Rheumatoid Finger Deformities: Pathomechanics & Surgery
Key Takeaway
Rheumatoid arthritis frequently produces complex finger deformities, including intrinsic plus and swan-neck presentations. These result from a combination of synovial hypertrophy, capsular attenuation, and altered biomechanical forces. Successful surgical management requires a systematic approach, prioritizing proximal joint stability before addressing digital deformities. Treatment ranges from soft tissue rebalancing, such as intrinsic release and flexor digitorum superficialis tenodesis, to salvage procedures like proximal interphalangeal joint arthrodesis or arthroplasty, depending on joint flexibility and articular destruction.
Comprehensive Introduction and Patho-Epidemiology
Deformities of the fingers in rheumatoid arthritis (RA) are the culmination of relentless, destructive synovitis interacting with the complex biomechanical forces of the hand. These deformities are driven by normal physiological forces applied to joints that have been structurally compromised by the systemic disease process. The extrinsic flexors and extensors, combined with the tightness of the intrinsic muscles, exert immense deforming forces on attenuated capsuloligamentous structures. The rheumatoid hand represents a unique biomechanical environment where enzymatic degradation of collagenous restraints allows normal muscle tone to produce profound architectural collapse.
The epidemiology of rheumatoid hand deformities demonstrates a strong predilection for the small joints of the hands and wrists, which are clinically involved in over 90% of patients with established RA. Despite the advent of disease-modifying antirheumatic drugs (DMARDs) and biologic therapies that have dramatically altered the natural history of RA, a significant cohort of patients still progresses to structural joint failure. This may be due to delayed diagnosis, refractory disease phenotypes, or lack of access to advanced pharmacotherapy. The cascade of destruction typically begins with synovial hypertrophy and pannus formation, leading to the stretching of the joint capsule and collateral ligaments, and culminates in articular cartilage destruction and periarticular bone erosions.

Specific anatomical failures in the rheumatoid hand include the displacement of the lateral bands of the extensor hood, rupture of the central slip, or attritional rupture of the long extensor or flexor tendons. Furthermore, abnormal forces act on joints already weakened by erosive pannus. Flexor tenosynovitis frequently produces a mechanical limitation of interphalangeal (IP) joint motion; consequently, the range of active flexion in these joints is significantly less than passive flexion. This discrepancy between active and passive motion is a hallmark of tenosynovial tethering and is often the earliest harbinger of impending tendon rupture or fixed joint contracture.
When managing the rheumatoid hand, the orthopedic surgeon must view the upper extremity as a single functional and kinetic unit. Souter famously advocated for a strict hierarchy of surgical interventions, emphasizing the correction of significant disease and deformity in the elbow and shoulder before addressing hand deformities. According to Ferlic, Smyth, and Clayton, surgical priorities follow a descending order of importance: Spine (cervical instability is life-threatening), Foot and Hip (weight-bearing and ambulation), Knee, Wrist (the foundation of hand function), Shoulder and Thumb, Elbow, and finally, the Fingers. Persistent tenosynovitis, impending tendon rupture, and nerve compression are high-priority problems that supersede this anatomical hierarchy. Generally, if wrist arthroplasty or arthrodesis is indicated, it must be performed first, as a stable, properly aligned wrist is an absolute prerequisite for balanced digital function.
Detailed Surgical Anatomy and Biomechanics
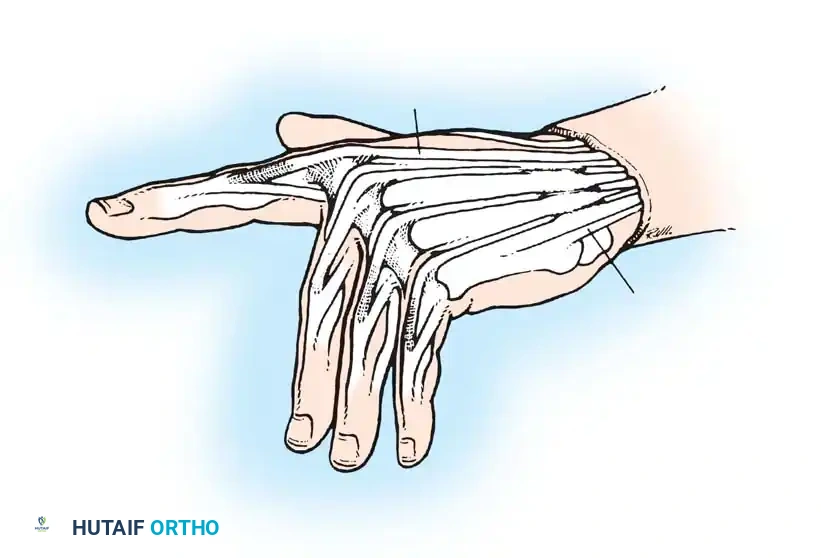
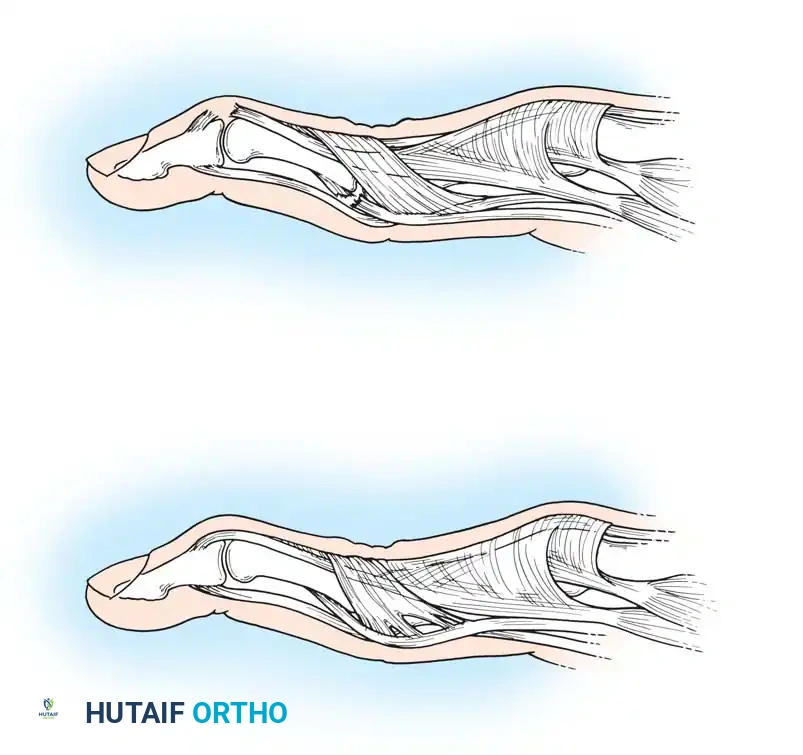
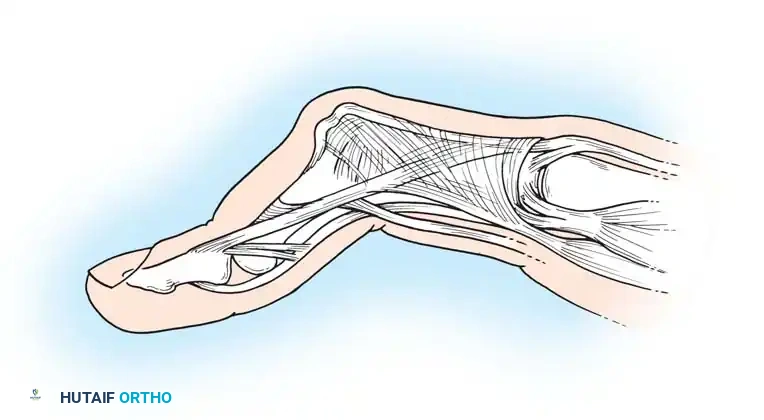
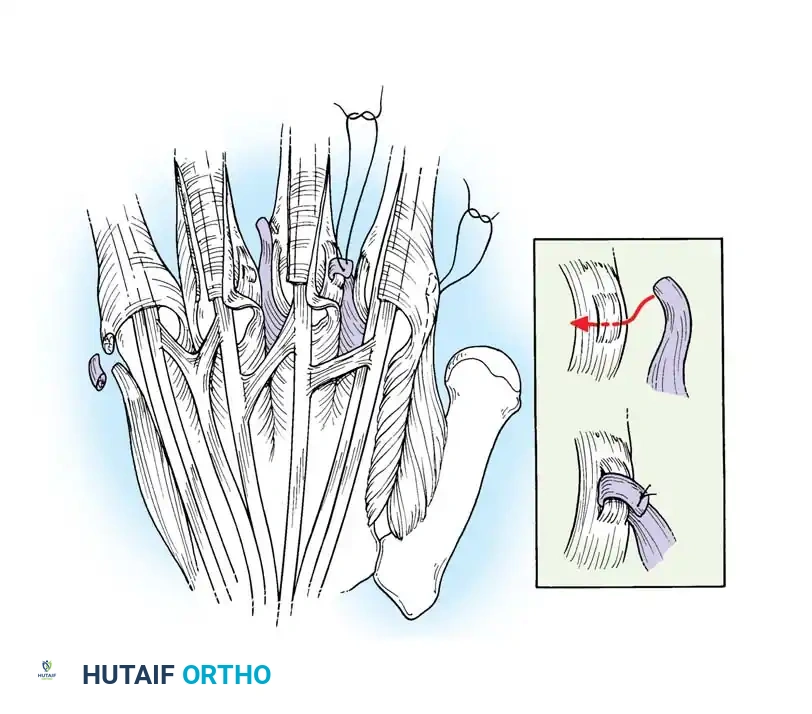
A profound understanding of the extensor mechanism and intrinsic musculature is paramount for the surgical reconstruction of the rheumatoid finger. The extensor hood is a highly sophisticated, multi-layered aponeurotic expansion that coordinates motion across the metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints. The extrinsic extensor tendon (extensor digitorum communis) bifurcates into a central slip, which inserts on the base of the middle phalanx to extend the PIP joint, and two lateral slips. These lateral slips merge with the tendinous contributions of the intrinsic muscles (lumbricals and interossei) to form the lateral bands, which coalesce distally into the terminal tendon inserting on the distal phalanx. The delicate balance of this system relies on the integrity of the triangular ligament (which prevents volar subluxation of the lateral bands) and the transverse retinacular ligament (which prevents dorsal subluxation).

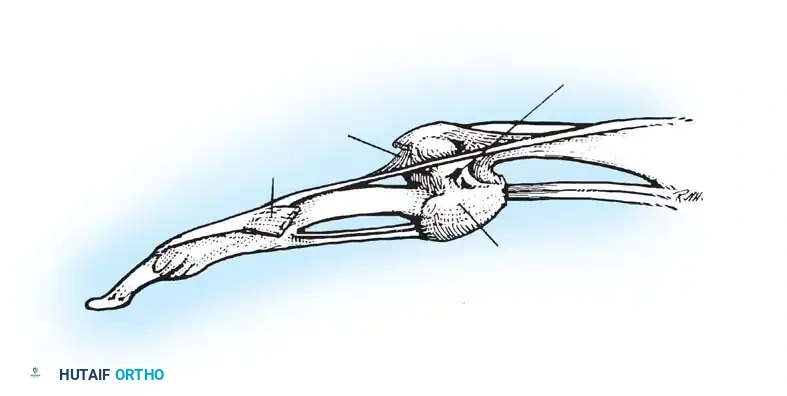
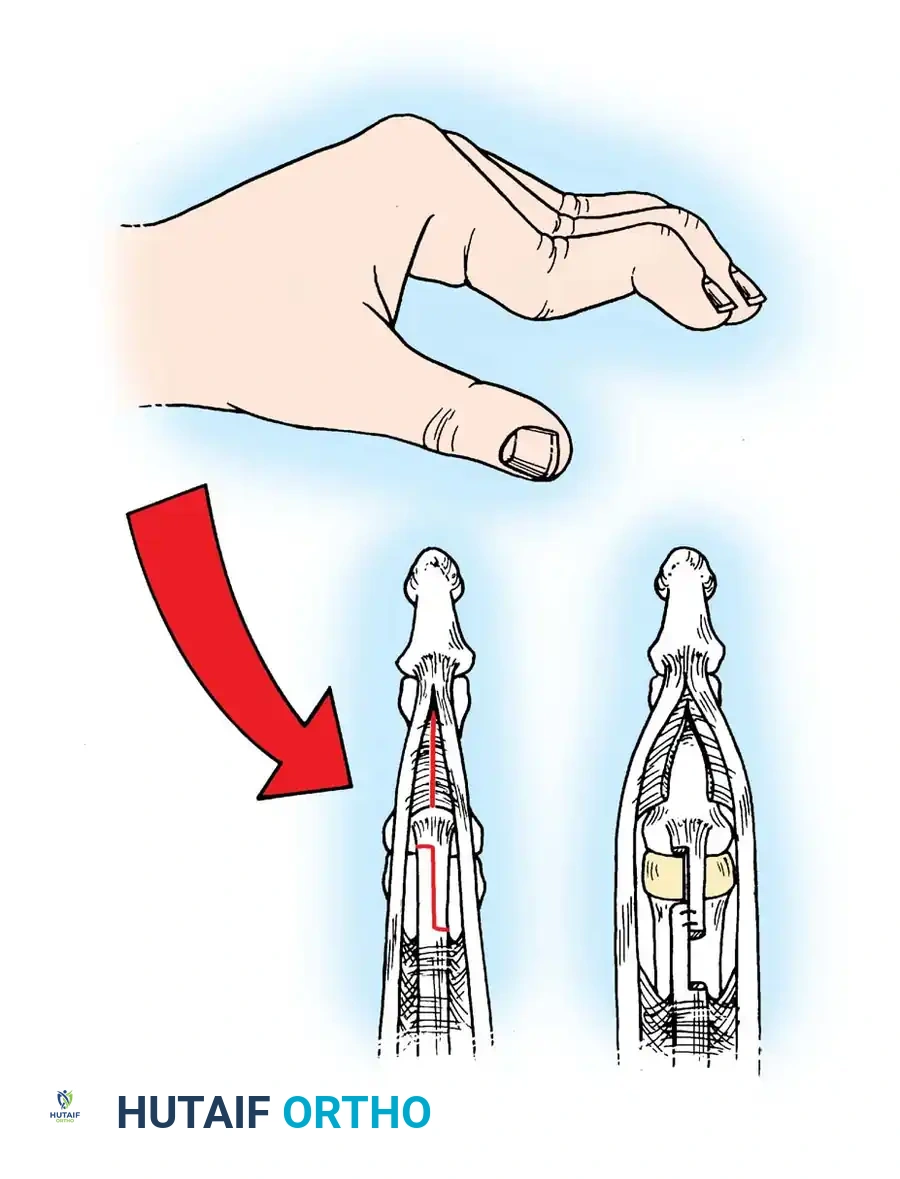
The intrinsic plus deformity is characterized by flexion of the MCP joints and extension of the PIP joints. It is caused by the tightness, spasm, and eventual ischemic contracture of the intrinsic muscles secondary to rheumatoid inflammation. In hands with a fixed intrinsic plus deformity, the PIP joint cannot be flexed while the MCP joint is fully extended. Accurate clinical testing is essential to differentiate intrinsic tightness from capsular contracture or extrinsic tendon adhesions. The Bunnell Test for intrinsic tightness is performed by passively holding the MCP joint in maximum extension, placing the intrinsic muscles on stretch. If the intrinsics are tight, passive flexion of the PIP joint is prevented or significantly limited. Conversely, when the MCP joint is passively flexed (relaxing the intrinsics), passive flexion of the PIP joint increases.

With ulnar drift of the fingers, intrinsic tightness may be present only on the ulnar side. To test this accurately, axial alignment of the finger with the metacarpal must be maintained. Any ulnar deviation at the MCP joint during the test slackens the intrinsics on the ulnar side and will yield a false-negative result. A tight first volar interosseous muscle pulls the extended index finger ulnarward. If the finger is held in line with the second metacarpal during the test, tightness of this specific muscle can be isolated. Tightness in the oblique retinacular ligament (ORL) is demonstrated by maintaining the PIP joint in extension while testing the DIP joint's resistance to passive flexion. This is particularly helpful when evaluating a digit with an evolving boutonnière or swan-neck deformity.

The flexor tendon system, comprising the flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS), operates within a tightly constrained fibro-osseous tunnel. Rheumatoid tenosynovitis within this sheath not only limits excursion but also alters the moment arms of the tendons. Beckenbaugh observed that flexor tenosynovitis results in ineffective volar support by the FDS tendon, acting as a primary catalyst for swan-neck deformity. Adherence of the FDS tendon prevents it from stabilizing the PIP joint against hyperextension. The unopposed overpull of the central tendon, combined with PIP synovitis, stretches the volar plate, locking the joint in hyperextension.
Exhaustive Indications and Contraindications
The fundamental goals of rheumatoid hand surgery are pain relief, improvement of function, and the prevention of further anatomical deterioration; cosmetic improvement is a secondary, albeit welcome, benefit. Surgical intervention is indicated when medical management has been optimized but fails to halt progressive deformity, or when mechanical complications (e.g., tendon rupture, severe nerve compression) arise. Prophylactic surgery, such as dorsal tenosynovectomy of the wrist or flexor tenosynovectomy of the digits, is highly effective in preventing attritional tendon ruptures and should be performed aggressively when tenosynovitis persists for more than 4 to 6 months despite optimal medical therapy.
Reconstructive procedures for finger deformities are indicated based on the flexibility of the joints and the degree of articular destruction. For flexible deformities (Nalebuff Type I and II swan-neck deformities), soft tissue rebalancing procedures such as intrinsic release, lateral band mobilization, or PIP joint flexor tenodesis are indicated. For stiff deformities with preserved joint spaces (Type III), joint manipulation combined with soft tissue release is required. When severe radiographic destruction is present (Type IV), salvage procedures such as silicone implant arthroplasty (for MCP and PIP joints) or arthrodesis (for PIP and DIP joints) become the definitive indications. Arthrodesis is particularly favored in the index and middle finger PIP joints to provide a stable post for pinch, whereas arthroplasty is often preferred in the ring and small fingers to preserve grip contour.
Contraindications to rheumatoid hand reconstruction must be carefully evaluated to avoid disastrous outcomes. Absolute contraindications include active local or systemic infection, profoundly compromised vascularity to the digit, and severe medical comorbidities that preclude safe anesthesia. Relative contraindications include a non-compliant patient, active and uncontrolled systemic flares of RA, and profound osteopenia that would preclude the stable seating of an arthroplasty implant or the secure fixation of an arthrodesis. Furthermore, operating on the fingers in the presence of an unstable or severely deviated wrist is a biomechanical contraindication; the wrist must be stabilized first to ensure the longevity of the digital reconstruction.
| Category | Indications | Contraindications |
|---|---|---|
| Soft Tissue Procedures (Synovectomy, Tenodesis, Releases) | Persistent tenosynovitis > 4-6 months; Flexible deformities (Nalebuff Type I/II); Impending tendon rupture; Intrinsic tightness with preserved joint space. | Fixed joint contractures; Severe articular destruction (bone-on-bone); Active local infection. |
| Silicone Implant Arthroplasty (MCP/PIP) | End-stage joint destruction (Nalebuff Type IV); Painful, stiff joints in ulnar digits (ring/small); Ulnar drift with subluxation. | Active infection; Inadequate skin envelope; Severe osteopenia precluding stem support; Unstable wrist (relative). |
| Arthrodesis (PIP/DIP) | Severe instability or destruction in radial digits (index/long); Fixed flexion contractures > 40 degrees; Failed arthroplasty. | Need for high-demand dexterity requiring full ROM; Poor bone stock for fixation; Active infection. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning begins with an exhaustive clinical examination to document the active and passive range of motion of every joint in the hand and wrist. The surgeon must meticulously assess the presence of intrinsic tightness, the integrity of the extrinsic flexor and extensor tendons, and the stability of the collateral ligaments. For swan-neck deformities, applying the Nalebuff classification is critical, as it directly dictates the surgical algorithm. Grip and pinch strength should be recorded to establish a baseline for post-operative comparison. The skin envelope must be evaluated for rheumatoid nodules, vasculitic lesions, and general tissue turgor, as rheumatoid skin is notoriously fragile and prone to delayed healing.

Radiographic evaluation requires high-quality posteroanterior, true lateral, and oblique views of the hand and wrist. The surgeon should look for periarticular osteopenia, joint space narrowing, marginal erosions, and subluxations or dislocations. If silicone implant arthroplasty is planned, digital templating is essential to estimate the appropriate implant size and to assess the intramedullary canal diameter. In patients with severe bone loss or cystic changes, the surgeon must be prepared with alternative techniques, such as bone grafting or utilizing specialized implants with thicker stems. Cervical spine radiographs (flexion/extension views) are mandatory in all RA patients prior to surgery to rule out atlantoaxial subluxation, which poses a lethal risk during endotracheal intubation.
Medical optimization requires close coordination with the patient's rheumatologist. The perioperative management of biologic agents (e.g., TNF-alpha inhibitors) and conventional DMARDs (e.g., methotrexate) must be carefully planned. Current guidelines generally recommend continuing methotrexate but holding biologic agents for one to two dosing cycles prior to surgery to mitigate infection risk, resuming them once wound healing is secure. Patients on chronic corticosteroid therapy may require perioperative stress-dose steroids to prevent adrenal crisis.
Patient positioning is standard for hand surgery. The patient is placed supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Regional anesthesia (brachial plexus block) is highly preferred over general anesthesia, as it provides excellent intraoperative muscle relaxation, profound post-operative analgesia, and avoids the airway risks associated with rheumatoid cervical spine disease. Prophylactic intravenous antibiotics (typically a first-generation cephalosporin) are administered 30 minutes prior to tourniquet inflation. The limb is exsanguinated with an Esmarch bandage, and the tourniquet is inflated to 250 mm Hg.
Step-by-Step Surgical Approach and Fixation Technique
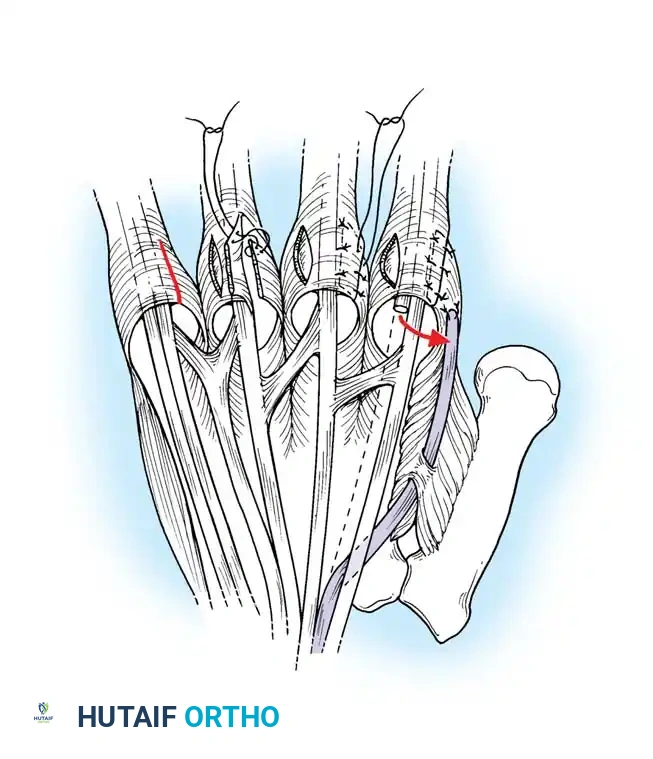
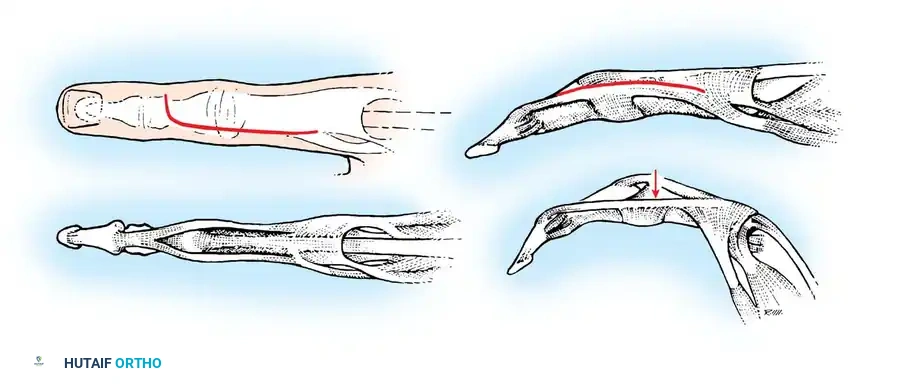
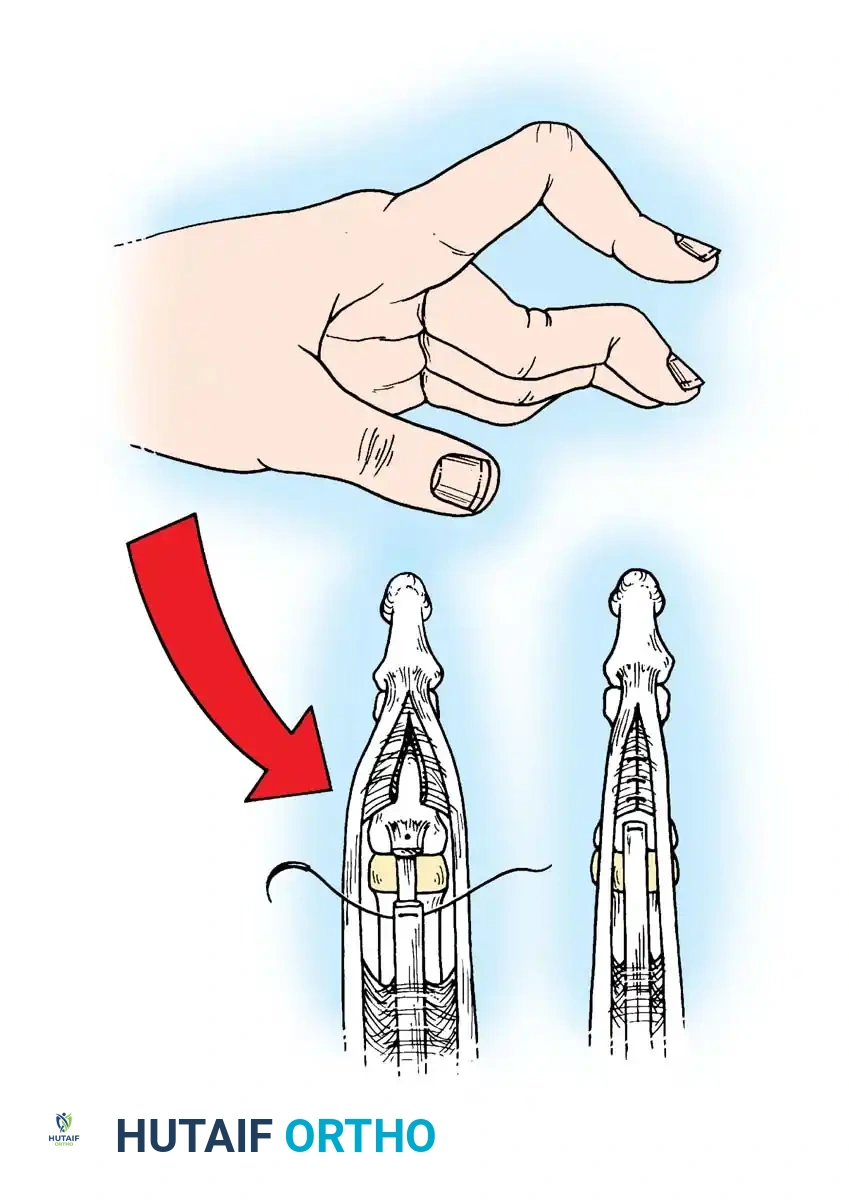
The correction of rheumatoid finger deformities requires meticulous soft tissue handling. For the correction of a flexible PIP hyperextension deformity (swan-neck), the Beckenbaugh FDS tenodesis is the gold standard. This technique utilizes a slip of the FDS to create a volar tether, preventing PIP hyperextension while allowing active flexion. The approach begins with a volar zigzag (Bruner) incision over the middle and proximal phalanges. The surgeon must meticulously avoid damaging the digital neurovascular bundles, which may be displaced or adherent to the cruciate pulley system anterior to the hyperextended PIP joint.
Once the skin flaps are elevated, the cruciate pulleys are exposed by retracting the neurovascular bundles medially and laterally. It is critical to clearly identify and preserve the A2 pulley, as it forms the proximal anchor for the tenodesis. The central pulley system (C1/A3) is incised centrally to expose the underlying flexor tendons. The flexor digitorum profundus (FDP) tendon is retracted, and any adhesions are released. The FDS tendon is then exposed, and a thorough flexor tenosynovectomy is performed to remove the invasive pannus.


The FDS tendon is pulled distally, and the decussation (Camper's chiasm) is incised, splitting the tendon into its two constituent slips. If necessary, the incision is extended proximally, and adhesions at the A1 pulley level are released to allow adequate distal translocation of the tendon. The divided FDS tendon is pulled distally, and the ulnar slip is incised proximally, leaving a 5-cm slip of tendon attached to its insertion on the ulnar side of the middle phalanx. The surgeon must pull the slip firmly to ensure its insertion has not been compromised by erosive synovitis. In the little finger, both slips are often incised and used together because a single slip is usually too diminutive.

A small fenestration is created in the A2 pulley, 3 to 4 mm from its distal border, using a scalpel or fine tenotomy scissors. A small curved hemostat is passed through the hole distally into the sheath. The tip of the harvested FDS tendon slip is clamped and pulled proximally through the fenestration in the A2 pulley. The slip of tendon is brought distally, folding it back on itself. The tension is meticulously adjusted so that the digit is held at exactly 5 to 10 degrees of flexion at the PIP joint. The tendon is then sutured to itself using nonabsorbable 4-0 braided sutures. Over-tensioning the tenodesis is a major pitfall and can result in a severe, iatrogenic PIP flexion contracture. The cruciate pulley is repaired if feasible, and the skin is closed over a small drain.

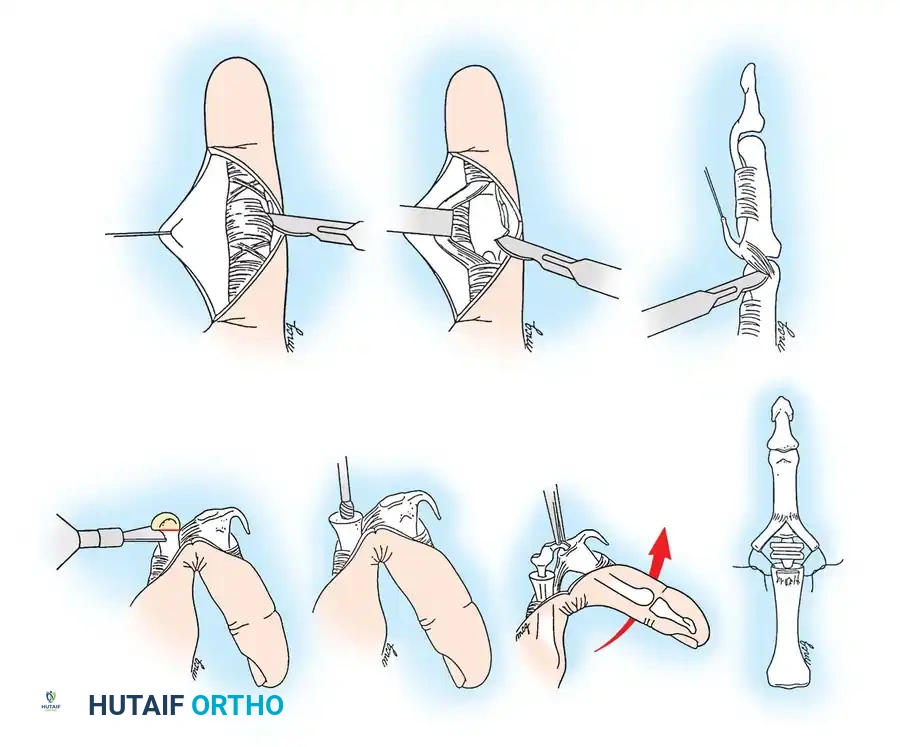


For Type III swan-neck deformities (stiff but with preserved joint space), lateral band mobilization and dorsal skin release (Nalebuff and Millender technique) are required. A dorsal curvilinear incision is made over the PIP joint. The central slip is identified, and the lateral bands, which are often scarred in a dorsal position, are sharply mobilized and relocated volarly to the axis of rotation of the PIP joint. If the PIP joint remains stiff, a gentle manipulation is performed. In severe cases, a step-cut lengthening of the central slip may be necessary to allow PIP flexion.
Complications, Incidence Rates, and Salvage Management
Surgical intervention in the rheumatoid hand carries a unique set of complications, driven largely by the systemic nature of the disease, the fragility of the soft tissues, and the immunosuppressive effects of medical therapies. Wound healing complications and surgical site infections are the most immediate concerns. The incidence of delayed wound healing can reach 10-15% in patients on chronic corticosteroids or those who have not appropriately held their biologic medications. Superficial infections can often be managed with oral antibiotics and local wound care, but deep space infections, particularly in the presence of a silicone implant, demand immediate operative debridement and usually necessitate implant removal.
Recurrence of deformity is a significant long-term complication. In soft tissue reconstructions like the FDS tenodesis for swan-neck deformity, the tenodesis can stretch out over time, leading to a recurrence of PIP hyperextension. This occurs in approximately 15-20% of cases at 5-year follow-up. Conversely, iatrogenic over-tensioning of the tenodesis can create a fixed PIP flexion contracture, severely limiting grip strength and dexterity. Progressive joint destruction from relentless rheumatoid disease can also render a previously successful soft-tissue balancing procedure ineffective, as the bony architecture collapses.
Neurovascular injury during the exposure of the flexor sheath is a devastating complication. The digital nerves in a rheumatoid hand are often displaced by severe synovitis and can be inadvertently transected during the Bruner approach. Careful, systematic exposure and loop magnification are essential to prevent this. If a digital nerve is cut, it must be repaired primarily using epineurial microsurgical techniques. Vascular compromise to the digit, while rare, can occur if both digital arteries are damaged or if profound vasospasm is induced; this requires immediate exploration and potential vein grafting.
Salvage management for failed rheumatoid finger reconstructions typically involves conversion to a more rigid stabilization. If a soft tissue reconstruction fails or if a silicone arthroplasty becomes infected or fractures, the definitive salvage procedure is an arthrodesis of the affected joint. PIP joint arthrodesis provides a stable, pain-free post for pinch and grip, though it sacrifices motion. The joint is typically fused in 25 to 40 degrees of flexion, increasing from the index to the small finger, using tension band wiring, headless compression screws, or crossed Kirschner wires.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Wound Dehiscence / Infection | 5 - 15% | Meticulous tissue handling; perioperative holding of biologics; prophylactic antibiotics. | Local wound care; oral/IV antibiotics; operative debridement and implant removal if deep. |
| Recurrent Swan-Neck Deformity | 15 - 20% | Secure suturing of tenodesis; adequate post-operative splinting; disease control. | Revision tenodesis; conversion to PIP arthrodesis or arthroplasty. |
| Iatrogenic Flexion Contracture | 5 - 10% | Avoid over-tensioning FDS slip (set at 5-10° flexion max); early controlled ROM. | Dynamic extension splinting; surgical release if refractory. |
| Silicone Implant Fracture | 10 - 25% (at 10 yrs) | Proper sizing; adequate bony resection; grommet use (controversial). | Revision arthroplasty; conversion to arthrodesis. |
Phased Post-Operative Rehabilitation Protocols
The success of rheumatoid hand surgery is inextricably linked to a rigorous, specialized, and phased post-operative rehabilitation protocol. The delicate balance achieved in the operating room can easily be destroyed by overly aggressive therapy or, conversely, by prolonged immobilization leading to insurmountable stiffness. Rehabilitation must be individualized, taking into account the patient's systemic disease activity, tissue quality, and the specific procedures performed.

Phase I: Immobilization and Tissue Protection (Days 0 to 14)
Immediately post-operatively, the hand is placed in a bulky, sterile compressive dressing supported by a custom-molded orthosis. For swan-neck corrections (FDS tenodesis), a dorsal blocking splint is fabricated to hold the PIP joints in 20 to 30 degrees of flexion, absolutely preventing any hyperextension. The MCP joints are typically positioned in 0 to 20 degrees of flexion, and the wrist in slight extension. The primary goals during this phase are strict edema control (using elevation and retrograde massage of exposed digits), pain management, and protection of the surgical repair. Active range of motion (AROM) of the uninvolved joints (shoulder, elbow) is encouraged to prevent proximal stiffness.
Phase II: Controlled Mobilization (Weeks 2 to 6)
At 10 to 14 days, sutures are removed, and the bulky dressing is discontinued. The patient
Clinical & Radiographic Imaging Archive