distal tibia, whose anatomical integrity is critical for posterior joint stability and load transfer.
The mortise articulates with the talar dome, which is trapezoidal in shape—approximately 2.5 mm wider anteriorly than posteriorly. This anatomical nuance dictates ankle kinematics: in dorsiflexion, the wider anterior portion of the talar dome engages the mortise, forcing the fibula laterally and into external rotation. Conversely, in plantarflexion, the talar dome rotates internally due to the checkrein action of the intact deltoid ligament.
Ligamentous Anatomy
The stability of the ankle joint relies heavily on its ligamentous complexes.
The Lateral Ligament Complex:
Originating from the lateral malleolus, this complex is generally not as robust as its medial counterpart.
* Anterior Talofibular Ligament (ATFL): The weakest ligament of the complex and typically the first to fail under inversion stress. It attaches at the anterior fibula and inserts on the talar neck, primarily functioning to prevent anterior subluxation of the talus (evaluated clinically via the anterior drawer test).
* Calcaneofibular Ligament (CFL): Spans from the tip of the lateral malleolus to the lateral calcaneus, resisting inversion forces.
* Posterior Talofibular Ligament (PTFL): The strongest of the lateral ligaments. It attaches at the lateral talar tubercle and prevents posterior subluxation of the talus. Due to its tensile strength, failure often results in a bony avulsion rather than mid-substance rupture.
The Medial Ligament Complex:
The deltoid ligament is the primary stabilizer of the medial ankle, resisting valgus stress and lateral translation of the talus.
* Superficial Portion: Originates from the anterior colliculus and comprises three distinct bands: the tibionavicular ligament (suspends the spring ligament), the tibiocalcaneal ligament (attaches to the sustentaculum tali to prevent valgus), and the tibiotalar ligament.
* Deep Portion: The primary medial stabilizer of the ankle. It originates from the posterior colliculus and intercollicular groove, attaching to the non-articular portion of the medial talus. It is intraarticular but extrasynovial. Disruption of the deep deltoid, or its bony attachment at the medial malleolus, results in profound abnormal talar motion and lateral shift.
The Syndesmotic Complex:
The distal tibiofibular syndesmosis maintains the integrity of the mortise and consists of the anterior inferior tibiofibular ligament (AITFL), the posterior inferior tibiofibular ligament (PITFL), the interosseous ligament (a distal continuation of the interosseous membrane), and the transverse ligament.
Muscular Compartments and Neurovascular Structures
The leg is divided into four distinct fascial compartments, which must be respected during surgical approaches to prevent iatrogenic injury and compartment syndrome.
* Anterior Compartment: Contains the tibialis anterior, extensor hallucis longus (EHL), extensor digitorum longus (EDL), and peroneus tertius. The deep peroneal nerve and anterior tibial vessels course through this compartment.
* Lateral Compartment: Contains the peroneus longus and brevis, along with the superficial peroneal nerve.
* Deep Posterior Compartment: Contains the flexor digitorum longus (FDL), flexor hallucis longus (FHL), tibialis posterior, posterior tibial vessels, and the tibial nerve.
* Superficial Posterior Compartment: Contains the gastrocnemius, soleus, and plantaris.

When executing surgical approaches, the local neurovascular relationships are paramount:
* Lateral: The peroneal tendons pass posterior to the lateral malleolus under the superior peroneal retinaculum. Superficial to the peroneals at this level lies the sural nerve and lesser saphenous vein.
* Medial: Posterior to the medial malleolus lie the tibialis posterior, FDL, and FHL tendons, along with the posterior tibial vessels and tibial nerve, all passing under the flexor retinaculum (laciniate ligament). Anterior to the medial malleolus run the greater saphenous vein and saphenous nerve.
* Anterior: Under the extensor retinaculum lie the anterior compartment tendons, deep peroneal nerve, and anterior tibial vessels. The superficial peroneal nerve arborizes superficial to the extensor retinaculum.
* Posterior: The Achilles and plantaris tendons dominate the posterior aspect.
Biomechanical Considerations
Normal range of motion (ROM) of the ankle is approximately 30° of dorsiflexion and 45° of plantarflexion. However, the minimum functional ROM required for normal gait is 10° of dorsiflexion and 20° of plantarflexion. The axis of rotation of the ankle joint is externally rotated approximately 20° compared to the coronal axis of the knee. Biomechanical studies, notably by Ramsey and Hamilton, have demonstrated that a mere 1 mm of lateral talar shift decreases the tibiotalar contact area by 42%. This exponential loss of contact area leads to significantly elevated peak articular pressures, underscoring the absolute necessity for anatomic reduction of the mortise to prevent rapid onset post-traumatic osteoarthritis.
Indications and Contraindications
The decision to proceed with operative versus non-operative management hinges on the stability of the ankle mortise. The fundamental goal of treatment is the restoration of articular congruity and the prevention of talar shift.
Operative Versus Non Operative Management Parameters
| Clinical Scenario | Management Strategy | Rationale and Criteria |
|---|---|---|
| Isolated Lateral Malleolus (Weber A or B) | Non-Operative | Intact medial structures (no deltoid tenderness, normal medial clear space on stress views). Treated with weight-bearing as tolerated in a CAM boot or cast. |
| Non-displaced Medial Malleolus | Non-Operative | Rare in isolation. Must ensure no occult syndesmotic or lateral injury. Cast immobilization. |
| Bimalleolar Fractures | Operative (ORIF) | Inherently unstable. Loss of both medial and lateral columns leads to inevitable talar shift. |
| Trimalleolar Fractures | Operative (ORIF) | Unstable. Posterior malleolar fixation indicated for fragments >25% of the plafond, or any size if associated with posterior talar subluxation or syndesmotic instability. |
| Bimalleolar Equivalent | Operative (ORIF) | Lateral malleolus fracture with a complete deltoid ligament rupture (evidenced by medial clear space >4 mm on stress radiographs). |
| Syndesmotic Disruption | Operative | Widened tibiofibular clear space or medial clear space requiring trans-syndesmotic fixation (screws or flexible suture buttons). |
| Open Fractures | Operative | Requires emergent irrigation, debridement, and stabilization (external fixation or definitive ORIF depending on soft tissue envelope). |
Contraindications to Surgery
Absolute contraindications include active local soft tissue infection, severe peripheral arterial disease precluding wound healing, and medically unstable patients unable to tolerate anesthesia. Relative contraindications include severe diabetic neuropathy (Charcot arthropathy), which may necessitate augmented fixation strategies (e.g., tibiotalocalcaneal nailing or multi-planar external fixation) rather than standard open reduction and internal fixation (ORIF), as well as severe soft tissue swelling (fracture blisters), which dictates a staged protocol utilizing a temporizing spanning external fixator until the "wrinkle sign" appears.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning begins with a meticulous clinical examination of the soft tissue envelope. The presence of fracture blisters, severe edema, or open wounds dictates the timing of definitive fixation.
Radiographic Evaluation
Standard radiographic assessment includes weight-bearing (if possible) anteroposterior (AP), lateral, and mortise views. The mortise view is obtained with the leg internally rotated 15° to 20° to overcome the normal fibular retroversion, allowing clear visualization of the tibiotalar joint space.
Key radiographic parameters include:
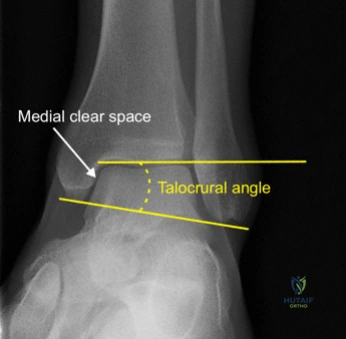
* Medial Clear Space: Should be ≤ 4 mm. Widening indicates deltoid ligament disruption and lateral talar shift.
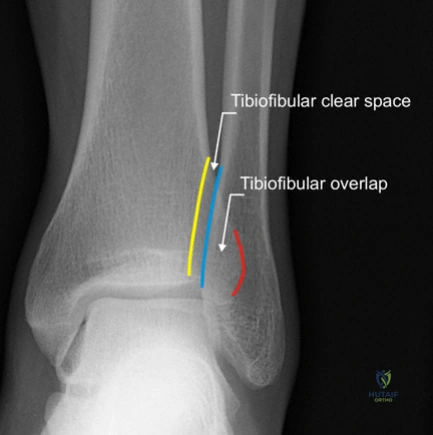
* Tibiofibular Overlap: Should be > 1 mm on the mortise view and > 6 mm on the AP view.
* Tibiofibular Clear Space: Should be < 5 mm on both AP and mortise views. Measurement > 5 mm indicates syndesmotic diastasis.
* Talar Tilt: The articular surface of the talar dome should be strictly parallel to the tibial plafond.
Advanced imaging with Computed Tomography (CT) is increasingly recognized as the standard of care for operative planning in the presence of posterior malleolar fractures, complex articular comminution, or suspected impaction of the tibial plafond (die-punch fragments). CT imaging allows for precise mapping of the posterior malleolus, determining whether a posterolateral or posteromedial approach is required.
Patient Positioning Setup
Patient positioning is dictated by the fracture pattern and the planned surgical approaches.
* Supine Positioning: Utilized for standard lateral and medial approaches. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the lateral malleolus anteriorly for easier access. A radiolucent triangle may be used to elevate the leg, facilitating lateral fluoroscopy.
* Prone Positioning: Indicated when a posterolateral approach is required for direct reduction and fixation of a displaced posterior malleolus fracture, combined with lateral malleolus fixation.
* Lateral Decubitus: Occasionally used for isolated lateral and posterior malleolar injuries, though it restricts access to the medial side.
A well-padded thigh tourniquet is applied to provide a bloodless surgical field. Intraoperative fluoroscopy (C-arm) must be positioned to allow unhindered AP, lateral, and mortise views throughout the procedure.
Detailed Surgical Approach and Technique
The surgical sequence typically addresses the fibula first to restore the lateral column and length, followed by the posterior malleolus, the medial malleolus, and finally, the syndesmosis.
Lateral Approach to the Fibula
The lateral malleolus is approached via a longitudinal incision centered over the fibula, curving slightly anteriorly at the distal tip to avoid the sural nerve. The internervous plane is technically between the superficial peroneal nerve (anteriorly) and the sural nerve (posteriorly).
- Dissection: Subcutaneous tissues are divided meticulously to preserve the vascularity of the skin flaps. Full-thickness flaps are elevated down to the periosteum. The sural nerve and lesser saphenous vein must be identified and protected if the incision extends posteriorly.
- Fracture Preparation: The fracture site is exposed, and the hematoma is evacuated. The periosteum is stripped only 1-2 mm from the fracture edges to preserve blood supply while allowing direct visualization of the cortical read.
- Reduction and Fixation: For simple oblique or spiral fractures (Weber B), anatomic reduction is achieved using a reduction forceps. A 3.5 mm cortical lag screw is placed perpendicular to the fracture plane to achieve interfragmentary compression. The technique involves drilling a 3.5 mm glide hole in the near cortex, a 2.5 mm thread hole in the far cortex, countersinking, measuring, tapping, and screw insertion.
- Plate Application: A 1/3 tubular plate or pre-contoured locking plate is applied in neutralization mode to protect the lag screw from torsional and bending forces. Alternatively, for short oblique fractures, an antiglide plate positioned on the posterolateral surface of the fibula can provide excellent biomechanical stability by utilizing the intact anterior cortex to resist proximal migration of the distal fragment.
Medial Approach to the Tibia
The medial malleolus is approached via a longitudinal or slightly curved incision centered over the medial malleolus.
1. Dissection: The greater saphenous vein and saphenous nerve lie anterior to the incision and must be protected. Full-thickness flaps are developed.
2. Joint Inspection: The fracture is opened, and the tibiotalar joint is inspected for osteochondral loose bodies or interposed periosteum, which commonly blocks anatomic reduction of the medial malleolus.
3. Reduction and Fixation: The fracture is reduced with a pointed reduction clamp. Fixation is typically achieved using two 4.0 mm partially threaded cancellous screws placed perpendicular to the fracture line to provide compression. For vertical shear fractures (often seen in SA mechanisms), an anti-glide or buttress plate is required to resist the vertical displacement forces.
Posterolateral Approach for the Posterior Malleolus
When direct fixation of the posterior malleolus is indicated, the patient is positioned prone.
1. Incision and Interval: A longitudinal incision is made midway between the posterior border of the fibula and the lateral border of the Achilles tendon. The superficial fascia is incised, and the lesser saphenous vein and sural nerve are retracted laterally.
2. Deep Dissection: The deep fascial interval is developed between the peroneal tendons (retracted laterally) and the flexor hallucis longus (FHL) (retracted medially). This exposes the posterior aspect of the distal tibia and the posterior malleolus.
3. Fixation: The fracture is reduced under direct vision and stabilized with anteriorly directed lag screws or a posterior buttress plate. This approach also affords excellent access to the posterior aspect of the fibula for concurrent lateral column fixation.
Syndesmotic Evaluation and Fixation
Following osseous fixation, the syndesmosis must be rigorously tested. The "Cotton test" involves placing a bone hook around the fibula and applying a lateral traction force under fluoroscopy. Widening of the tibiofibular clear space or medial clear space indicates syndesmotic instability. Alternatively, an external rotation stress test can be applied to the foot.
If unstable, the syndesmosis is reduced by applying a large pelvic reduction clamp across the medial and lateral malleoli with the ankle in neutral dorsiflexion. Fixation is achieved using either trans-syndesmotic screws (typically one or two 3.5 mm or 4.5 mm cortical screws placed across three or four cortices) or flexible suture button constructs. Suture buttons offer the biomechanical advantage of allowing physiologic micromotion of the syndesmosis and eliminate the need for routine hardware removal.
Complications and Management
The management of ankle fractures is fraught with potential complications, largely driven by the precarious soft tissue envelope surrounding the distal tibia and fibula, as well as the unforgiving biomechanics of the tibiotalar joint.
Common Complications and Salvage Strategies
| Complication | Incidence | Etiology and Risk Factors | Management and Salvage Strategies |
|---|---|---|---|
| Wound Dehiscence / Infection | 2% - 10% | Poor soft tissue handling, smoking, diabetes mellitus, operating through severe edema. | Superficial: Oral/IV antibiotics, local wound care. Deep: Emergent surgical debridement, hardware retention if stable, removal if loose. Vacuum-assisted closure (VAC) or flap coverage may be required. |
| Post-Traumatic Osteoarthritis | 10% - 40% | Malreduction (even 1 mm shift), initial articular cartilage impact damage, syndesmotic malreduction. | Initial conservative management (bracing, NSAIDs, injections). Definitive surgical salvage via ankle arthrodesis or total ankle arthroplasty (TAA). |
| Syndesmotic Malreduction | Up to 39% | Failure to directly visualize the incisura, over-compression with clamps, reliance on standard 2D fluoroscopy. | Intraoperative 3D fluoroscopy or post-operative CT. Early revision surgery with open debridement of the syndesmosis and re-fixation is critical to prevent late arthritis. |
| Nonunion | < 3% | Inadequate fixation, infection, severe comminution, smoking. Medial malleolus most common site. | Revision ORIF with autologous bone grafting. Optimization of host factors (smoking cessation, glycemic control). |
| Hardware Prominence | 15% - 30% | Thin subcutaneous tissue laterally and medially. Use of bulky plates. | Symptomatic hardware removal after complete radiographic union (typically > 6-12 months post-operatively). |
| Complex Regional Pain Syndrome (CRPS) | 1% - 5% | High energy trauma, prolonged immobilization, tight casts. | Early recognition. Aggressive physical therapy, neuropathic pain modulators (gabapentin/pregabalin), sympathetic nerve blocks. |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must balance the need for rigid immobilization to facilitate osseous union with the necessity of early motion to prevent joint stiffness and capsular contracture. Protocols vary based on the stability of the fixation and patient compliance.
Phase 1: Immediate Post-Operative (Weeks 0-2)
The patient is placed in a well-padded short leg splint in neutral dorsiflexion to prevent equinus contracture. The patient remains strictly non-weight-bearing (NWB). Elevation and cryotherapy are emphasized to mitigate edema. Deep vein thrombosis (DVT) prophylaxis is initiated based on patient risk stratification.
Phase 2: Early Healing and Motion (Weeks 2-6)
At the two-week mark, sutures are removed. For patients with highly stable fixation, the splint is transitioned to a removable Controlled Ankle Motion (CAM) boot. Active range of motion (AROM) exercises for dorsiflexion and plantarflexion are initiated out of the boot. Inversion and eversion are typically restricted to protect the syndesmosis and medial/lateral ligamentous repairs. Weight-bearing status remains NWB or touch-down weight-bearing (TDWB) depending on surgeon preference and fracture complexity. If syndesmotic screws were utilized, strict NWB is often maintained for 6 weeks to prevent screw breakage.
Phase 3: Weight-Bearing Progression (Weeks 6-12)
Radiographs are obtained at 6 weeks to assess for callus formation and maintenance of the mortise. If clinical and radiographic progression is satisfactory, the patient is transitioned to progressive weight-bearing in the CAM boot, advancing to full weight-bearing (FWB) over a 2-to-4-week period. Physical therapy is intensified, focusing on isometric strengthening, proprioceptive retraining (e.g., BAPS board), and normalization of gait mechanics.
Phase 4: Return to Activity (Months 3-6)
The patient is weaned from the CAM boot to an ankle lacer brace or supportive footwear. Advanced plyometrics, sport-specific drills, and dynamic balance exercises are incorporated. Full functional recovery and maximal medical improvement may take up to 12 to 18 months, and patients must be counseled that mild residual swelling and aching after strenuous activity are common long-term sequelae.
Summary of Key Literature and Guidelines
Evidence-based management of ankle fractures relies on several foundational studies and evolving clinical guidelines.
- Biomechanical Foundations: The seminal work by Ramsey and Hamilton (1976) remains the cornerstone of ankle fracture management, definitively proving that a 1 mm lateral shift of the talus results in a 42% decrease in tibiotalar contact area. This study dictates the absolute requirement for anatomic reduction.
- Classification Systems: The Lauge-Hansen classification (1950) provides the mechanistic understanding necessary for closed reduction maneuvers and predicting associated ligamentous injuries. The Danis-Weber classification is heavily utilized for its simplicity, categorizing fractures based on the level of the fibular fracture relative to the syndesmosis (Type A: infra-syndesmotic; Type B: trans-syndesmotic; Type C: supra-syndesmotic), effectively guiding the index of suspicion for syndesmotic instability.
- Syndesmotic Fixation: Recent multicenter randomized controlled trials comparing syndesmotic screws to flexible suture buttons have demonstrated that suture buttons yield slightly superior functional outcomes (measured via AOFAS scores), lower rates of malreduction, and eliminate the need for routine hardware removal procedures.
- Posterior Malleolus Management: Historically, posterior malleolus fractures involving less than 25% to 33% of the articular surface were managed non-operatively. Contemporary guidelines and recent literature strongly advocate for direct fixation of posterior malleolar fragments of any size if they contribute to syndesmotic instability or posterior talar subluxation, given that the posterior inferior tibiofibular ligament (PITFL) remains attached to this fragment. Direct open reduction via a posterolateral approach has been shown to restore the incisura fibularis more accurately than indirect reduction techniques.
- Timing of Surgery: The American Orthopaedic Foot & Ankle Society (AOFAS) guidelines emphasize that surgical intervention should ideally occur within 24 hours of injury, before the onset of profound soft tissue edema. If significant edema or fracture blisters are present, surgery must be delayed until the soft tissue envelope recovers (indicated by the presence of skin wrinkles), typically taking 7 to 14 days, during which temporizing measures such as spanning external fixation may be employed.
Clinical & Radiographic Imaging
