
Arthritides Explained: Symptoms, Diagnosis, and Treatment Options
Introduction and Epidemiology
Arthritides encompass a diverse group of conditions characterized by inflammation and degeneration of articular structures, leading to pain, stiffness, and functional impairment. As orthopedic surgeons, our involvement spans the spectrum from early diagnostic assessment to advanced reconstructive and salvage procedures for end-stage disease. Osteoarthritis (OA) and Neuropathic Arthropathy (Charcot Joint) represent two distinct entities within this spectrum, each with unique pathophysiological mechanisms, clinical presentations, and management paradigms.
Osteoarthritis, the most prevalent form of arthritis globally, is a progressive disorder involving the degradation of articular cartilage and changes in subchondral bone, synovium, and surrounding soft tissues. Its immense burden on healthcare systems and individual quality of life necessitates a thorough understanding of its etiology, progression, and advanced treatment options.
Neuropathic arthropathy, or Charcot joint, while less common than OA, is a profoundly destructive condition demanding specialized surgical expertise. It arises from a loss of protective sensory innervation and proprioception, leading to repetitive microtrauma and subsequent rapid joint disorganization, particularly in the lower extremities of patients with diabetes mellitus.
Osteoarthritis Etiology
Osteoarthritis is a multifactorial disease.
* Idiopathic: No clear primary cause is identified, often considered "wear-and-tear" but is fundamentally a biological process involving dysregulated cartilage metabolism.
* Secondary:
* Genetics: Predisposition can be significant. Defects in type II collagen (Col2) are implicated, and OA affects women more frequently than men, suggesting hormonal or genetic influences.
* Overload: Excessive mechanical stress accelerates cartilage degradation. This includes factors such as obesity, heavy manual labor, joint dysplasia (e.g., femoral acetabular impingement, developmental dysplasia of the hip), and chronic joint malalignment (varus/valgus deformities).
* Trauma: Prior intra-articular fractures, meniscal tears, ligamentous injuries (e.g., ACL rupture), and repetitive impact activities can initiate or accelerate OA progression.
Osteoarthritis Pathological Tissue Changes
The hallmark of OA is a cascade of destructive and dysfunctional tissue alterations:
1. Cartilage: Initial chondrocyte hyperactivity with increased matrix synthesis followed by an imbalance, leading to enzymatic degradation via matrix metalloproteinases (MMPs) and aggrecanases. This results in progressive loss of proteoglycans and collagen, fibrillation, fissuring, and eventual denudation of articular cartilage.

FIG. 1.30 Enzyme cascade of IL-1–stimulated degradation of articular cartilage.
2. Synovium: Secondary inflammation is common, characterized by synovial hypertrophy, cellular infiltration, and increased vascularity. Inflammatory mediators (cytokines like IL-1, TNF-alpha) contribute to cartilage destruction.
3. Ligaments: As joint architecture changes, ligaments on the concave side of a deformity may tighten, while those on the convex side may stretch and become insufficient, contributing to instability.
4. Bone: Subchondral bone undergoes significant remodeling, including subchondral sclerosis (increased bone density), formation of subchondral cysts ("geodes"), and osteophyte formation at joint margins.
* Osteophyte formation is due to pathologic activation of endochondral ossification by periarticular chondrocytes through the Indian hedgehog (Ihh) mechanism.
5. Muscles: Significant atrophy often results from disuse due to pain and guarding, further exacerbating joint instability and functional decline.
Neuropathic Arthropathy Clinical Presentation
Neuropathic arthropathy is characterized by an extreme form of joint destruction.
* Clinical Presentation: Patients typically present with a warm, swollen, erythematous joint, often painlessly or with disproportionately mild pain given the severity of destruction due to the underlying neuropathy. Deformity, instability, and ulceration (particularly in the foot/ankle) are common late-stage findings. The progression can be rapid, sometimes occurring over weeks.
Other arthritides such as Rheumatoid Arthritis (RA), Psoriatic Arthritis (PsA), Gout, and Septic Arthritis also frequently necessitate orthopedic intervention, particularly for managing joint destruction, deformity, or acute infection. While their primary etiologies are distinct, their end-stage manifestations often overlap with OA in requiring reconstructive strategies such as arthroplasty or arthrodesis.
Surgical Anatomy and Biomechanics
A profound understanding of surgical anatomy and biomechanics is fundamental to successful management of arthritic conditions. This section will focus on the principles relevant to the lower extremity, where the vast majority of surgical interventions for OA and neuropathic arthropathy occur.
Articular Cartilage Structure and Function
Articular cartilage is a highly specialized connective tissue characterized by its unique extracellular matrix (ECM), composed primarily of water, type II collagen, and proteoglycans (predominantly aggrecan). This composition confers its remarkable viscoelastic properties, allowing it to withstand high compressive loads, distribute stress across subchondral bone, and provide a low-friction articulating surface. Chondrocytes, the sole cell type within cartilage, maintain the ECM, a process dysregulated in OA. The avascular and aneural nature of articular cartilage contributes to its limited intrinsic repair capacity.

Subchondral Bone Contributions
The subchondral bone plate and cancellous bone below it play a critical role in load transmission and cartilage health. It acts as a shock absorber and a source of nutrients for the basal layer of cartilage. In OA, subchondral bone undergoes significant remodeling, including sclerosis and cyst formation, which can alter its mechanical properties and contribute to cartilage degeneration. The bone-cartilage interface is a dynamic unit, and pathology in one often affects the other.
Synovial Joint Biomechanics
The synovial joint functions as a dynamic system where the interaction of cartilage, synovial fluid, ligaments, and capsule dictates mobility and stability.
* Kinematics: Understanding normal joint motion, including flexion/extension, rotation, and translation, is crucial for restoring function post-arthroplasty. Abnormal kinematics due to deformity or cartilage loss significantly alter load distribution.
* Load Bearing: The knee and hip joints, as major weight-bearing articulations, are particularly susceptible to OA. Varus or valgus malalignment in the knee significantly shifts the mechanical axis, concentrating load on one compartment and accelerating cartilage wear. Similarly, changes in hip center of rotation or femoral offset can alter abductor muscle efficiency and joint contact pressures.
* Ligamentous Stability: Ligaments provide static and dynamic stability. In end-stage arthritis, particularly with significant deformity, ligaments can be contracted or attenuated, necessitating careful intraoperative assessment and balancing during arthroplasty.
Neuropathic Arthropathy Biomechanics
In Charcot arthropathy, the loss of protective sensation (proprioception and pain perception) combined with autonomic neuropathy (leading to increased blood flow and osteoclast activity) results in repetitive microtrauma. This leads to bone resorption, fragmentation, and joint subluxation or dislocation.
* Foot and Ankle Predominance: The foot and ankle are the most common sites due to their complex architecture and high weight-bearing demands. The midfoot is frequently affected, leading to the characteristic "rocker-bottom" deformity due to collapse of the medial longitudinal arch.
* Bone Fragility: The underlying neuropathy often coexists with metabolic changes that contribute to osteopenia and increased bone fragility, making internal fixation challenging.
* Mechanical Environment: The absence of protective reflexes allows patients to continue ambulating on unstable, damaged joints, propagating destruction. Surgical stabilization aims to create a mechanically sound construct capable of withstanding these forces.
Indications and Contraindications
The decision-making process for surgical intervention in arthritides is complex, weighing patient factors, disease severity, and potential surgical benefits against risks. It typically follows a failure of comprehensive non-operative management.
General Surgical Indications for Arthritides
- Persistent, disabling pain: Unrelieved by conservative measures, significantly impacting quality of life.
- Progressive functional impairment: Limiting activities of daily living, employment, or recreational pursuits.
- Significant joint deformity or instability: Leading to gait abnormalities, recurrent falls, or subluxation.
- Radiographic evidence of severe joint destruction: Kellgren-Lawrence Grade III or IV osteoarthritis, or progressive fragmentation/disorganization in neuropathic arthropathy.
- Specific complications: Ulceration in Charcot feet, uncontrolled infection (requiring debridement/fusion), or impending pathological fracture.
Osteoarthritis Indications
- Early/Moderate OA:
- Arthroscopy with Debridement/Chondroplasty: Limited indications, primarily for mechanical symptoms (loose bodies, meniscal tears) in early disease without significant cartilage loss. Not for diffuse OA.
- Microfracture/OATS (Osteochondral Autograft Transfer System): For contained, symptomatic full-thickness chondral defects, typically in younger patients.
- Osteotomy (e.g., High Tibial Osteotomy HTO, Distal Femoral Osteotomy DFO): For younger, active patients with unicompartmental OA and correctable varus or valgus malalignment, aiming to offload the affected compartment.
- End-Stage OA:
- Arthroplasty (Total Joint Replacement TJR/Total Knee Arthroplasty TKA, Total Hip Arthroplasty THA, Total Ankle Arthroplasty TAA): The gold standard for symptomatic, end-stage OA of major weight-bearing joints.
- Arthrodesis (Fusion): Considered for specific joints (e.g., ankle, subtalar, interphalangeal joints) where arthroplasty is not feasible or has failed, especially in younger, high-demand individuals or those with previous infection.
Neuropathic Arthropathy Indications
- Acute Charcot (Eichenholtz Stage I):
- Strict non-weight bearing (casting/bracing) is the primary treatment.
- Surgery typically reserved for unstable fractures or dislocations that threaten the skin, or gross instability that cannot be managed conservatively.
- Chronic Charcot (Eichenholtz Stage II/III):
- Exostectomy: For prominent bony prominences causing recurrent ulceration.
- Realignment Osteotomies and Fusion: For significant deformity (e.g., rocker-bottom foot), instability, or non-reducible fractures/dislocations, aiming to restore a plantigrade foot and prevent recurrent ulceration.
- Superconstructs: Employing robust internal and/or external fixation for severely unstable or comminuted deformities.
- Amputation: Salvage procedure for uncontrollable infection, severe non-reconstructible deformity, or critical limb ischemia.
General Surgical Contraindications
- Absolute Contraindications:
- Active systemic or local infection.
- Uncontrolled medical comorbidities (e.g., severe cardiac disease, poorly controlled diabetes with end-organ damage, recent myocardial infarction or stroke) that significantly increase anesthetic and surgical risk.
- Skeletal immaturity (for arthroplasty).
- Rapidly progressive neuropathic joint destruction (for arthroplasty, often a relative contraindication even for fusion).
- Relative Contraindications:
- Morbid obesity (BMI > 40 kg/m²), increasing complication rates.
- Severe vascular disease, particularly in Charcot patients, requiring revascularization prior to definitive osseous surgery.
- Lack of patient compliance with post-operative rehabilitation protocols.
- Neuropathic joint involvement (for arthroplasty).
- Severe psychiatric illness or substance abuse.
- Extensor mechanism compromise or previous extensive soft tissue damage (for TKA).
Operative versus Non-Operative Indications
| Condition | Operative Indications | Non-Operative Indications |
|---|---|---|
| Osteoarthritis (OA) | - Failure of non-operative management for > 6 months (pain, dysfunction) - Severe radiographic changes (Kellgren-Lawrence III-IV) - Progressive deformity - Specific mechanical symptoms (e.g., locked knee, symptomatic loose bodies) - Young patient with unicompartmental OA and correctable malalignment (osteotomy) |
- Mild to moderate pain controlled with analgesics - Acceptable functional status - Willingness to adhere to lifestyle modifications (weight loss, activity modification) - Successful response to physical therapy, bracing, intra-articular injections (corticosteroids, hyaluronic acid) - Early radiographic changes |
| Neuropathic Arthropathy (Charcot Joint) | - Acute instability with fracture/dislocation threatening skin integrity - Chronic, severe deformity (e.g., rocker-bottom) leading to recurrent ulceration - Non-reducible dislocation/subluxation - Osteomyelitis requiring debridement/fusion - Progressive destruction despite protected weight-bearing |
- Acute phase (Eichenholtz Stage I) managed with strict non-weight bearing immobilization (total contact cast, CAM boot) - Absence of ulceration or skin breakdown - Stable deformity amenable to accommodative bracing/custom orthotics - Successful offloading of at-risk areas - Controlled infection (for non-surgical candidates) |
Pre Operative Planning and Patient Positioning
Thorough pre-operative planning is paramount for optimizing outcomes, minimizing complications, and ensuring a safe and efficient surgical procedure.
Diagnostic Workup and Imaging
-
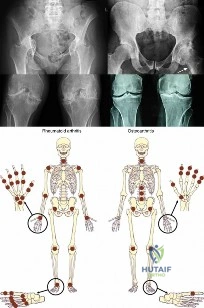
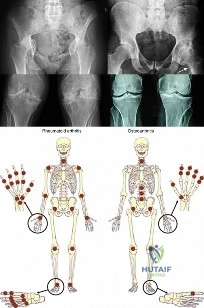
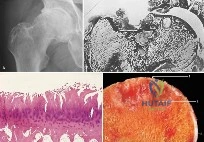
Standard Radiographs: Weight-bearing anteroposterior, lateral, and specialized views (e.g., bilateral knee Rosenberg view, hip false profile view) are essential for assessing joint space narrowing, osteophyte formation, subchondral sclerosis, cyst formation, and overall alignment. Full-length standing radiographs (hip-to-ankle alignment films) are critical for lower extremity osteotomies and arthroplasties to determine mechanical axis and guide correction.
FIG. 1.31 (A) Joint space narrowing/sclerosis. (B) Subarticular cysts in femoral head. (C) Micrograph of cartilage fissures. (D) Gross pathology of hyaline cartilage thinning.
* Magnetic Resonance Imaging (MRI): Provides detailed visualization of cartilage integrity, menisci, ligaments, synovium, and subchondral bone edema. Useful for assessing chondral defects, inflammatory changes, or pre-operative planning for osteochondral procedures.
* Computed Tomography (CT): Indicated for complex deformities, bone stock assessment (e.g., acetabular defects for THA revision), assessment of fracture nonunion, and for 3D templating, particularly useful in Charcot foot reconstruction.
* Nuclear Medicine Scans: Bone scans (Tc-99m) can differentiate acute Charcot from osteomyelitis, though they are often equivocal. PET/CT has emerging utility.
Patient Optimization
- Medical Comorbidities: Comprehensive medical evaluation by an internist or cardiologist is crucial. Optimization of diabetes control (HbA1c < 7.5% for Charcot, <8.0% for arthroplasty), hypertension, and cardiac function significantly reduces perioperative risks. Smoking cessation is non-negotiable for improving wound healing and reducing infection risk.
- Nutritional Status: Malnutrition increases surgical complications. Pre-operative nutritional assessment and supplementation may be necessary.
- Weight Management: Significant weight loss can reduce mechanical stress on joints and improve surgical outcomes, particularly for lower extremity arthroplasty.
- Anemia Correction: Pre-operative anemia should be corrected to minimize the need for blood transfusions.
- Dental Clearance: Required prior to arthroplasty to minimize the risk of hematogenous infection.
Pre-operative Templating
- Arthroplasty: Critical for determining implant size, position, and restoration of limb alignment, length, and offset. Digital templating software, used with calibrated radiographs, allows for precise planning of component orientation, osteotomy levels, and anticipated leg length changes.
- Osteotomy: Planning involves drawing correction angles and identifying the optimal level of osteotomy to achieve desired mechanical axis realignment.
- Charcot Reconstruction: Detailed planning of osteotomy levels, amount of bone resection, and selection of appropriate implants (plates, screws, intramedullary nails, external fixators) is essential due to challenging bone quality and significant deformity.
Surgical Site Preparation
- Antibiotic Prophylaxis: Administered typically within 60 minutes of incision, tailored to local resistance patterns (e.g., Cefazolin). For patients with allergies, alternatives like Clindamycin or Vancomycin are used.
- Skin Preparation: Meticulous skin preparation using chlorhexidine-alcohol or povidone-iodine solutions is vital.
- Tourniquet: Commonly used for distal extremity surgery (knee, ankle, foot) to provide a bloodless field, typically inflated to 100-150 mmHg above systolic blood pressure.
Patient Positioning
Proper patient positioning is critical for surgical access, safety, and anesthetic management.
* Total Hip Arthroplasty (THA):
* Lateral Decubitus: Common for posterior and direct lateral approaches. Requires careful padding of bony prominences, axillary roll, and beanbag stabilization.
* Supine: Used for anterior approaches (direct anterior, anterolateral). A specialized surgical table (e.g., fracture table) may be used for specific anterior approaches to facilitate limb manipulation and traction.
* Total Knee Arthroplasty (TKA):
* Supine: With a bump under the ipsilateral hip to allow leg rotation and a bump under the ankle to facilitate knee flexion.
* Total Ankle Arthroplasty (TAA) / Foot & Ankle Fusion:
* Supine: Often with a bolster under the ipsilateral hip and foot of the bed dropped. A tourniquet is essential.
* Charcot Foot Reconstruction:
* Supine: Positioned to allow maximal access to the foot and ankle, often with external fixation requiring specific positioning frames or bolsters. Fluoroscopy must be readily available.
Detailed Surgical Approach and Technique
The surgical management of arthritides spans a spectrum from arthroscopic debridement to complex reconstructive arthroplasty or arthrodesis. This section details common operative techniques for managing osteoarthritis and neuropathic arthropathy.
Surgical Management of Osteoarthritis
Arthroscopy and Chondral Procedures
- Diagnostic Arthroscopy: Allows direct visualization of articular surfaces, menisci, and ligaments.
- Chondroplasty/Debridement: Arthroscopic removal of unstable cartilage flaps and loose bodies. While it can provide temporary symptom relief, it does not alter the natural history of diffuse OA.
- Microfracture: Induces bone marrow stimulation for repair cartilage (fibrocartilage) formation in contained full-thickness chondral defects (<2-4 cm²), typically in younger patients. Technique involves perforating the subchondral bone plate.
- Osteochondral Autograft Transfer System (OATS): Involves harvesting osteochondral plugs from a less weight-bearing area and transplanting them to a defect. Indicated for larger, contained defects.
- Autologous Chondrocyte Implantation (ACI): A two-stage procedure where chondrocytes are harvested, expanded in vitro, and reimplanted under a periosteal flap or matrix (MACI). Reserved for specific indications in younger patients.
Corrective Osteotomies
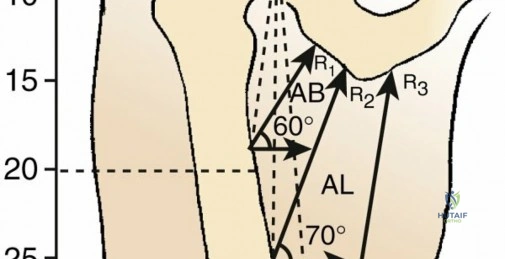
- High Tibial Osteotomy (HTO): For medial compartment knee OA with varus malalignment.
- Planning: Full-length standing radiographs to determine mechanical axis deviation and desired correction angle. Templating guides the wedge size (opening or closing) and osteotomy level.
- Approach: Medial approach, protecting the saphenous nerve and artery.
- Technique (Opening Wedge): A medial cortical cut is made proximally on the tibia, extending laterally towards the fibular head, stopping short of the lateral cortex to preserve the hinge. The wedge is opened to the pre-determined angle and stabilized with a plate and screws, often with bone graft or substitute.
- Distal Femoral Osteotomy (DFO): For lateral compartment knee OA with valgus malalignment.
- Planning: Similar to HTO, with precise angle calculation.
- Approach: Lateral approach, protecting the common peroneal nerve.
- Technique (Closing Wedge): A lateral wedge of bone is resected, and the osteotomy is closed and stabilized with a plate.
Arthroplasty Total Joint Replacement
-
Total Hip Arthroplasty (THA):
- Approaches:
- Posterior Approach: Most common, excellent exposure, preserves abductors. Internervous plane between gluteus maximus (inferior gluteal nerve) and gluteus medius/minimus (superior gluteal nerve). Risks posterior dislocation.
- Direct Anterior Approach: Muscle-sparing (between sartorius/rectus femoris and tensor fascia lata/gluteus medius). Reduced dislocation risk but steeper learning curve and potential for lateral femoral cutaneous nerve injury.
- Direct Lateral/Anterolateral Approach: Involves detaching/splitting the gluteus medius. Less dislocation risk but can lead to abductor weakness.
- Technique: Femoral head resection, acetabular reaming, implanting a press-fit or cemented acetabular component, femoral canal reaming, implanting a press-fit or cemented femoral stem, and articulation with a modular femoral head and liner. Careful attention to limb length, offset, and component orientation.
- Approaches:
-
Total Knee Arthroplasty (TKA):
- Approach: Medial parapatellar approach, eversion of patella.
- Technique: Meticulous bone cuts using cutting blocks (distal femur, proximal tibia, patella). Ligamentous balancing (flexion and extension gaps) to achieve symmetric stability and proper component alignment. Implanting cemented or cementless femoral, tibial, and patellar components.
- Total Ankle Arthroplasty (TAA):
- Approach: Anterior approach, often requiring retraction or tenotomy of the extensor hallucis longus and anterior tibialis tendon. Careful neurovascular bundle protection.
- Technique: Resection of distal tibia and talar dome. Component implantation with precise alignment to restore mechanical axis and kinematics.
Arthrodesis (Fusion)
- Indications: For painful, unstable joints where arthroplasty is contraindicated or has failed (e.g., severe bone loss, chronic infection, young active patient).
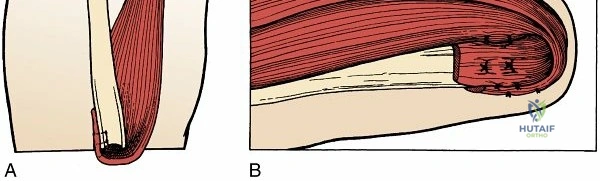
- Technique: Resection of articular cartilage and sclerotic bone to expose cancellous bone. Shaping joint surfaces for maximal contact. Compression with internal fixation (screws, plates, intramedullary nails). Bone grafting (autograft or allograft) may be used to enhance fusion rates.
Surgical Management of Neuropathic Arthropathy (Charcot Joint)
Surgical reconstruction for Charcot arthropathy is complex, requiring robust fixation and a multidisciplinary approach due to challenging bone quality, soft tissue issues, and high infection rates.
Exostectomy and Debridement
- Indications: For prominent bony deformities that cause chronic skin ulceration, risking osteomyelitis.
- Technique: Careful soft tissue dissection to expose the exostosis. Resection of bone using osteotomes or burrs until the pressure point is relieved and the foot is plantigrade. Meticulous wound closure.
Realignment Osteotomies and Fusion
- Indications: For gross instability, severe rocker-bottom deformity, or non-unions that cannot be managed with orthoses, especially if associated with ulceration or impending skin breakdown.
- Planning: Extensive pre-operative CT imaging for 3D understanding of deformity and bone stock. Detailed templating of osteotomy cuts, correction angles, and fixation strategies.
- Approach: Tailored to the deformity (e.g., medial approach for midfoot collapse, lateral approach for hindfoot valgus). Wide exposure to identify and resect necrotic or sclerotic bone.
- Technique:
- Resection: Removal of prominent bone, non-viable tissue, and often a wedge osteotomy to correct the deformity (e.g., dorsomedial wedge for rocker-bottom).
- Reduction: Realignment of the foot to a plantigrade position.
- Fixation: High-strength, stable internal fixation is crucial. This often involves:
- Large Diameter Screws: For robust interfragmentary compression.
- Locked Plating Systems: Providing strong angular stability.
- Intramedullary Nailing: Particularly effective for hindfoot and ankle fusions, providing axial stability across multiple joints.
- External Fixation: Often used in conjunction with internal fixation (hybrid constructs) or as a primary method for severe deformity, soft tissue compromise, or infected cases.
- Bone Grafting: Autograft or allograft is often used to enhance fusion due to poor bone healing potential in these patients.
Superconstructs
- Concept: Utilizes multiple fixation methods (e.g., plates, screws, intramedullary rods) and extends fixation well beyond the reconstruction site into healthy bone segments to distribute stress and enhance stability, particularly in complex Charcot reconstructions. This is critical given the poor bone quality and high loads.
Complications and Management
Surgical intervention for arthritides, while often providing significant relief, carries inherent risks. Understanding common complications and developing robust management strategies is essential for orthopedic practice.
General Surgical Complications
- Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE): Incidence varies with procedure and patient factors. Prophylaxis (mechanical and/or chemical) is standard. Management involves anticoagulation for DVT, thrombolysis or embolectomy for PE.
- Infection: A devastating complication, particularly in arthroplasty and Charcot. Prophylactic antibiotics, meticulous aseptic technique, and optimization of patient factors are crucial. Management ranges from debridement and retention to component removal (Girdlestone arthroplasty, two-stage revision) or amputation.
- Neurovascular Injury: Direct trauma or stretch injury to nerves (e.g., common peroneal nerve in TKA, sciatic nerve in THA) or vessels. Careful surgical dissection and knowledge of anatomy are key. Management may involve observation, nerve repair, or vascular repair.
- Anesthetic Complications: Related to general or regional anesthesia, including cardiac events, respiratory compromise, allergic reactions.
Osteoarthritis Surgical Complications
Arthroplasty Specific Complications
- Periprosthetic Joint Infection (PJI): Incidence 0.5-2%. Managed with surgical debridement and retention (DAIR) in acute cases, or two-stage revision (implant removal, spacer, delayed reimplantation) for chronic infections.
- Aseptic Loosening: Mechanical failure of the implant-bone interface without infection. Incidence increases over time. Managed by revision arthroplasty.
- Periprosthetic Fracture: Fracture occurring around the implant. Management depends on fracture location, stability, and implant stability, ranging from non-operative treatment to ORIF or revision arthroplasty.
- Dislocation (THA): Incidence 1-5%, higher with certain approaches. Managed by closed reduction, but recurrent dislocations may require revision.
- Polyethylene Wear: Degradation of the plastic bearing surface, leading to osteolysis and aseptic loosening. Managed by liner exchange or revision arthroplasty.
- Nerve Palsy: Post-operative nerve injury, often temporary. Observation, nerve conduction studies, or neurolysis may be required.
- Heterotopic Ossification (HO): Ectopic bone formation around the joint. Prophylaxis with NSAIDs or radiation. Symptomatic HO may require excision.
- Persistent Pain: Can be multifactorial (component malposition, infection, neuropathic pain, soft tissue impingement). Thorough workup is required.

Osteotomy Specific Complications
- Nonunion/Malunion: Failure of the osteotomy to heal or healing in an incorrect position. Incidence can be 5-15%. Managed by revision osteotomy with grafting and more rigid fixation.
- Hardware Failure: Plate or screw breakage. Often associated with nonunion.
- Delayed Healing/Pseudarthrosis: Prolonged healing time.
- Nerve/Vascular Injury: Specific to the region of osteotomy.
Neuropathic Arthropathy Surgical Complications
These are often higher than for routine arthroplasty due to poor bone quality, soft tissue compromise, and patient comorbidities.
* Surgical Site Infection (SSI) / Osteomyelitis: Incidence can be >20%. Aggressive debridement, targeted antibiotics, and staged reconstruction are often necessary. Amputation may be required for uncontrolled infection.
* Nonunion/Malunion: Fusion rates are lower than in non-neuropathic patients. Re-operation with further debridement, grafting, and revision fixation may be needed.
* Hardware Failure: High loads on fragile bone lead to higher rates of screw pullout, plate breakage, or loss of reduction. Revision with stronger constructs (e.g., superconstructs, IM nails) is common.
* Recurrence of Deformity: Despite successful initial correction, the underlying neuropathy and biomechanical stresses can lead to new or recurrent deformity. Requires continued orthotic management and potential re-operation.
* Amputation: The ultimate salvage procedure for intractable infection, non-reconstructible deformity, or critical limb ischemia.
Common Complications, Incidence, and Salvage Strategies
| Complication | Typical Incidence (Approx.) | Salvage Strategy |
|---|---|---|
| Periprosthetic Joint Infection (PJI) (Arthroplasty) | 0.5-2% | - Acute: Irrigation & debridement with component retention (DAIR) and antibiotics - Chronic: Two-stage revision arthroplasty (explantation, antibiotic spacer, delayed reimplantation) or one-stage revision in select cases. Girdlestone or amputation for failed revisions. |
| Aseptic Loosening (Arthroplasty) | 5-10% at 10 years | Revision arthroplasty with cementless or cemented components, potentially using augments or structural grafts for bone loss. |
| Periprosthetic Fracture (Arthroplasty) | 0.3-2% | - Stable implant: ORIF with plates/screws - Unstable implant: Revision arthroplasty (stem/cup) with fixation of fracture. |
| Dislocation (THA) | 1-5% | - Closed reduction and bracing - Recurrent: Revision arthroplasty (component repositioning, constrained liner, larger femoral head) or constrained cup. |
| Nerve Injury | 1-2% (e.g., peroneal, sciatic, LFCN) | - Observation, non-steroidal anti-inflammatory drugs (NSAIDs) - Nerve conduction studies - Surgical exploration and neurolysis/repair for persistent deficits. |
| DVT/PE | DVT: 0.5-5%; PE: 0.1-1% | - DVT: Anticoagulation (LMWH, oral anticoagulants) - PE: Anticoagulation, thrombolysis, embolectomy, IVC filter. |
| Nonunion/Malunion (Osteotomy/Charcot Fusion) | 5-15% | - Revision surgery: Re-osteotomy/re-fusion with bone grafting (autograft/allograft) and more rigid internal fixation (plates, screws, IM nails, external fixation). Bone stimulators. |
| Hardware Failure (Osteotomy/Charcot) | 5-10% | - Associated with nonunion: Revision osteotomy/fusion with stronger fixation and bone grafting. - Isolated hardware failure: May require hardware removal. |
| Surgical Site Infection (Charcot Reconstruction) | 10-30% | - Aggressive surgical debridement, cultures, targeted IV antibiotics - staged reconstruction - Amputation for uncontrolled infection. |
| Recurrence of Deformity (Charcot) | 10-20% | - Custom orthotics/bracing - Revision surgery: Further osteotomies, fusion, or complex reconstruction with superconstructs. |
Post Operative Rehabilitation Protocols
Effective post-operative rehabilitation is as crucial as the surgical procedure itself in restoring function, preventing complications, and optimizing long-term outcomes for patients undergoing surgery for arthritides. Protocols are tailored to the specific procedure, joint, and patient's baseline health.
General Principles
- Pain Management: Multimodal analgesia (NSAIDs, acetaminophen, opioids, regional blocks) is employed to facilitate early mobilization.
- Wound Care: Meticulous dressing changes, monitoring for signs of infection (erythema, warmth, purulence), and timely suture/staple removal.
- Deep Vein Thrombosis Prophylaxis: Continued post-operatively with mechanical (sequential compression devices) and/or chemical (anticoagulants) methods as per institutional guidelines.
- Patient Education: Crucial for compliance with weight-bearing restrictions, exercise regimens, and recognizing warning signs.
Osteoarthritis Rehabilitation
Arthroplasty (Total Hip, Knee, Ankle Replacement)
- Phase I: Hospital Stay (Days 0-5):
- Goals: Early mobilization, pain control, independent transfers, achieving initial range of motion (ROM) goals.
- Hip: Immediately weight-bearing as tolerated (WBAT), unless specified. Hip precautions (e.g., no hip flexion >90 degrees, no adduction past midline, no internal rotation for posterior approach) depending on surgical approach and surgeon preference. Focus on quad and gluteal activation.
- Knee: Continuous Passive Motion (CPM) machine may be used, though its benefit is debated. Early weight-bearing (WBAT) with assistive devices. ROM goals (0-90 degrees flexion by discharge). Quad sets, ankle pumps.
- Ankle: Non-weight bearing (NWB) or touch-down weight-bearing (TDWB) in a splint or boot for several weeks, then progressive weight-bearing. Gentle ankle ROM.
- Phase II: Home/Outpatient Rehabilitation (Weeks 1-12):
- Goals: Progressive ROM, strengthening, gait training, return to functional activities.
- Hip/Knee: Gradual weaning from assistive devices. Progressive resistance exercises for major muscle groups around the joint. Proprioceptive training. Progression to light impact activities.
- Ankle: Gradually increase weight-bearing. Strengthening of dorsiflexors and plantarflexors. Balance and proprioception exercises.
- Phase III: Advanced Rehabilitation/Return to Activity (Months 3+):
- Goals: Restoration of maximal strength, endurance, and agility for desired activities.
- Emphasis on sport-specific training or high-level functional tasks. Avoid high-impact activities for arthroplasty to minimize wear.
Osteotomy (HTO, DFO)
- Initial Immobilization: Often cast or brace for 4-6 weeks to protect the osteotomy site.
- Weight-Bearing: Touch-down or partial weight-bearing (PWB) for 6-12 weeks, with gradual progression based on radiographic evidence of healing.
- Range of Motion: Initiated cautiously, often delayed compared to arthroplasty, to protect the healing bone.
- Strengthening: Gradual, progressive strengthening exercises, avoiding excessive torque across the osteotomy.
- Return to Activity: Typically slower than arthroplasty, with full return to sports or heavy labor often taking 6-12 months.
Arthroscopy and Chondral Procedures
- Weight-Bearing: Varies. May be NWB or PWB for 4-6 weeks for microfracture or OATS. WBAT for simple debridement.
- Range of Motion: Early, controlled ROM is typically encouraged to prevent stiffness and facilitate cartilage healing.
- Strengthening: Progressive strengthening exercises once pain and swelling subside.
Neuropathic Arthropathy Rehabilitation (Charcot Reconstruction)
Rehabilitation following Charcot reconstruction is characterized by prolonged immobilization and protected weight-bearing due to compromised bone healing and soft tissue fragility.
* Phase I: Prolonged Non-Weight Bearing (NWB) (3-6+ months):
* Immobilization: Rigid cast or custom-molded orthosis, often extending above the knee for hindfoot/ankle fusions. External fixation may be in place.
* Strict NWB: Absolutely critical to allow osseous consolidation. Use of crutches, walker, or wheelchair.
* Wound Care: Meticulous wound checks, especially if external fixators are present (pin site care).
* Monitoring: Regular clinical and radiographic follow-up to assess healing and detect early complications (e.g., loss of reduction, infection).
* Phase II: Progressive Protected Weight-Bearing (6-12+ months):
* Goals: Gradual transition to weight-bearing, customized orthotic fitting.
* Weight-Bearing: Progress from TDWB to PWB in a custom Charcot brace (CROW – Charcot Restraint Orthotic Walker) or custom-molded shoe with orthosis.
* Bracing: Lifelong accommodative bracing is often required to protect the reconstructed foot and prevent recurrence of deformity or ulceration.
* Ulcer Prevention: Daily foot inspection, meticulous skin care, and offloading strategies are paramount.
* Phase III: Long-Term Management:
* Goals: Maintenance of a stable, plantigrade foot; prevention of ulceration; accommodation for residual deficits.
* Regular follow-up with orthopedic surgeon and podiatrist for ongoing foot health surveillance.
Summary of Key Literature and Guidelines
The management of arthritides, particularly OA, is guided by robust evidence and consensus guidelines from major orthopedic and rheumatologic societies. Neuropathic arthropathy, while less common, also has evolving evidence-based treatment algorithms.
Osteoarthritis Management Guidelines
- American Academy of Orthopaedic Surgeons (AAOS): Provides clinical practice guidelines for various joint-specific OA, emphasizing non-operative treatment modalities (weight management, exercise, NSAIDs, intra-articular injections) as first-line. Surgical recommendations are typically for patients failing conservative care, with arthroplasty as the definitive treatment for end-stage disease.
- Osteoarthritis Research Society International (OARSI): Publishes comprehensive guidelines for OA management, categorizing recommendations by joint, disease severity, and patient comorbidities. OARSI emphasizes a multimodal approach, integrating pharmacological, non-pharmacological, and surgical interventions. Recent updates highlight the role of individualized treatment plans and shared decision-making.
- European League Against Rheumatism (EULAR): Similar to OARSI, EULAR provides evidence-based recommendations for the diagnosis and management of OA, often with a focus on early intervention and the role of biologics in specific inflammatory subsets (though less prominent in pure OA).
Key Literature in OA Surgical Management
- Efficacy of Arthroplasty: Numerous long-term studies and national joint registries consistently demonstrate the efficacy of TKA and THA in providing significant pain relief, functional improvement, and high patient satisfaction rates (often >90%) in appropriately selected patients with end-stage OA. Survival rates for modern prostheses are excellent, with 10-15 year survival often exceeding 90-95%.
- Osteotomy Outcomes: Long-term follow-up studies for HTO indicate good to excellent results in younger, active patients with unicompartmental varus OA, with implant survival ranging from 60-80% at 10 years, often delaying the need for TKA. Patient selection for osteotomy remains critical.
- Arthroscopic Debridement: Systematic reviews and randomized controlled trials have largely refuted the broad utility of arthroscopic debridement and lavage for symptomatic knee OA, demonstrating no significant long-term benefit over non-operative treatment. Its role is primarily limited to mechanical symptoms (e.g., loose bodies, meniscal tears) in specific settings.
Neuropathic Arthropathy Management Guidelines
- Consensus Guidelines: Recommendations for Charcot foot management are often derived from multidisciplinary expert consensus rather than large-scale randomized trials, reflecting the rarity and complexity of the condition. Guidelines emphasize a staged approach:
- Early Diagnosis and Immobilization: Aggressive non-weight bearing immobilization (total contact casting) is the cornerstone for acute Charcot.
- Deformity Management: Surgical intervention is indicated for unstable deformities, those leading to ulceration, or non-reducible dislocations.
- Post-operative Management: Prolonged non-weight bearing, robust fixation strategies, and lifelong custom bracing are crucial.
- Key Literature in Charcot Reconstruction: Literature largely consists of retrospective case series and expert reviews. These highlight:
- High Surgical Risk: High rates of infection, nonunion, and hardware failure, emphasizing the need for patient optimization and aggressive surgical techniques (e.g., superconstructs, intramedullary nailing).
- Importance of External Fixation: Often used in conjunction with internal fixation or as a primary method in complex cases with significant soft tissue compromise or infection.
- Multidisciplinary Team: The critical role of endocrinologists, infectious disease specialists, podiatrists, and wound care specialists is repeatedly emphasized for successful outcomes.
Future Directions
Research in arthritides continues to evolve. In OA, focus areas include cartilage regeneration strategies (stem cells, gene therapy, biomaterials), targeting inflammatory pathways to slow progression, and advanced imaging for early diagnosis. For Charcot arthropathy, improved implant designs for compromised bone, biological adjuncts to enhance fusion, and better risk stratification tools remain active areas of investigation. Robotic-assisted surgery and navigation continue to improve precision and potentially outcomes in arthroplasty procedures.
Clinical & Radiographic Imaging

Detailed Chapters & Topics
Dive deeper into specialized chapters regarding arthritides