Talus Fractures: Understanding the Talus Bone & Recovery

Key Takeaway
Learn more about Talus Fractures: Understanding the Talus Bone & Recovery and how to manage it. Talus fractures are breaks in the talus bone, second in frequency among tarsal fractures, accounting for 0.1-0.85% of all fractures. The talus, crucial for weight bearing, sees its neck as the most vulnerable site for talus fractures talus injuries. These often result from high-impact trauma like hyperdorsiflexion, impacting the talus's limited vascular supply.
Introduction and Epidemiology
Talus fractures represent a complex and challenging entity within orthopedic traumatology, demanding a profound understanding of hindfoot biomechanics and osseous vascularity. These injuries are second in frequency among all tarsal fractures, following calcaneus fractures. Despite their relative rarity—comprising an incidence ranging from 0.1% to 0.85% of all skeletal fractures and 5% to 7% of all foot injuries—their potential for significant long-term morbidity makes them a critical focus for orthopedic surgeons.
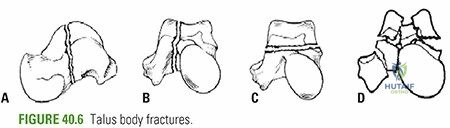
The anatomic distribution of talus fractures is clinically significant. Talar neck fractures are the most prevalent, accounting for approximately 50% of all talus fractures. Talar body fractures constitute 15% to 20%, while fractures of the talar head are exceedingly rare, representing only 3% to 5% of all talus fractures. Lateral process fractures of the talus have seen a distinct epidemiological shift; they are frequently identified in snowboarding injuries, currently accounting for up to 15% of all ankle injuries within that specific athletic demographic.
Concomitant injuries are highly prevalent due to the high-energy mechanisms typically involved. Approximately 14% to 26% of talar neck fractures present with an associated fracture of the medial malleolus. Other associated injuries frequently include fractures of the calcaneus, tibial plafond, spinal column, and contralateral lower extremity.
Mechanism of Injury
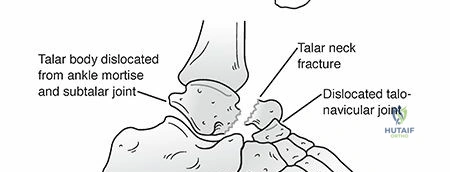
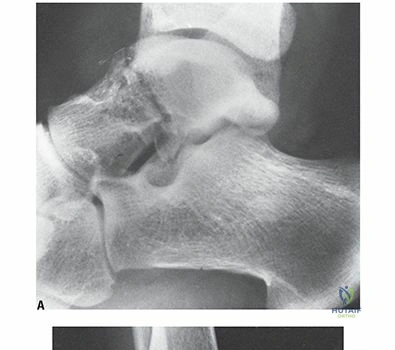
The classic mechanism of injury for a talar neck fracture involves high-energy axial loading combined with hyperdorsiflexion of the ankle. This force vector drives the talar neck superiorly, causing it to impact the anterior margin of the tibial plafond, which acts as a fulcrum, effectively shearing or fracturing the neck. Historically, this injury was termed “Aviator’s astragalus,” a nomenclature derived from early aviation where the rudder bar of a crashing airplane would forcefully impact the plantar aspect of the pilot's foot, resulting in a hyperdorsiflexion talar neck fracture. Today, these injuries are most commonly associated with high-velocity motor vehicle collisions or falls from a significant height.
Surgical Anatomy and Biomechanics
The talus is a unique osseous structure, functioning as the critical intercalary segment that transmits the entire weight of the human body from the tibial plafond into the complex longitudinal and transverse arches of the foot.
Osseous Architecture
Approximately 60% of the talus is covered by articular cartilage, reflecting its extensive participation in the tibiotalar, subtalar, and talonavicular joints. Uniquely, no muscles originate from or insert onto the talus; its stability and spatial orientation are entirely dependent on articular congruity and robust ligamentous constraints.
The body of the talus is covered superiorly by the trochlear articular surface. The anterior aspect of the talar dome is intrinsically wider than the posterior aspect. This trapezoidal morphology confers intrinsic osseous stability to the ankle mortise during dorsiflexion, as the wider anterior segment wedges into the tibiofibular articulation. Medially and laterally, the articular cartilage extends plantarly to articulate with the medial and lateral malleoli. The inferior surface of the talar body forms the complex articulation with the posterior facet of the calcaneus.
The neck of the talus projects anteriorly, deviating medially by 15 to 25 degrees and plantarflexing relative to the body. The neck is structurally narrower, devoid of articular cartilage, and roughened by essential ligamentous attachments and vascular foramina. This anatomic narrowing, combined with its role as a cantilever, makes the talar neck the most vulnerable region to fracture under axial and dorsiflexion loads.
The talar head features continuous articular facets for the navicular anteriorly, the spring ligament (plantar calcaneonavicular ligament) inferiorly, the sustentaculum tali posteroinferiorly, and the deltoid ligament medially.
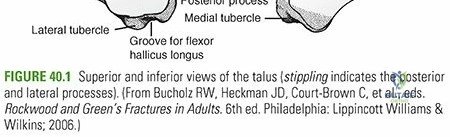
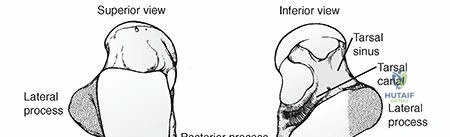
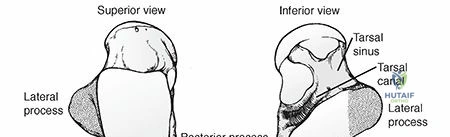
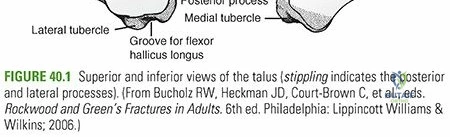
The talus possesses two distinct bony processes. The lateral process is a wedge-shaped structure articulating with the posterior calcaneal facet inferomedially and the lateral malleolus superolaterally. The posterior process consists of a medial and lateral tubercle, which are separated by a distinct fibro-osseous groove housing the flexor hallucis longus (FHL) tendon. An os trigonum, arising from a separate ossification center just posterior to the lateral tubercle, is present in up to 50% of normal feet and must be differentiated from an acute posterior process fracture.
Vascular Supply Dynamics
The vascular anatomy of the talus is arguably its most critical clinical feature, directly dictating the high rates of osteonecrosis following trauma. Because the talus lacks muscular attachments, its vascular supply is entirely dependent on fascial structures, capsular reflections, and ligamentous vessels to penetrate the non-articular regions.
The extraosseous vascular supply forms a rich anastomotic ring, but the intraosseous supply is highly susceptible to disruption. The vascular supply consists of four primary sources:
1. Artery of the Tarsal Canal: A branch of the posterior tibial artery, this is the dominant blood supply to the talar body. It enters the tarsal canal and supplies the majority of the middle and posterior thirds of the talar body.
2. Artery of the Sinus Tarsi: Formed by an anastomosis between the perforating peroneal artery and the dorsalis pedis artery, this vessel supplies the talar head, neck, and the lateral aspect of the talar body.
3. Deltoid Artery: A branch of the posterior tibial artery that runs within the deep deltoid ligament to supply the medial one-third of the talar body.
4. Dorsalis Pedis Branches: Supply the dorsal aspect of the talar head and neck via capsular and ligamentous vessels.
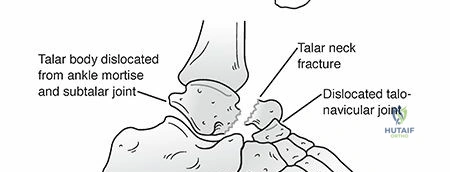
Fractures through the talar neck frequently disrupt the intraosseous anastomoses. If the fracture is displaced, the artery of the tarsal canal and the artery of the sinus tarsi are often compromised. If the body subsequently dislocates posteriorly from the ankle mortise, the deltoid branches are ruptured, rendering the talar body entirely avascular.
Indications and Contraindications
The management of talus fractures is dictated by fracture displacement, articular congruity, and the integrity of the soft tissue envelope. Due to the high risk of malunion, nonunion, and osteonecrosis, the threshold for operative intervention is exceedingly low.
| Clinical Scenario | Management Strategy | Rationale and Considerations |
|---|---|---|
| Strictly Non-Displaced Neck/Body Fractures | Non-Operative | Requires <1mm step-off, intact articular cartilage, and zero varus/valgus malalignment. Managed with strict non-weight-bearing cast immobilization for 8-12 weeks. |
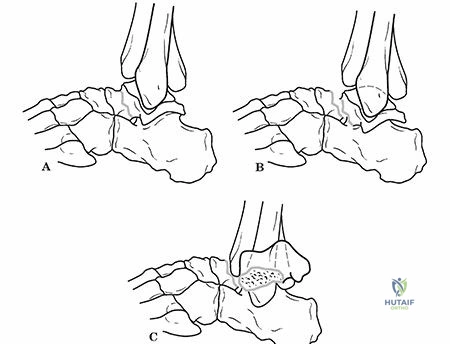
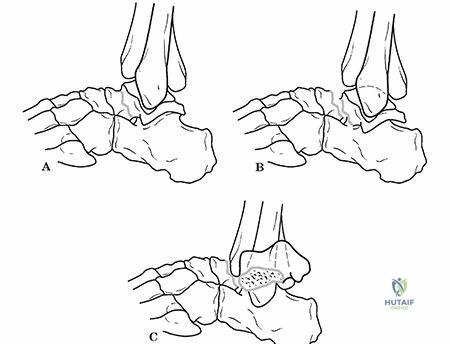
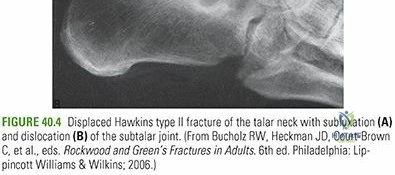
| Displaced Talar Neck Fractures (Hawkins II-IV) | Operative (ORIF) | Anatomic reduction is mandatory to restore joint congruity, decompress the soft tissue envelope, and optimize revascularization of the talar body. |
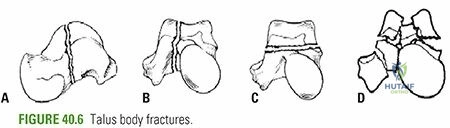
| Displaced Talar Body Fractures | Operative (ORIF) | Essential to restore the tibiotalar and subtalar articular surfaces. May require medial malleolar osteotomy for adequate exposure. |
| Lateral Process Fractures (>1cm or Displaced) | Operative (ORIF or Excision) | Large fragments require fixation to restore subtalar stability. Small, comminuted fragments may be excised to prevent impingement. |
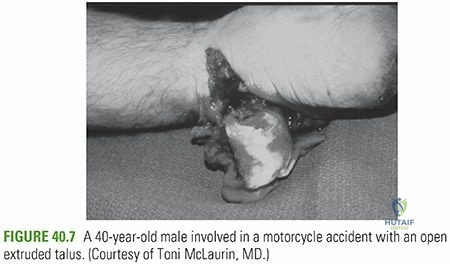
| Open Fractures / Irreducible Dislocations | Urgent Operative | Requires immediate surgical debridement, joint reduction, and stabilization to mitigate catastrophic infection and skin necrosis. |
Contraindications to Immediate Surgical Fixation
While open fractures and irreducible dislocations demand emergent intervention, closed fractures with severe soft tissue compromise (e.g., fracture blisters, massive edema) represent a contraindication to immediate definitive internal fixation. In such cases, the extremity should be placed in a well-padded splint or an external fixator spanning the ankle joint until the soft tissue envelope is amenable to surgical incisions (typically indicated by the presence of skin wrinkling). Active local infection or a medically unstable polytrauma patient also preclude immediate definitive fixation.
Pre Operative Planning and Patient Positioning
Thorough preoperative evaluation is paramount for executing a successful surgical strategy. Patients typically present with severe hindfoot pain, diffuse swelling, and an inability to bear weight.
Clinical and Radiographic Evaluation
Clinical examination must meticulously assess the soft tissue envelope. Talar neck fractures with subtalar or tibiotalar dislocation frequently cause severe skin tenting, most commonly over the medial aspect of the hindfoot, which can rapidly progress to full-thickness skin necrosis if not urgently reduced.

Standard radiographic evaluation includes anteroposterior (AP), mortise, and lateral radiographs of the ankle, alongside AP, lateral, and oblique views of the foot.
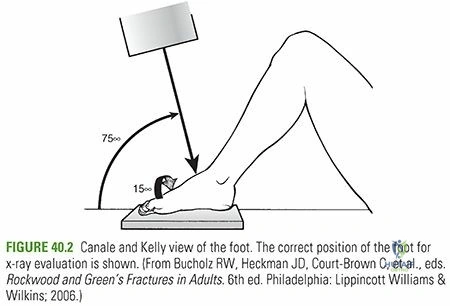
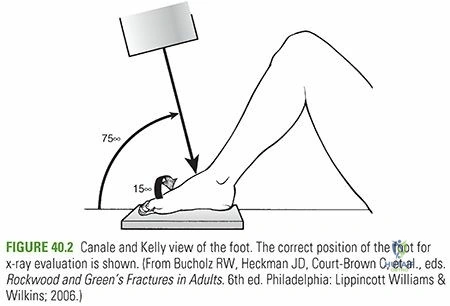
The Canale view is a specialized radiographic projection critical for visualizing the talar neck in profile. It is obtained by placing the ankle in maximum equinus (plantarflexion), pronating the foot 15 degrees, and directing the x-ray beam 75 degrees cephalad from the horizontal plane. This view is indispensable for assessing varus/valgus alignment of the talar neck.
Computed Tomography (CT) scanning with fine cuts (1mm) and multiplanar reconstructions is now considered the standard of care for preoperative planning. CT delineates fracture comminution, articular step-offs, and occult fracture lines that are frequently missed on plain radiography. It allows the surgeon to map precise screw trajectories and anticipate the need for bone grafting or specific plate configurations.
Patient Positioning and Setup
The patient is typically positioned supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position, facilitating access to both the medial and lateral aspects of the ankle. A thigh tourniquet is applied to ensure a bloodless surgical field. Intraoperative fluoroscopy must be positioned to easily obtain AP, lateral, and Canale views without compromising the sterile field.
Detailed Surgical Approach and Technique
The fundamental goal of operative intervention is precise anatomic reduction to restore the congruity of the subtalar and tibiotalar joints, thereby preventing post-traumatic arthritis and minimizing the risk of varus malunion.
Surgical Approaches
To achieve anatomic reduction, dual surgical incisions (anteromedial and anterolateral) are strongly recommended for the majority of displaced talar neck and body fractures. Relying on a single approach frequently leads to an underappreciation of medial comminution, resulting in a catastrophic varus malreduction.
Anteromedial Approach:
The incision is made centered over the talonavicular joint, extending proximally between the tibialis anterior tendon and the medial malleolus. The internervous plane is technically absent here, but care must be taken to protect the terminal branches of the saphenous nerve and vein. The capsule is incised longitudinally to expose the medial talar neck and body. If access to the posterior aspect of the talar body is required, a medial malleolar osteotomy (typically a chevron osteotomy directed towards the axilla of the medial malleolus) can be performed.
Anterolateral Approach:
The incision is placed in line with the fourth ray, starting at the level of the lateral malleolus and extending distally toward the base of the fourth metatarsal. The dissection proceeds lateral to the extensor digitorum longus (EDL) and peroneus tertius tendons. The superficial peroneal nerve branches must be identified and protected. This approach provides excellent visualization of the lateral talar neck, the lateral process, and the subtalar joint.
Reduction and Fixation Strategies
Once the fracture site is exposed bilaterally, the fracture hematoma is evacuated. Small, devitalized articular fragments that cannot be fixed may be excised, but all structural bone must be retained.
Reduction is achieved using pointed reduction forceps. The surgeon must pay meticulous attention to the medial cortex; medial comminution is common, and failure to restore medial length directly causes a varus deformity of the talar neck. Provisional fixation is achieved with multiple Kirschner wires (K-wires) driven from anterior to posterior.

Definitive fixation typically involves multiple headless compression screws or partially threaded cancellous screws (typically 3.5mm or 4.0mm). Screws can be placed from anterior-to-posterior or posterior-to-anterior. Biomechanical studies suggest that posterior-to-anterior screw placement offers superior biomechanical construct stiffness, but it requires a separate posterolateral approach, which may increase surgical morbidity.
In cases of significant comminution where screw fixation alone is insufficient to prevent shortening or varus collapse, mini-fragment plates (2.0mm or 2.4mm) should be utilized in a bridging fashion. The plates are typically applied to the lateral or dorsal aspect of the talar neck to act as a buttress against varus forces.
Complications and Management
The complication profile for talus fractures is notoriously high, driven by the tenuous vascular supply and the extensive articular surface.
| Complication | Incidence / Risk Factors | Management and Salvage Strategies |
|---|---|---|
| Osteonecrosis (AVN) | Hawkins I: 0-15% Hawkins II: 20-50% Hawkins III: 50-100% Hawkins IV: ~100% |
Protected weight-bearing if asymptomatic. Core decompression or vascularized bone grafting for early symptomatic AVN. Talectomy or tibiotalocalcaneal (TTC) arthrodesis for late collapse. |
| Post-Traumatic Arthritis | Subtalar joint: 50-70% Tibiotalar joint: 30-40% |
NSAIDs, bracing, intra-articular injections. Definitive management involves arthrodesis of the affected joint(s) (Subtalar fusion or Ankle fusion). |
| Varus Malunion | Common with isolated lateral approaches or unrecognized medial comminution. | Leads to rigid hindfoot varus and lateral column overload. Requires corrective opening wedge osteotomy of the talar neck or triple arthrodesis. |
| Nonunion | Rare (<5%) due to robust cancellous bone, but occurs with inadequate fixation. | Revision ORIF with autologous bone grafting. |
Assessing Osteonecrosis: The Hawkins Sign
The development of osteonecrosis is the most feared complication. The Hawkins Sign is a critical radiographic prognostic indicator observed on the AP or mortise radiograph of the ankle at approximately 6 to 8 weeks post-injury.

It is characterized by a subchondral radiolucent band in the dome of the talus. This radiolucency indicates subchondral osteopenia, which is a physiologic response to disuse. Crucially, the presence of this osteopenia confirms that the talar body retains an intact vascular supply capable of resorbing bone. Therefore, a positive Hawkins sign is a highly reliable indicator that AVN will not occur. Conversely, a sclerotic or radiodense talar dome at 8 weeks suggests an avascular talar body, though it does not guarantee structural collapse.
Salvage of the Collapsed Talus
When AVN progresses to structural collapse of the talar dome, the patient experiences profound pain and loss of function.
Salvage procedures are complex. If the collapse is localized, focal debridement and grafting may be attempted. However, for widespread collapse and secondary arthritis, a tibiotalocalcaneal (TTC) arthrodesis using a retrograde intramedullary nail or robust plate fixation is often required. In severe cases with massive bone loss, a Blair fusion (sliding tibial graft into the talar neck) or total talus replacement using 3D-printed custom implants are emerging as viable salvage options.
Post Operative Rehabilitation Protocols
Rehabilitation following surgical fixation of a talus fracture requires a delicate balance between protecting the osseous fixation and preventing severe joint contractures.
Phase 1: Immediate Post-Operative (0-2 Weeks)
The patient is placed in a well-padded, short-leg splint in a neutral position. Strict non-weight-bearing (NWB) status is enforced. Elevation and strict edema control are paramount to ensure wound healing.
Phase 2: Early Motion (2-6 Weeks)
Once the surgical incisions have fully healed and sutures are removed, the patient is transitioned to a removable controlled ankle motion (CAM) boot. Strict NWB status is maintained. However, the patient is instructed to remove the boot multiple times daily to perform active and active-assisted range of motion (ROM) exercises for the tibiotalar and subtalar joints. Early mobilization is critical for cartilage nutrition and preventing arthrofibrosis.
Phase 3: Radiographic Assessment and Progression (6-12 Weeks)
At the 6-to-8-week mark, radiographs are obtained to assess for the Hawkins sign and early callus formation. If vascularity is confirmed and clinical healing is progressing, the patient may begin progressive partial weight-bearing in the CAM boot.
Phase 4: Full Weight-Bearing and Strengthening (>12 Weeks)
Assuming radiographic union is achieved, the patient is transitioned to full weight-bearing in a supportive shoe. Formal physical therapy is intensified, focusing on proprioception, peroneal strengthening, and maximizing residual subtalar and
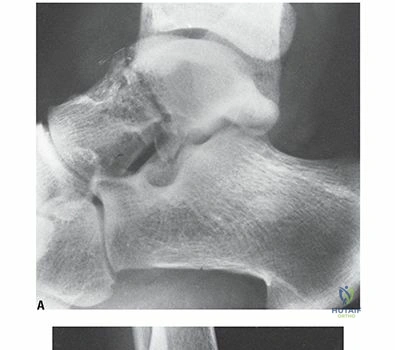
Clinical & Radiographic Imaging