Operative Management of Osteoarthritis: A Comprehensive Surgical Guide
Key Takeaway
Osteoarthritis represents a complex biomechanical and biological destabilization of articular cartilage and subchondral bone. This comprehensive guide explores evidence-based operative interventions, ranging from arthroscopic debridement and marrow stimulation to corrective osteotomies and total joint arthroplasty. Designed for orthopedic surgeons, it details step-by-step surgical techniques, patient positioning, biomechanical principles, and postoperative rehabilitation protocols to optimize clinical outcomes in degenerative joint disease.
Comprehensive Introduction and Patho-Epidemiology
Osteoarthritis (OA) represents the clinical and pathological endpoint of a multifactorial cascade involving mechanical, biological, and genetic events that systematically dismantle the homeostatic equilibrium of articular joints. Unlike a simple "wear and tear" phenomenon, OA is a metabolically active, dynamically progressive disease characterized by the profound destabilization of degradation and synthesis within the articular cartilage, subchondral bone, and synovial tissues. At the cellular level, the pathogenesis initiates with chondrocyte hypertrophy and apoptosis, leading to an insidious alteration in the extracellular matrix (ECM). This is marked pathognomonically by an initial, paradoxical increase in cartilage water content, followed by a precipitous decline in proteoglycan concentration and structural disorganization of the type II collagen fibril network. This biochemical degradation is heavily mediated by the upregulation of matrix metalloproteinases (specifically MMP-1, MMP-3, and MMP-13) and aggrecanases (ADAMTS-4 and ADAMTS-5), driven by pro-inflammatory cytokines such as Interleukin-1 beta (IL-1β) and Tumor Necrosis Factor-alpha (TNF-α). The resultant catabolic environment ultimately yields irreversible structural deterioration, subchondral sclerosis, and osteophyte formation.
Clinically and etiologically, osteoarthritis is bifurcated into primary and secondary classifications, each demanding distinct diagnostic and therapeutic algorithms. Primary osteoarthritis generally manifests as an idiopathic, polyarticular degenerative arthropathy. It is intrinsically linked to genetic predispositions, advancing age (rarely presenting before the age of 35, but exponentially prevalent in the demographic over 50), and metabolic syndromes. The progression of primary OA is characteristically insidious, slow, and relentless. It exhibits a profound epidemiological correlation with obesity, particularly in weight-bearing articulations such as the knee and hip, where the mechanical overload exponentially accelerates ECM degradation. Furthermore, occupational hazards necessitating repetitive axial loading, heavy lifting, and elite-level sporting activities have been statistically validated as significant risk factors for the premature onset of primary OA, particularly in the coxofemoral joint.
Conversely, secondary osteoarthritis typically presents as a monoarticular phenomenon, arising as a direct, mechanically driven reaction of the joint to a pre-existing pathological condition that has induced articular incongruity or instability. The etiologies of secondary OA are vast and include traumatic mechanical derangements (e.g., neglected anterior cruciate ligament tears, meniscectomies), pyogenic joint infections leading to chondrolysis, congenital anomalies such as developmental dysplasia of the hip (DDH) or slipped capital femoral epiphysis (SCFE), chronic ligamentous laxity, and malunited intra-articular fractures. The prognosis for secondary osteoarthritis is often significantly less favorable than its primary counterpart. The localized, severe mechanical deficits inherent to secondary OA create focal areas of extreme contact stress, rapidly accelerating joint destruction and often necessitating operative intervention at a much earlier chronological age.
The epidemiological burden of osteoarthritis is staggering, representing one of the leading causes of global disability. As the population ages and the prevalence of obesity continues to rise, the economic impact—encompassing direct surgical costs, prolonged rehabilitation, and lost workforce productivity—has reached astronomical levels. Consequently, the operative management of osteoarthritis has evolved dramatically over the past three decades. The paradigm has shifted from palliative procedures, such as isolated arthroscopic debridement, toward sophisticated joint preservation techniques (e.g., corrective osteotomies, autologous chondrocyte implantation) for younger demographics, and highly advanced, kinematically aligned arthroplasty solutions for end-stage disease. Understanding the nuanced patho-epidemiology of OA is paramount for the orthopedic surgeon, as it directly dictates the timing, modality, and ultimate success of surgical intervention.
Detailed Surgical Anatomy and Biomechanics
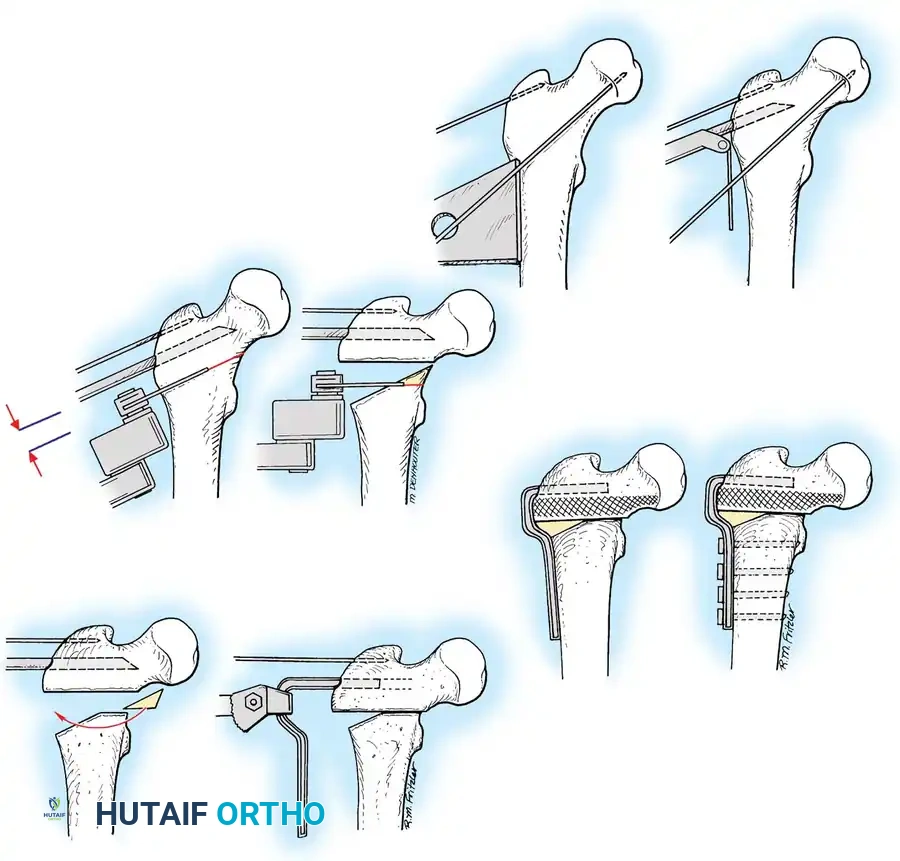
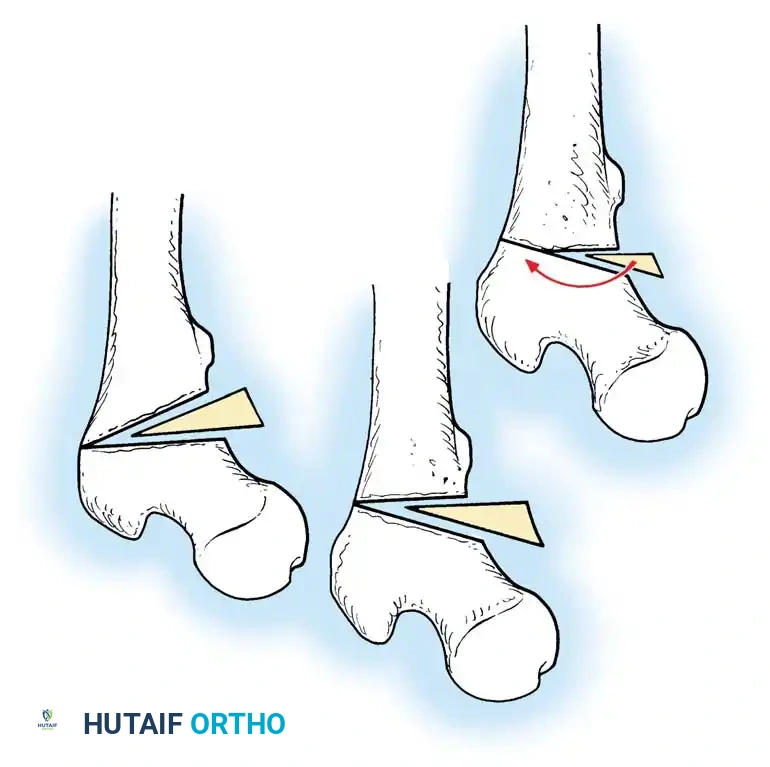
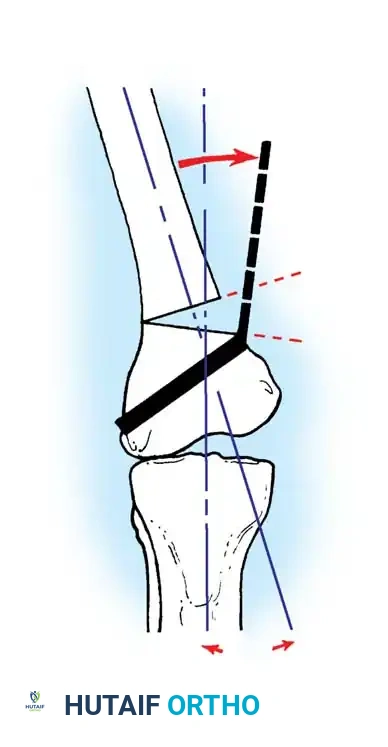
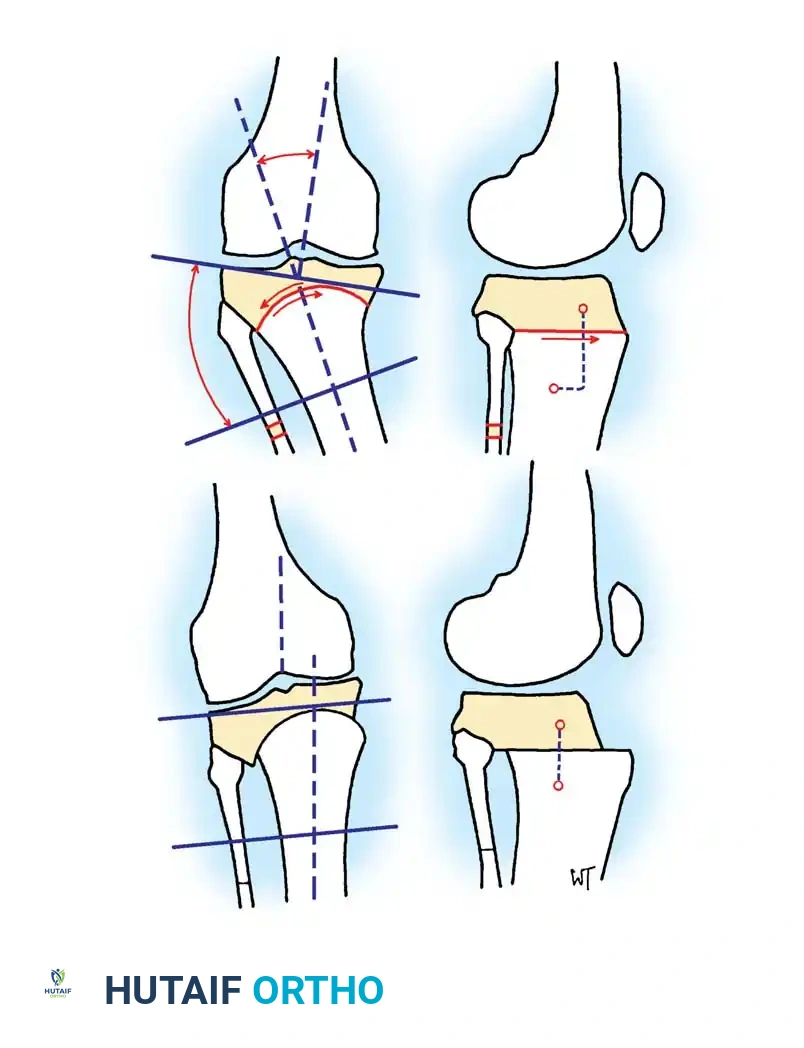
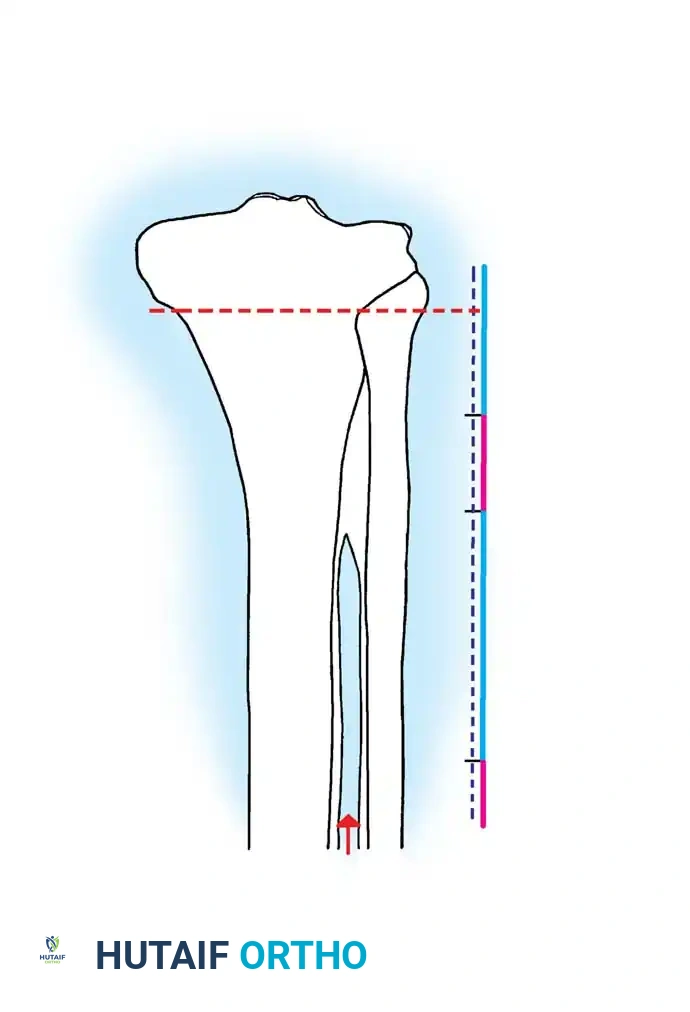
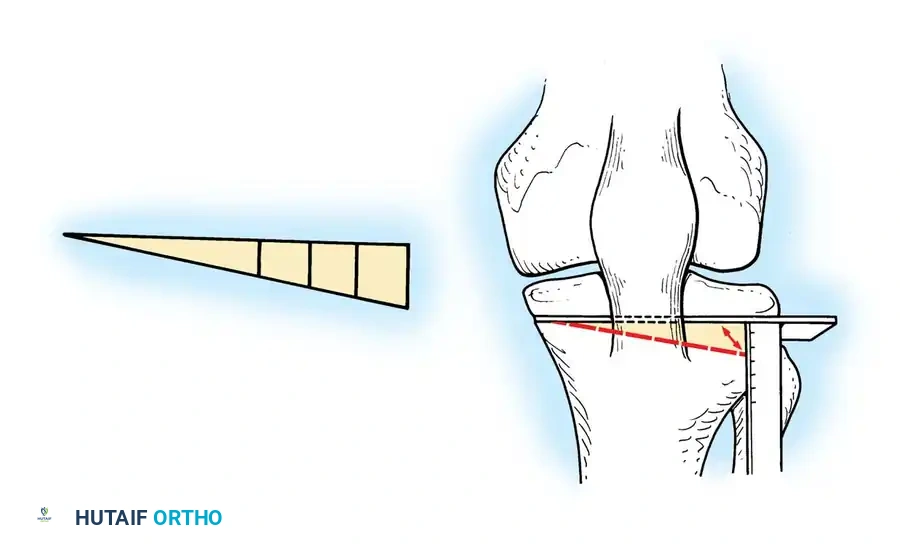
A profound mastery of joint biomechanics and surgical anatomy is the absolute prerequisite for the successful operative management of osteoarthritis. In the lower extremity, particularly the knee, the concept of the mechanical axis is foundational. The mechanical axis of the lower limb is defined by a line drawn from the center of the femoral head to the center of the ankle mortise. In a neutrally aligned knee, this weight-bearing line (WBL) passes precisely through the center of the knee joint, distributing approximately 60% of the axial load to the medial compartment and 40% to the lateral compartment. This baseline asymmetry explains the higher prevalence of medial compartment osteoarthritis. When varus malalignment occurs, the WBL shifts medially, exponentially increasing the contact pressures on the medial articular cartilage and meniscus, creating a vicious cycle of cartilage loss, progressive varus deformity, and lateral ligamentous stretching (varus thrust). Corrective osteotomies aim to manipulate this axis, shifting the WBL to the "Fujisawa point"—typically located at 62% of the tibial plateau width from the medial edge—to decompress the diseased medial compartment and transfer loads to the preserved lateral compartment.
The menisci and ligamentous stabilizers play an equally critical role in the biomechanical milieu of the knee. The medial and lateral menisci are vital for load transmission, shock absorption, and secondary joint stability. They function by converting axial compressive forces into circumferential "hoop stresses." Iatrogenic disruption of the peripheral meniscal rim or the meniscal roots during arthroscopy effectively nullifies these hoop stresses, biomechanically equating to a total meniscectomy and ensuring rapid osteoarthritic progression. Furthermore, the superficial medial collateral ligament (sMCL) is a crucial anatomical landmark during medial opening wedge high tibial osteotomies (HTO). The sMCL must be meticulously identified and partially released distally (coronal plane balancing) to allow the osteotomy to hinge open without inadvertently increasing the contact pressures within the medial compartment, which would defeat the purpose of the realignment procedure.


In the upper extremity, the elbow presents a unique biomechanical challenge as a highly constrained, non-weight-bearing hinge joint that is nonetheless highly susceptible to degenerative and inflammatory arthropathies. The articulation consists of the ulnohumeral joint (primary hinge) and the radiocapitellar joint (pronation/supination and secondary valgus stabilizer). During procedures such as radial head excision and synovectomy, the surgeon must possess an intimate knowledge of the lateral collateral ligamentous complex. The lateral ulnar collateral ligament (LUCL), which originates on the lateral epicondyle and inserts on the supinator crest of the ulna, is the primary restraint to posterolateral rotatory instability (PLRI). Iatrogenic transection of the LUCL during a Kocher approach is a devastating complication. Furthermore, the ulnar nerve, coursing through the cubital tunnel posterior to the medial epicondyle, is at extreme risk during total elbow arthroplasty (TEA). The nerve's vascular supply and delicate epineurium must be preserved during mandatory transposition to prevent severe postoperative neuropathy.
The foot and ankle complex represents a marvel of static and dynamic biomechanics, designed to transition seamlessly from a flexible shock absorber at heel strike to a rigid lever arm at toe-off. Osteoarthritis in this region frequently involves the first metatarsophalangeal (MTP) joint (hallux rigidus), the subtalar joint, or the transverse tarsal joints. The biomechanics of the first MTP joint require a complex sliding and rolling motion; dorsal osteophytes (cheilectomy targets) mechanically block the crucial windlass mechanism of the plantar fascia. In the hindfoot, the subtalar joint acts as a torque converter, translating tibial internal/external rotation into foot pronation/supination. Arthrodesis of the subtalar or triple joint complex eliminates this motion, drastically altering the kinematics of the adjacent ankle and midfoot joints, thereby predisposing them to adjacent segment disease. Surgical planning must therefore meticulously balance the need for pain relief through fusion with the imperative to maintain a plantigrade, biomechanically viable foot.
Exhaustive Indications and Contraindications
The decision-making algorithm for the operative management of osteoarthritis is highly complex, requiring the synthesis of the patient’s chronological and physiological age, functional demands, body mass index (BMI), and the precise radiographic severity of the disease (e.g., Kellgren-Lawrence grading). The primary indication for any surgical intervention is recalcitrant pain and functional disability that has comprehensively failed an exhaustive trial of non-operative modalities. These non-operative measures must include targeted physical therapy focusing on dynamic joint stabilizers, judicious use of NSAIDs, unloader orthoses, and intra-articular therapeutics (corticosteroids, hyaluronic acid, or orthobiologics). Only when the patient exhibits persistent mechanical symptoms, rest pain, or progressive deformity that significantly impairs their activities of daily living should operative pathways be considered.
Joint preservation techniques, such as High Tibial Osteotomy (HTO), Distal Femoral Osteotomy (DFO), and advanced cartilage restoration (Autologous Chondrocyte Implantation, Osteochondral Allografts), possess strict, narrow indications. The ideal candidate for a corrective osteotomy is a young (typically under 60 years of age), active, non-obese patient suffering from isolated unicompartmental osteoarthritis (usually medial) driven by a distinct mechanical malalignment (varus deformity). Crucially, the contralateral compartment and the patellofemoral joint must be radiographically and clinically preserved, as the procedure will inherently transfer increased load to these areas. Furthermore, the patient must possess a stable ligamentous envelope; while a concomitant ACL reconstruction can be performed simultaneously with an HTO to address sagittal instability and varus thrust, severe, uncorrectable multidirectional instability remains a relative contraindication.

Contraindications for joint preservation are absolute and must be rigorously respected to prevent catastrophic early failure. Absolute contraindications include the presence of inflammatory arthropathies (e.g., Rheumatoid Arthritis), severe tricompartmental disease, and restricted range of motion (specifically a flexion contracture exceeding 15 degrees or flexion less than 90 degrees). Morbid obesity (BMI > 35) is a strong relative, if not absolute, contraindication, as the excessive axial loads will rapidly overwhelm the fixation constructs and the newly loaded "healthy" compartment. Active infection, severe peripheral vascular disease, and an inability to comply with strict, prolonged non-weight-bearing postoperative protocols also preclude patients from these advanced joint-preserving operations.
When joint preservation is contraindicated or the disease has progressed to end-stage, arthroplasty (Unicompartmental, Total Knee, or Total Elbow) becomes the definitive indication. Total joint arthroplasty is indicated for patients with severe, bone-on-bone tricompartmental OA, inflammatory arthritis, or failed previous osteotomies, who demand predictable pain relief and restoration of basic functional mobility. In the elbow, Total Elbow Arthroplasty (TEA) is primarily indicated for advanced rheumatoid arthritis, post-traumatic OA in the elderly, or distal humeral nonunions where internal fixation is impossible. However, TEA is strictly contraindicated in young, high-demand patients or laborers due to the permanent lifelong lifting restrictions (typically 5-10 lbs) required to prevent aseptic loosening and catastrophic catastrophic implant failure.
| Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| High Tibial Osteotomy (HTO) | Unicompartmental medial OA, Varus malalignment, Age < 60, Active lifestyle | Inflammatory arthritis, Tricompartmental OA, Flexion contracture > 15°, Restricted ROM (<90° flexion) | Morbid obesity (BMI > 35), Patellofemoral severe OA, Smoking |
| Distal Femoral Osteotomy (DFO) | Unicompartmental lateral OA, Valgus malalignment, Joint line > 10° oblique | Inflammatory arthritis, Medial compartment OA, Severe ligamentous instability | Obesity, Advanced age, Poor bone stock |
| Autologous Chondrocyte Implantation (ACI) | Focal, symptomatic full-thickness chondral defects (Outerbridge IV), Size > 2cm², Femoral condyle | Diffuse OA, Malalignment (unless corrected concurrently), Kissing lesions | Patellofemoral lesions (lower success rates), Age > 55 |
| Total Elbow Arthroplasty (TEA) | End-stage RA, Post-traumatic OA in low-demand elderly, Distal humerus nonunion | Active infection, Young/high-demand laborers, Charcot arthropathy | Poor soft tissue envelope, Prior triceps avulsion |
| Arthroscopic Debridement | Mechanical symptoms (catching/locking), Unstable meniscal flap tear, Mild OA | Severe bone-on-bone OA, Insidious onset of generalized pain, Malalignment | Pending litigation/Workers' Comp, High BMI |
Pre-Operative Planning, Templating, and Patient Positioning
The cornerstone of successful osteotomy and arthroplasty surgery lies in meticulous, exhaustive pre-operative planning and radiographic templating. For lower extremity realignment procedures, standard short-leg radiographs are entirely insufficient. The surgeon must obtain full-length, weight-bearing, hip-to-ankle standing alignment films to accurately calculate the mechanical axis deviation (MAD). Additional mandatory views include weight-bearing 45-degree posteroanterior flexion views (Rosenberg views) to assess the functional cartilage space in the posterior condyles, and Merchant or Sunrise views to evaluate the patellofemoral articulation. Advanced imaging, such as MRI, is often utilized to confirm the integrity of the crucial contralateral compartment and assess the status of the menisci and cruciate ligaments prior to committing to a joint preservation strategy.
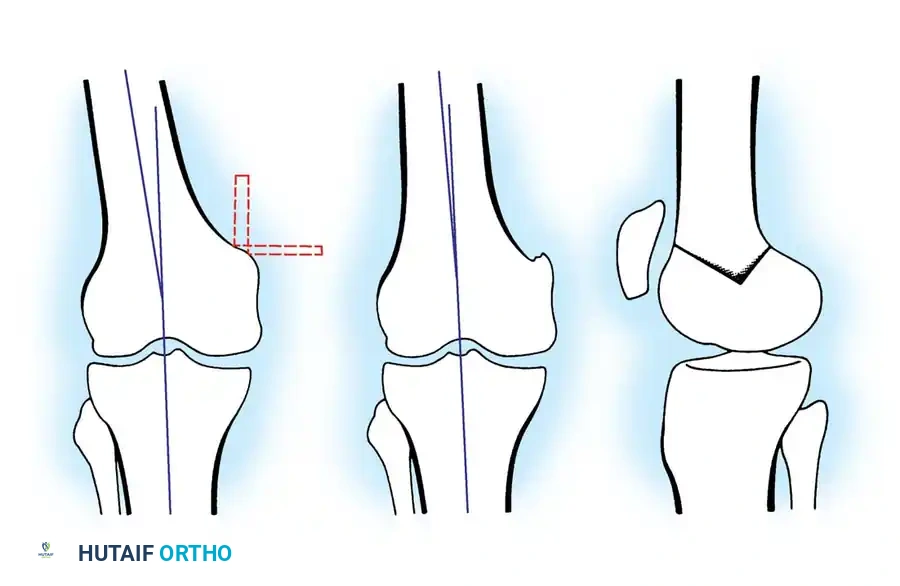
Templating for an HTO or DFO requires precise geometric calculations to determine the exact degree of correction required. The Miniaci method is widely considered the gold standard for this calculation. The surgeon first plots the current mechanical axis. Next, a new, desired mechanical axis is drawn from the center of the femoral head through the target coordinate on the tibial plateau (e.g., the Fujisawa point at 62% for a varus knee). A hinge point is then established on the lateral cortex of the tibia (for a medial opening wedge HTO), typically 1.5 cm distal to the lateral joint line to preserve the proximal tibiofibular joint. Lines are drawn from the hinge point to the center of the ankle mortise on both the current and planned mechanical axes. The angle subtended by these two lines dictates the exact angular correction and the required base width of the opening wedge. This precise templating prevents both under-correction (leading to early failure) and over-correction (leading to rapid contralateral compartment degeneration).
For upper extremity procedures, particularly Total Elbow Arthroplasty, pre-operative templating focuses on assessing bone stock, medullary canal geometry, and the extent of capitellar and trochlear wear. True anteroposterior and lateral radiographs of the elbow are templated to determine the appropriate size of the ulnar and humeral stems. In cases of severe rheumatoid arthritis or post-traumatic deformity, computed tomography (CT) with 3D reconstruction is invaluable for evaluating bone loss and planning for potential structural allografts. The surgeon must carefully evaluate the anatomic axis of the humerus and ulna to ensure the stems will not perforate the cortices during reaming and broaching, a complication that is notoriously difficult to salvage in the osteopenic bone typical of TEA candidates.
Patient positioning and operating room setup are critical logistical steps that directly impact the surgical flow and the accuracy of intraoperative fluoroscopy. For knee osteotomies, the patient is positioned supine on a fully radiolucent Jackson or OSI table. A sterile tourniquet is applied high on the thigh. A bump is often placed under the ipsilateral hip to correct external rotation and ensure a true anteroposterior fluoroscopic view of the knee. The C-arm must be positioned to allow unhindered arc rotation to verify guide pin placement in both coronal and sagittal planes. For elbow procedures, positioning is dictated by the specific approach. A lateral Kocher approach for synovectomy and radial head excision can be performed supine with the arm draped across a chest roll. However, for a posterior approach utilized in TEA, the lateral decubitus position with the arm draped over a well-padded post provides superior, gravity-assisted exposure to the posterior radiocapitellar and ulnohumeral articulations, whilst facilitating excellent access for the mandatory ulnar nerve transposition.
Step-by-Step Surgical Approach and Fixation Technique
Knee Joint Preservation and Osteotomy Techniques
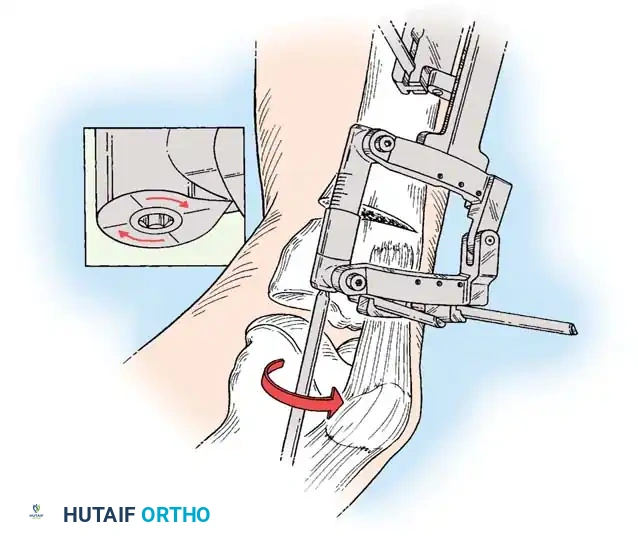
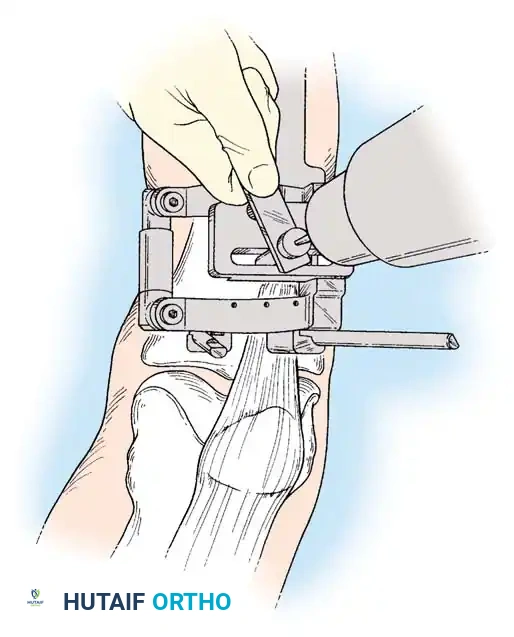
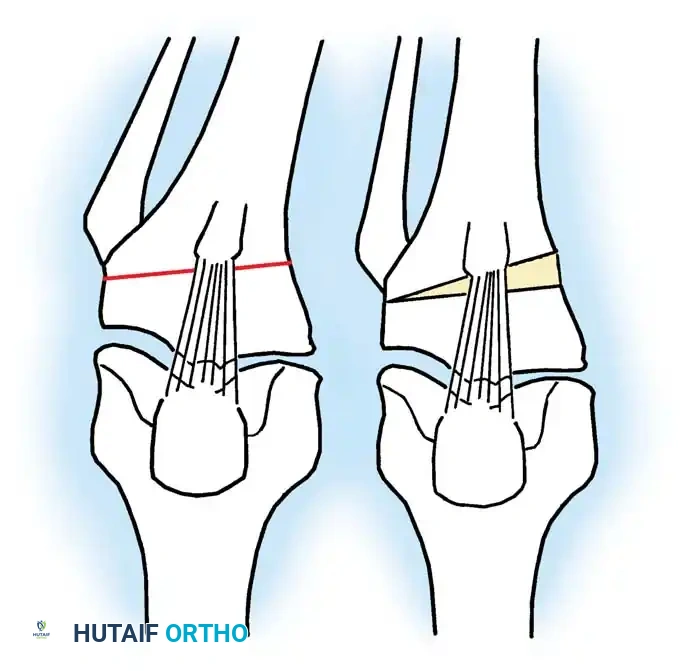
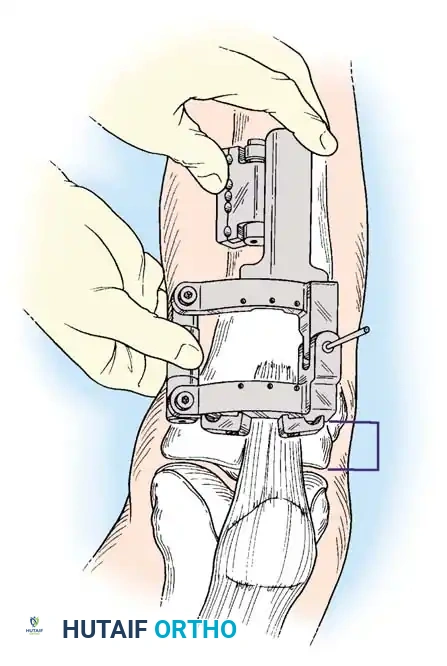
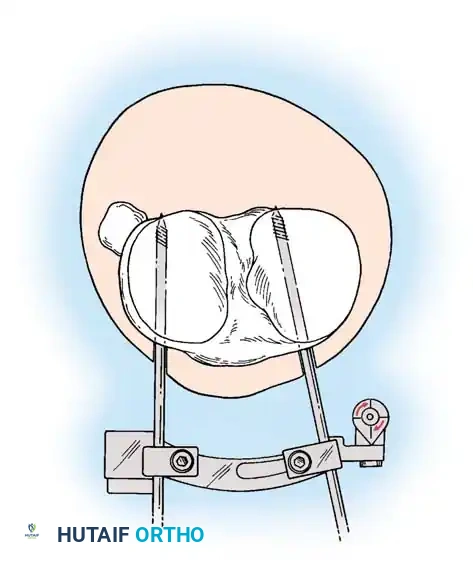
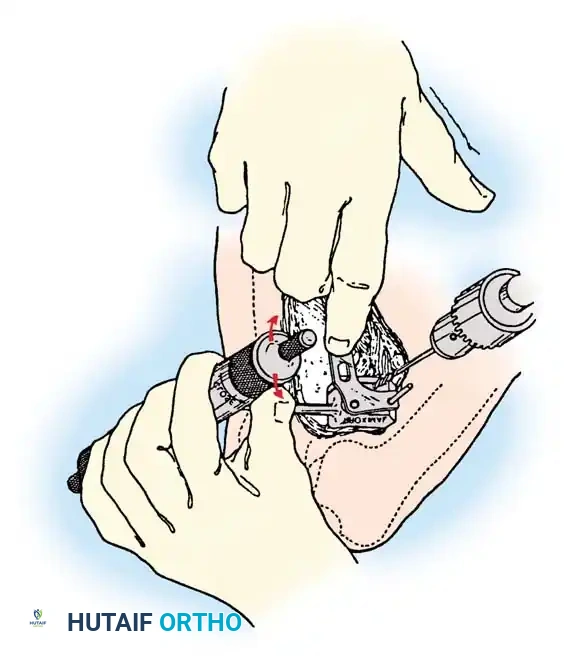
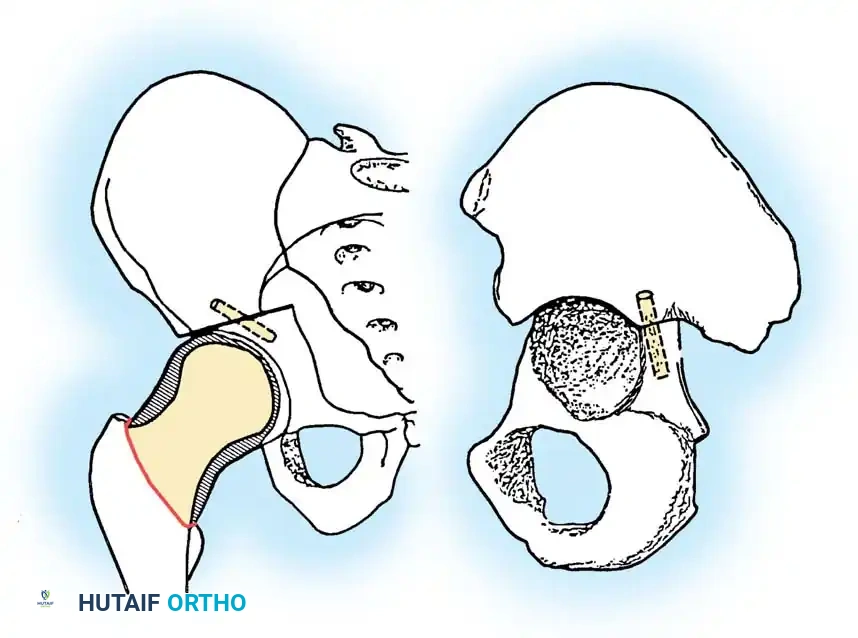
The medial opening wedge High Tibial Osteotomy (HTO) begins with an oblique or longitudinal incision centered over the anteromedial proximal tibia. Dissection is carried down to the pes anserinus, which is carefully retracted distally or partially elevated. The superficial medial collateral ligament (sMCL) is identified; its distal fibers must be released from the tibia to allow the osteotomy to open symmetrically without increasing medial compartment pressures. Retractors are placed posteriorly to protect the neurovascular bundle. Under fluoroscopic guidance, two parallel guide pins are advanced from medial to lateral, targeting the lateral hinge point (typically 1-1.5 cm distal to the lateral articular margin and proximal to the fibular head).
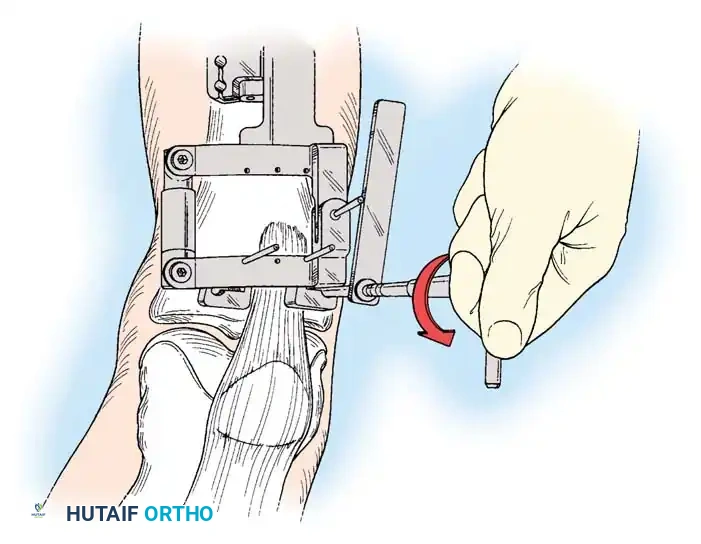
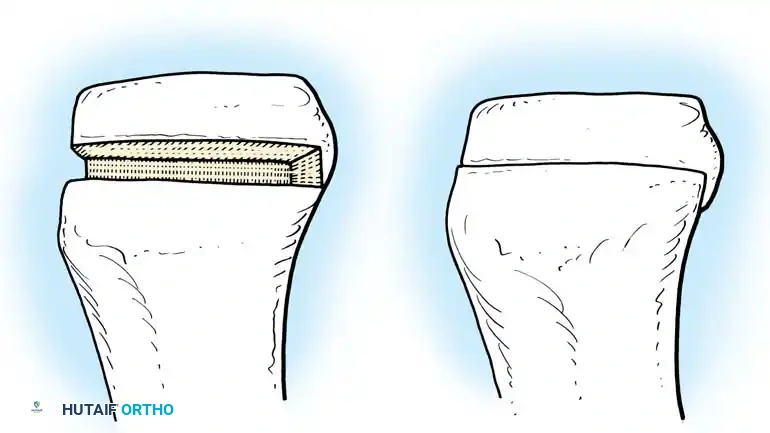
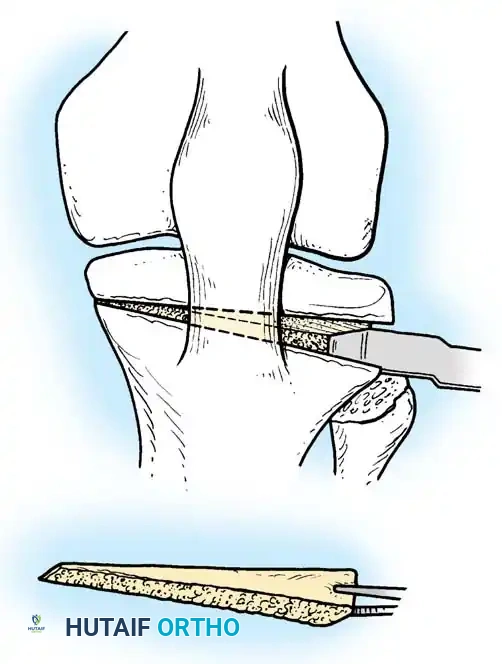
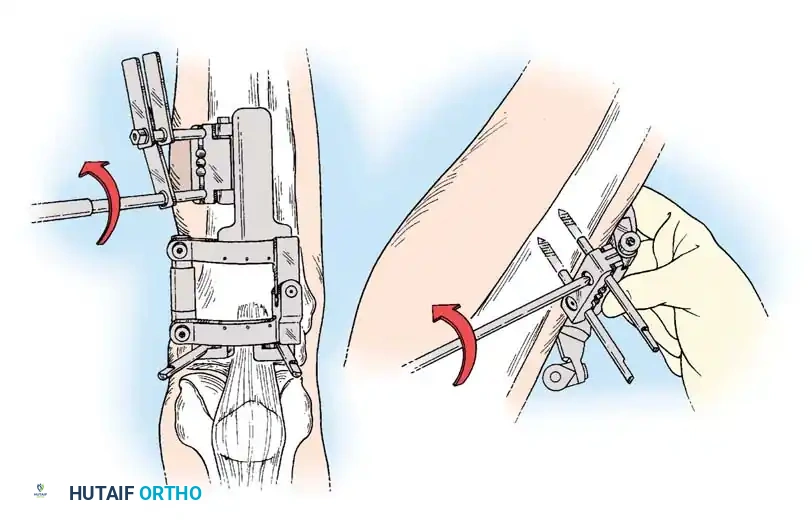
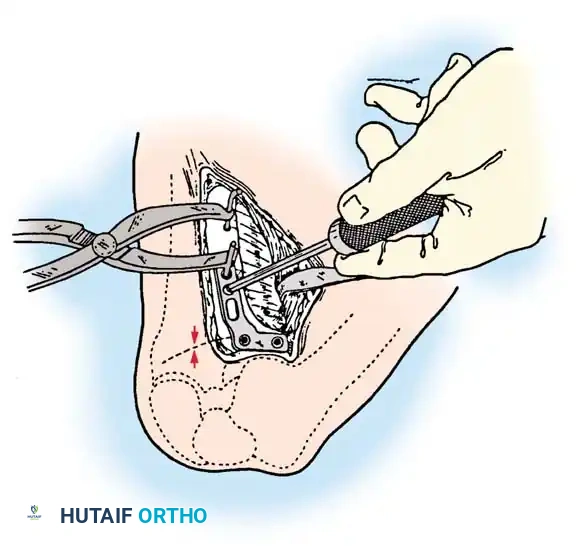
A biplanar osteotomy is highly recommended to enhance rotational stability and increase the surface area for bone healing. The transverse cut is made immediately distal to the guide pins using an oscillating saw, stopping 1 cm short of the lateral cortex to preserve the crucial bony hinge. The ascending coronal cut is then made behind the tibial tubercle, maintaining a bone bridge of at least 1 cm to prevent tubercle avulsion. Flexible osteotomes are sequentially impacted into the transverse cut to gently open the osteotomy. A calibrated opening jack or stacked wedges are utilized to achieve the templated correction angle, which is meticulously verified with an alignment rod under fluoroscopy, confirming the WBL now intersects the Fujisawa point.
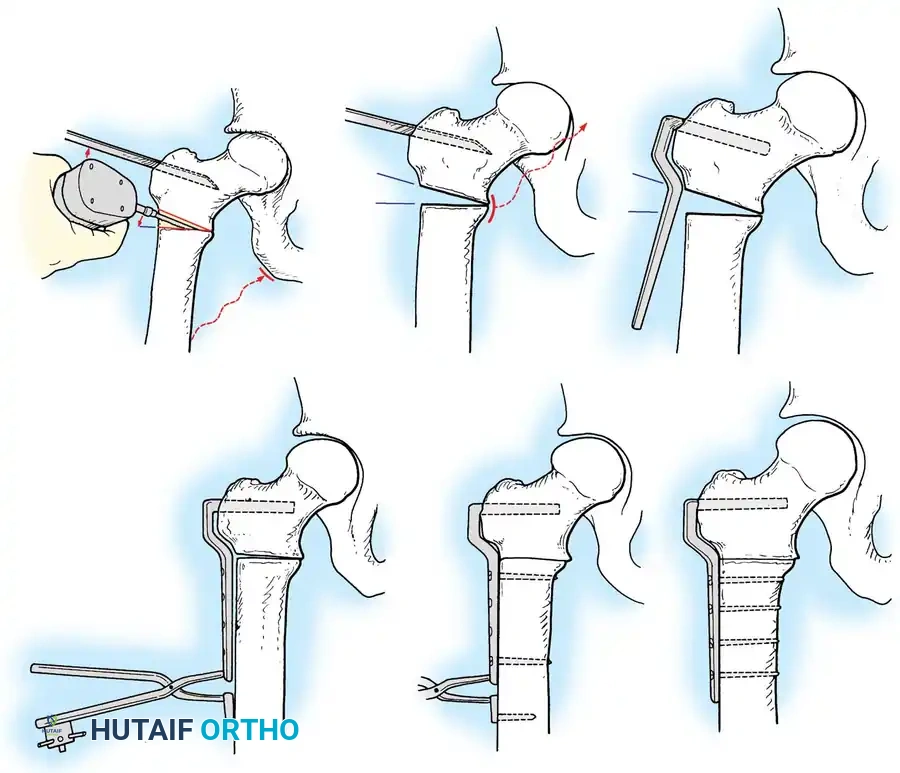
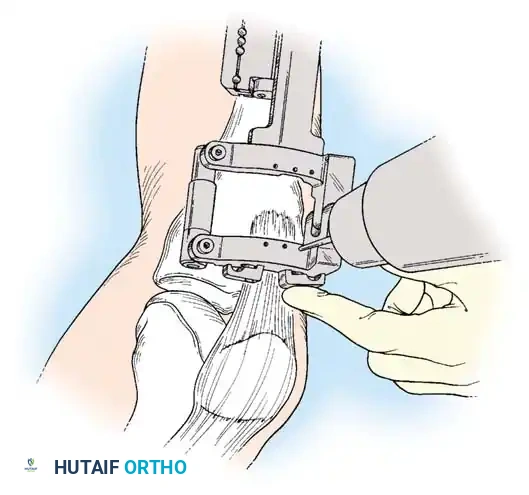
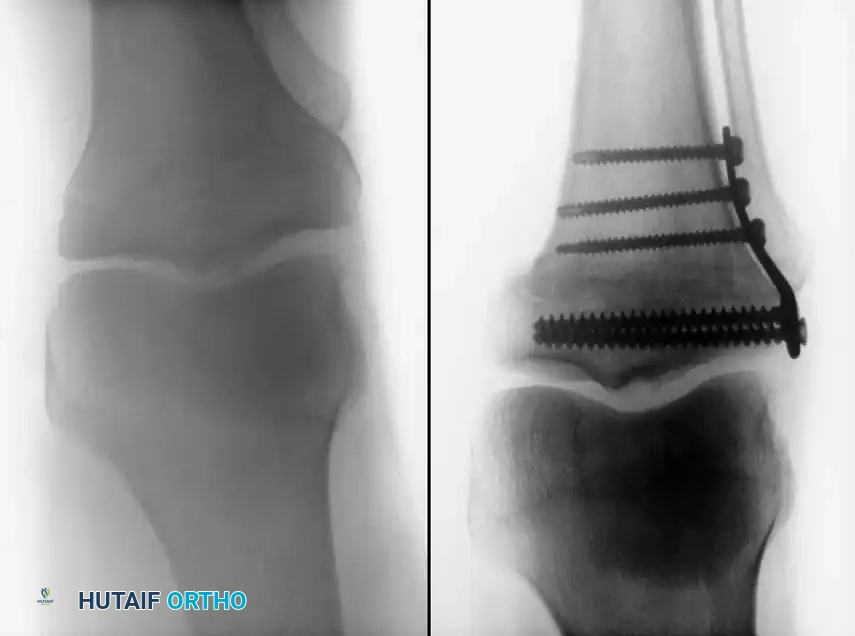
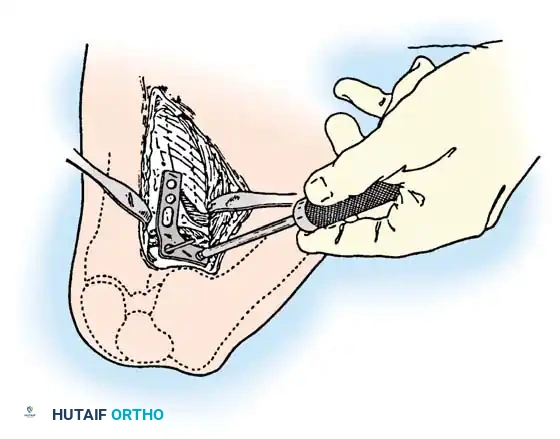
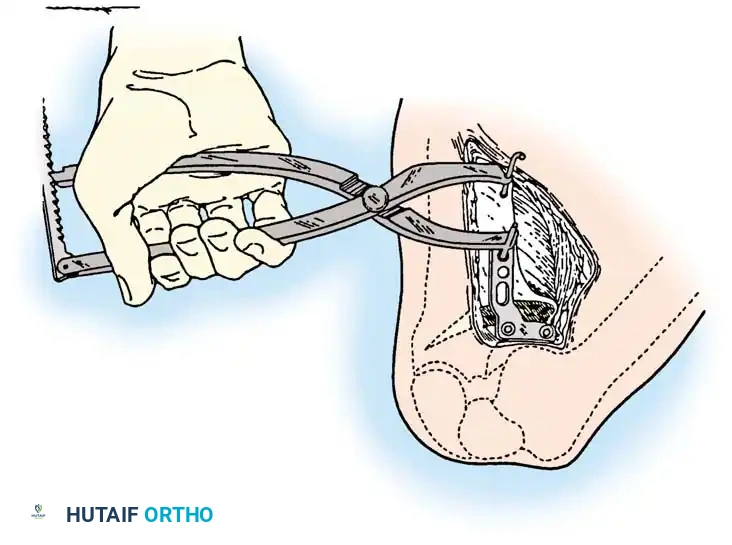
Once the optimal correction is achieved, rigid internal fixation is paramount. Anatomically contoured, titanium locking plates (such as the TomoFix system) are the gold standard. The plate is applied to the anteromedial tibia, and locking screws are placed proximally into the tibial plateau, ensuring they do not breach the articular surface. Distal locking screws are then inserted to secure the construct. Depending on the size of the opening wedge (typically >10mm) and the patient's biological healing capacity, the resulting void may be grafted with structural allograft (e.g., iliac crest or fibular wedges), autograft, or synthetic tricalcium phosphate bone substitutes to provide structural support and osteoconductive scaffolding. The wound is closed in layers over a suction drain to prevent hematoma formation.
Distal Femoral Osteotomy (DFO) for valgus malalignment is typically performed via a lateral opening wedge or medial closing wedge technique. The lateral opening wedge DFO utilizes a lateral longitudinal incision, elevating the vastus lateralis off the lateral intermuscular septum. Guide pins are directed from lateral to medial, targeting a hinge point just proximal to the medial epicondyle. The osteotomy is performed, taking extreme care not to propagate the cut into the intercondylar notch, which would destabilize the entire distal femur. The osteotomy is opened, grafted, and stabilized with a robust distal femoral locking plate. The biomechanical forces on the distal femur are substantially higher than the proximal tibia; thus, fixation must be exceptionally rigid to withstand the significant bending moments and prevent catastrophic hardware failure or nonunion.
Elbow Arthroplasty and Synovectomy Procedures
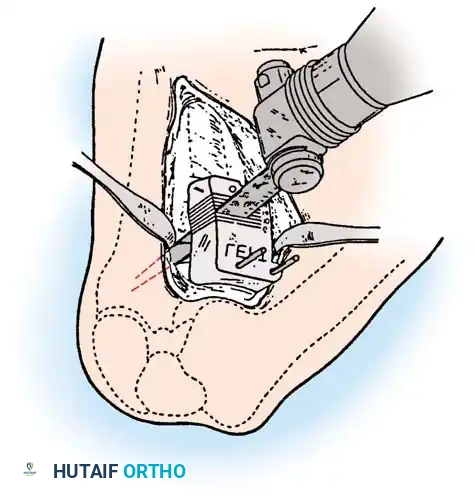
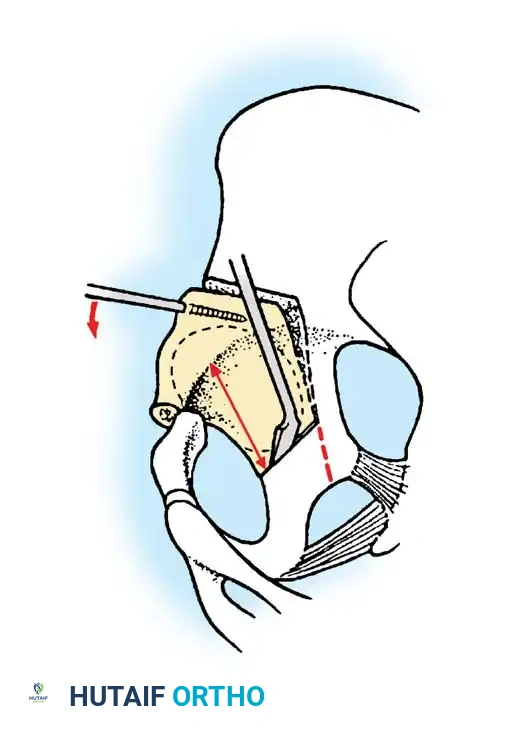
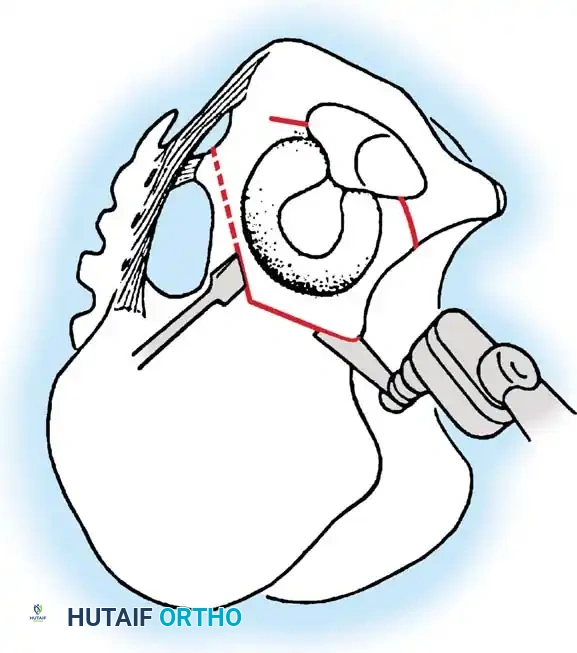
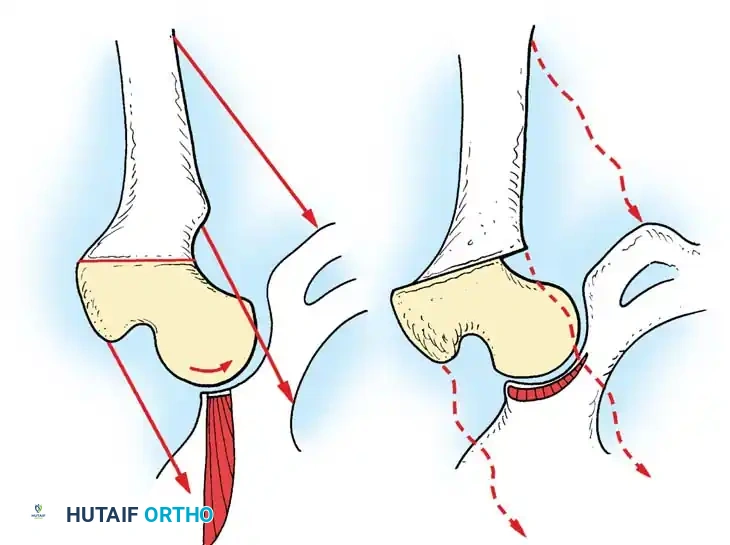
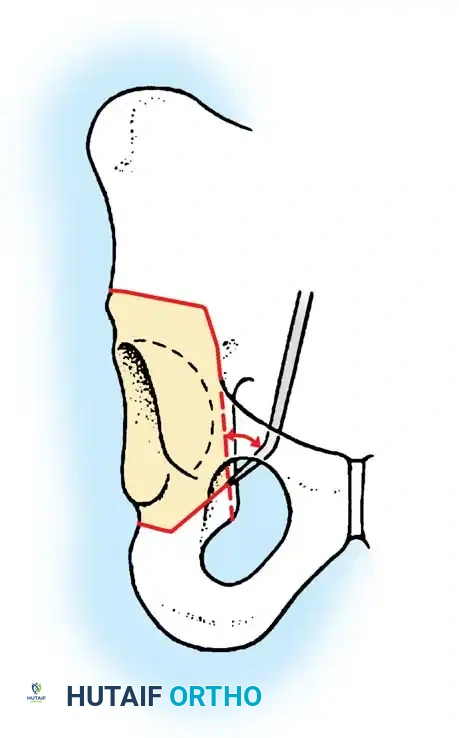
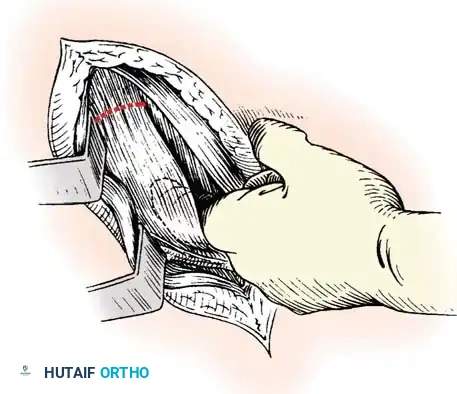
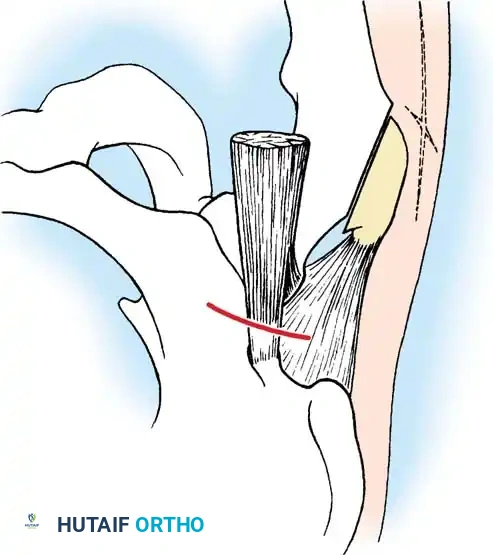
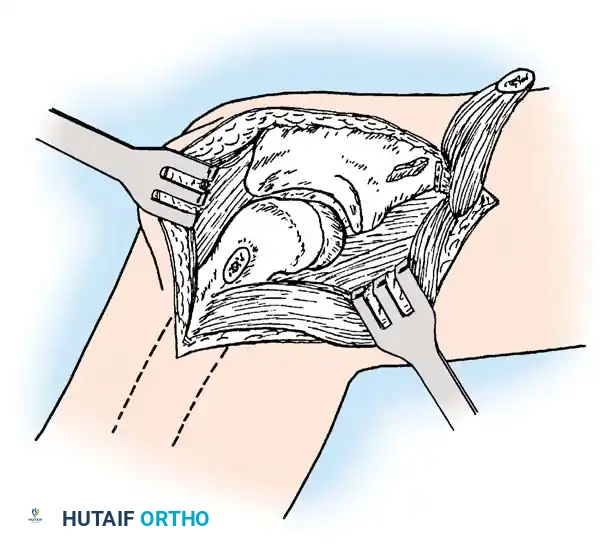
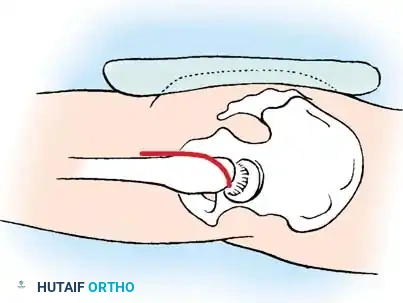
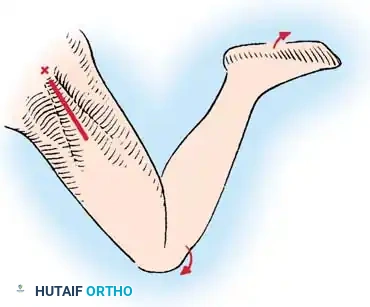
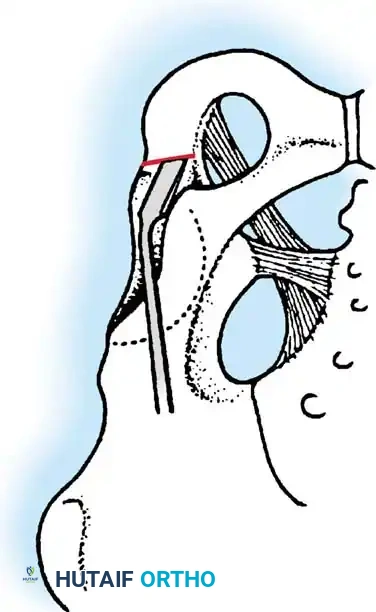
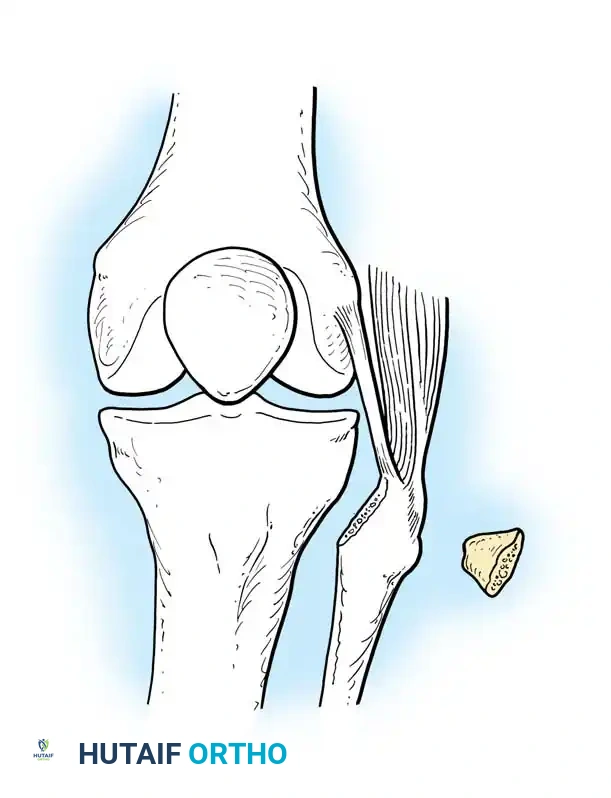
For the osteoarthritic or rheumatoid elbow requiring synovectomy and radial head excision, the lateral Kocher approach is highly effective. The incision extends from the lateral epicondyle distally toward the posterior border of the ulna. The interval between the anconeus and the extensor carpi ulnaris (ECU) is developed. The common extensor origin is elevated, exposing the radiocapitellar joint capsule. The capsule is incised longitudinally, immediately anterior to the lateral ulnar collateral ligament (LUCL). The radial head is visualized, and an oscillating saw is used to resect the head precisely at the level of the annular ligament. A comprehensive anterior and posterior synovectomy is then performed using rongeurs and arthroscopic shavers. The absolute critical step here is the meticulous preservation of the LUCL; the surgeon must maintain a thick sleeve of tissue posteriorly to ensure the elbow does not succumb to iatrogenic posterolateral rotatory instability.
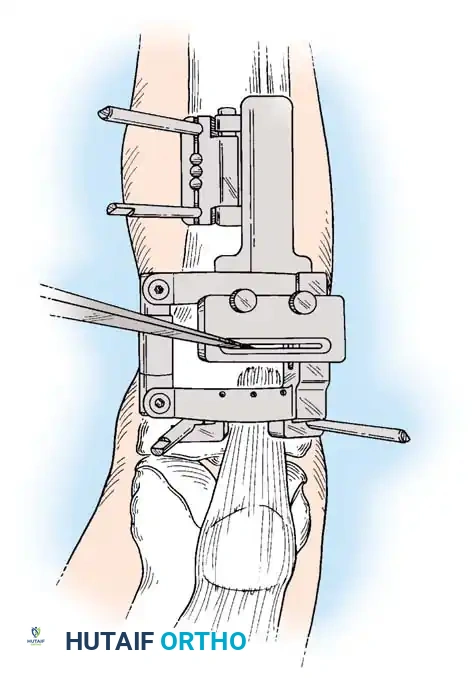
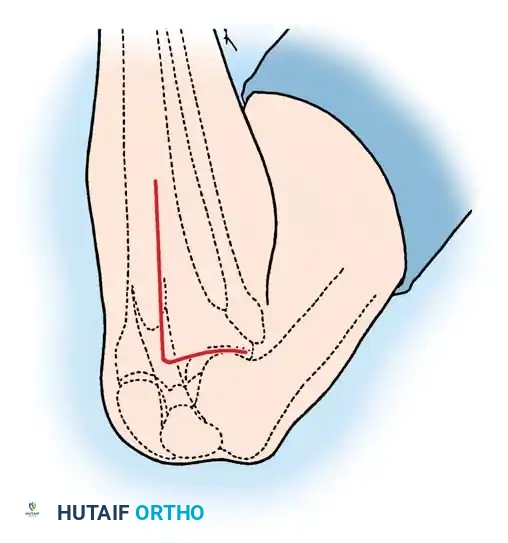
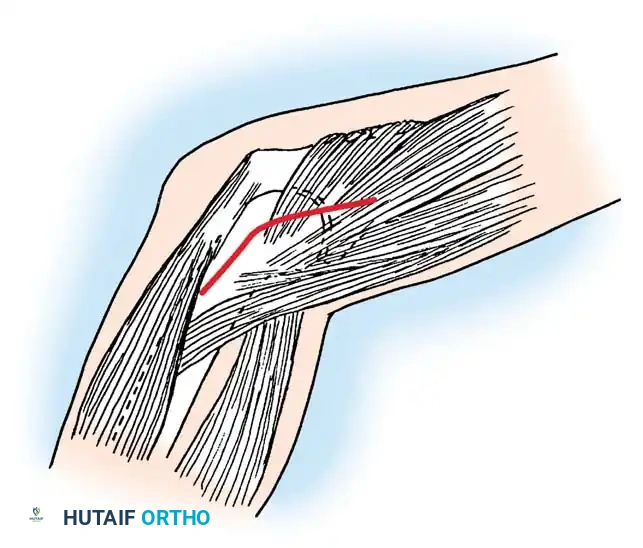
Total Elbow Arthroplasty (TEA) demands a more extensive posterior approach. A straight posterior incision is made, curving slightly laterally around the olecranon to avoid placing the scar directly over the bony prominence. The ulnar nerve is immediately identified proximally, meticulously neurolysed, and mobilized from the cubital tunnel. It is protected with a vessel loop for the duration of the procedure and ultimately transposed anteriorly into a subcutaneous or subfascial pocket. The triceps mechanism is then managed; a triceps-sparing approach (Bryan-Morrey) or a triceps-reflecting approach can be utilized depending on the surgeon's preference and the required exposure. The collateral ligaments are released, and the joint is dislocated.

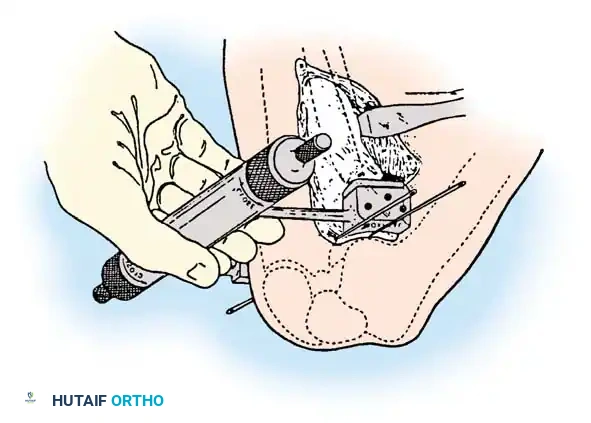
Humeral and ulnar preparation involves precise intramedullary reaming and broaching. The distal humerus is resected to accommodate the capitellocondylar or semiconstrained prosthesis. The medullary canals of both the ulna and humerus are thoroughly irrigated and dried. Third-generation cementing techniques are mandatory. A restrictive cement plug is placed in the medullary canals, and PMMA bone cement is injected retrograde using a syringe system to ensure deep interdigitation into the cancellous bone. The humeral and u
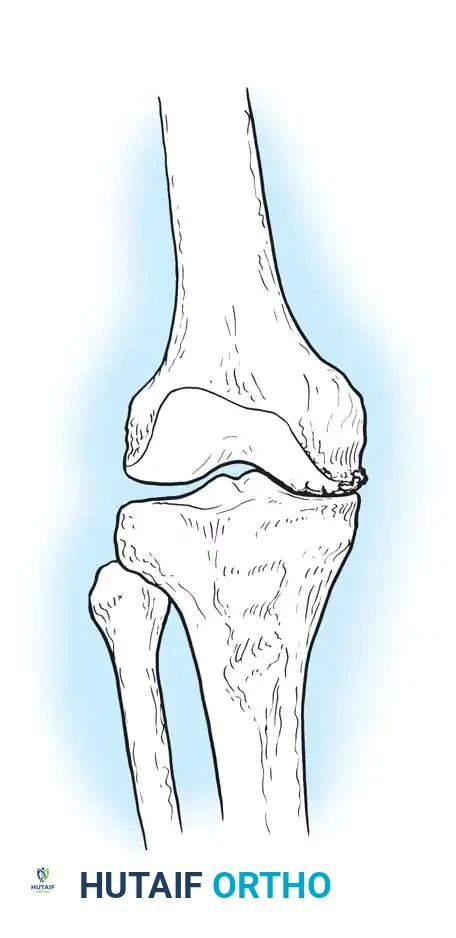
Clinical & Radiographic Imaging Archive