Surgical Management of Psoriatic and Crystal-Induced Arthropathies of the Hand

Key Takeaway
Psoriatic arthritis and crystal-induced arthropathies present complex biomechanical challenges in the hand and upper extremity. Surgical intervention is indicated for severe deformity, intractable pain, or impending tendon rupture. This guide details evidence-based operative strategies, including metacarpophalangeal resection arthroplasty, proximal interphalangeal arthrodesis, and the management of tophaceous gout, providing orthopedic surgeons with critical technical pearls for optimizing functional outcomes in inflammatory hand disease.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of inflammatory and crystal-induced arthropathies of the hand and upper extremity requires a profound understanding of joint biomechanics, soft-tissue balancing, and the underlying systemic pathophysiology. While rheumatoid arthritis (RA) remains the most extensively described inflammatory arthropathy, psoriatic arthritis (PsA), gout, and calcium pyrophosphate deposition (CPPD) disease (pseudogout) present unique patterns of joint destruction, soft-tissue compromise, and deformity. The surgical approach to these conditions must be highly individualized, as the biologic behavior of the synovium, entheses, and periarticular bone differs drastically from the classic rheumatoid paradigm.
Psoriatic arthritis is a seronegative spondyloarthropathy affecting approximately 20% to 30% of patients with cutaneous psoriasis. Unlike the predominantly synovial-driven pathology of rheumatoid arthritis, psoriatic arthritis is fundamentally a disease of the enthesis—the insertion site of tendons, ligaments, and joint capsules into bone. The inflammatory cascade is heavily mediated by the IL-23/IL-17 axis, leading to a paradoxical combination of profound osteolysis and exuberant periosteal new bone formation. This aggressive osteoclastogenesis can culminate in arthritis mutilans, a severely destructive phenotype characterized by telescoping digits ("opera-glass hand") and catastrophic loss of bone stock. Furthermore, psoriatic arthritis frequently involves the distal interphalangeal (DIP) joints, a region typically spared in rheumatoid arthritis, and is strongly associated with characteristic nail dystrophies due to the intimate anatomical relationship between the nail matrix and the terminal extensor tendon enthesis.

FIGURE 1: Common findings of psoriatic arthritis. Pitted nail deformities are a hallmark of the disease and are highly predictive of underlying distal interphalangeal joint arthropathy.
FIGURE 2: Typical psoriatic elbow lesion. Cutaneous manifestations often precede articular symptoms, though they may occur simultaneously.
Crystal-induced arthropathies, primarily gout and pseudogout, drive joint destruction through a completely different pathophysiological mechanism. Gout is characterized by the precipitation of monosodium urate (MSU) crystals in avascular tissues, such as cartilage, and relatively avascular tissues, such as tendons and ligaments. The presence of MSU crystals activates the NLRP3 inflammasome within macrophages, triggering a massive release of interleukin-1 beta (IL-1β). Chronic hyperuricemia leads to the formation of tophi—chalky, granulomatous masses of urate crystals surrounded by chronic inflammatory cells and foreign body giant cells. These tophi mechanically infiltrate and chemically degrade tendons, ligaments, and subchondral bone, leading to spontaneous tendon ruptures, compressive neuropathies, and severe erosive arthropathy. Pseudogout, driven by calcium pyrophosphate dihydrate (CPPD) crystals, frequently targets the radiocarpal joint and the triangular fibrocartilage complex (TFCC), leading to a rapid, osteoarthritis-like degenerative cascade known as scaphoid chondrocalcinosis advanced collapse (SCAC) or scapholunate advanced collapse (SLAC).
Detailed Surgical Anatomy and Biomechanics
A rigorous understanding of hand anatomy is paramount when addressing the complex deformities induced by psoriatic and crystal arthropathies. The biomechanical failure in these diseases is rarely isolated to a single structure; rather, it is a cascading failure of the skeletal architecture, capsuloligamentous restraints, and the musculotendinous units.
In the distal interphalangeal (DIP) joint, the terminal slip of the extensor mechanism inserts into the dorsal base of the distal phalanx. In psoriatic arthritis, enthesitis at this precise anatomical junction triggers an inflammatory response that readily spills over into the adjacent nail matrix, explaining the high concordance between nail pitting, onycholysis, and DIP joint erosions. The volar plate and collateral ligaments of the DIP and proximal interphalangeal (PIP) joints often become heavily fibrosed in psoriatic arthritis, leading to severe, unyielding flexion contractures. This fibrotic tendency stands in stark contrast to the ligamentous laxity and attenuation typically seen in systemic lupus erythematosus (SLE) or rheumatoid arthritis.
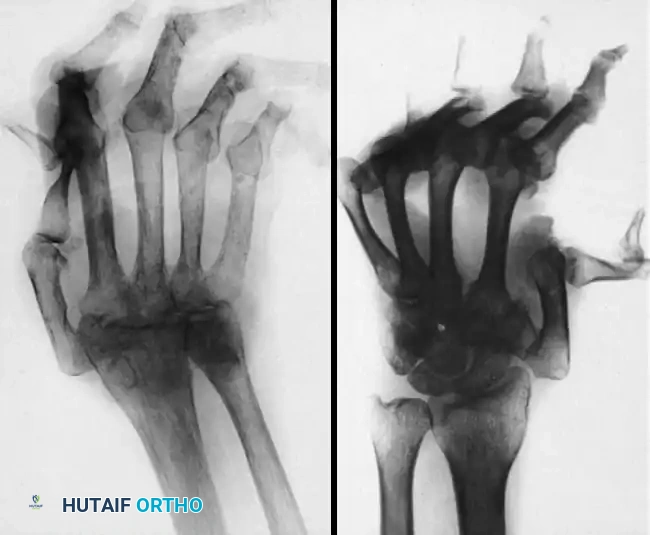
FIGURE 3: Typical radiographs of the hand and wrist in patients with systemic lupus erythematosus (SLE). Note the severe joint dislocations and ulnar drift without the erosive changes or joint space narrowing characteristic of psoriatic or rheumatoid arthritis.
The metacarpophalangeal (MCP) joints are particularly vulnerable to subluxation and dislocation in advanced psoriatic arthritis. The cam-shaped metacarpal head and the asymmetric collateral ligaments dictate that the MCP joint is loose in extension and stable in flexion. However, profound osteolysis of the metacarpal head alters this kinematic relationship, leading to volar subluxation of the proximal phalanx and ulnar drift, exacerbated by the unopposed pull of the intrinsic musculature and the ulnar shift of the extensor digitorum communis (EDC) tendons.

FIGURE 4: Severe metacarpophalangeal joint dislocations and thumb interphalangeal joint destruction in advanced psoriatic arthritis.
Vascular anatomy is of critical importance, particularly in psoriatic arthritis and tophaceous gout. The digital arteries course volar to the cleavage plane of the flexor tendon sheath. In psoriatic arthritis, chronic systemic inflammation frequently induces microvascular thrombosis and intimal hyperplasia, severely compromising digital perfusion. This can lead to ischemic fingertip ulcerations and pulp necrosis. In gout, massive tophaceous deposits physically compress the digital arteries and the common digital nerves, leading to simultaneous ischemic and neuropathic compromise. Surgical dissection in these environments must be exceptionally meticulous to preserve the tenuous remaining blood supply.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention in the setting of inflammatory or crystal arthropathy must be made collaboratively with the patient's rheumatologist. Surgery is generally reserved for structural failures that are no longer amenable to medical management. The primary goals are the alleviation of intractable pain, the restoration of functional kinematics (pinch and grasp), the prevention of impending tendon rupture, and the treatment of compressive neuropathies.
In psoriatic arthritis, the indications for surgery often center around severe stiffness, arthritis mutilans, and fixed deformities that severely limit activities of daily living. Because psoriatic joints have a high propensity for spontaneous fusion and severe stiffness, the surgical strategy often leans toward arthrodesis rather than arthroplasty, particularly in the interphalangeal joints. In gout, surgery is rarely indicated for the mere presence of hyperuricemia or small tophi; however, it becomes urgently necessary when tophi cause skin breakdown and secondary infection, acute nerve compression (e.g., carpal tunnel syndrome), or infiltration resulting in tendon attrition and rupture.
| Pathology | Primary Surgical Indications | Relative and Absolute Contraindications |
|---|---|---|
| Psoriatic Arthritis | Intractable pain refractory to biologics; progressive arthritis mutilans; severe fixed PIP/DIP contractures; MCP joint volar subluxation/dislocation; impending tendon rupture. | Active ischemic digital ulceration (Absolute); active systemic infection; uncontrolled medical comorbidities; lack of patient compliance with post-operative rehabilitation. |
| Tophaceous Gout | Acute compressive neuropathy (e.g., median/ulnar nerve); impending or actual tendon rupture (e.g., EPL); skin necrosis over massive tophi; secondary bacterial infection of an ulcerated tophus. | Asymptomatic tophi; acute gouty flare without medical optimization (Relative); severe peripheral vascular disease precluding wound healing. |
| Pseudogout (CPPD) | Severe radiocarpal/midcarpal pain refractory to injections; SLAC/SCAC wrist progression; acute carpal tunnel syndrome secondary to crystal deposition. | Advanced age with low functional demands (Relative); active septic arthritis (must differentiate from pseudogout flare via aspiration). |
Contraindications must be strictly observed to prevent catastrophic post-operative complications. Performing an elective arthroplasty or arthrodesis in a psoriatic digit with active ischemic ulceration is an absolute contraindication; the surgical wound will invariably fail to heal, and the risk of deep infection and subsequent amputation is unacceptably high. Vascular optimization and wound healing must precede any structural orthopedic reconstruction.
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning begins with a comprehensive clinical and radiographic assessment. The surgeon must meticulously document the active and passive range of motion of every joint, noting the presence of fixed contractures, tendon ruptures, and neurovascular deficits. In psoriatic arthritis, the presence of dactylitis ("sausage digits") indicates active tenosynovitis and joint inflammation, which may require concurrent tenosynovectomy during joint reconstruction.
Radiographic evaluation requires high-quality posteroanterior, lateral, and oblique views of the hand and wrist. The radiographic hallmark of psoriatic arthritis is the simultaneous presence of erosive changes and bone proliferation. The classic "pencil-in-cup" deformity—caused by severe osteolysis of the proximal phalanx head and periarticular bone proliferation at the base of the distal phalanx—must be identified, as this profound loss of bone stock dictates the type of internal fixation required for arthrodesis. Templating is critical; the surgeon must determine the precise angles for interphalangeal joint fusions to recreate a functional cascade (e.g., 40° of flexion for the index PIP, increasing by 5° for each subsequent ulnar digit). For MCP joint resection arthroplasty, templating ensures the availability of appropriately sized silicone interpositional implants.
Medical optimization is a critical phase of pre-operative planning. Biologic disease-modifying antirheumatic drugs (DMARDs), such as TNF-alpha inhibitors or IL-17 inhibitors, must be managed according to the latest American College of Rheumatology (ACR) guidelines. Typically, biologics are withheld for one dosing cycle prior to surgery to mitigate infection risk, and restarted once the surgical wound has completely healed. For gout patients, uric acid levels must be optimized with xanthine oxidase inhibitors (e.g., allopurinol) or uricosurics, and prophylactic colchicine or NSAIDs should be considered perioperatively to prevent a stress-induced acute gouty flare.
Patient positioning is standard for hand surgery: the patient is placed supine with the operative extremity extended on a radiolucent hand table. A well-padded upper arm tourniquet is applied. However, in patients with severe psoriatic microvascular disease or extensive tophaceous gout with compromised digital perfusion, the surgeon must exercise extreme caution. Exsanguination with an Esmarch bandage may be contraindicated if there is a risk of dislodging microthrombi; simple elevation prior to tourniquet inflation is preferred. Furthermore, tourniquet time should be strictly minimized to prevent exacerbating ischemic injury to the digits.
Step-by-Step Surgical Approach and Fixation Technique
Proximal Interphalangeal (PIP) Joint Arthrodesis
Due to the severe soft-tissue contractures and the inherent tendency for psoriatic joints to stiffen, restoring functional movement at the PIP joint via arthroplasty is notoriously difficult and often yields poor long-term results. Consequently, arthrodesis is the gold standard procedure for the proximal interphalangeal joint in advanced psoriatic arthritis.
1. Surgical Approach: A dorsal longitudinal or a Chamay (V-shaped) incision is utilized over the PIP joint, centered over the articulation. The skin flaps are elevated full-thickness to protect the delicate subdermal vascular plexus.
2. Extensor Mechanism Management: The extensor tendon is split longitudinally down the midline, preserving the central slip insertion if possible, though in severe deformity, it is often sacrificed. The collateral ligaments and the volar plate are sharply excised from their proximal attachments to allow complete "shotgun" exposure of the articular surfaces.
3. Joint Resection and Preparation: The articular cartilage and sclerotic subchondral bone are resected. In psoriatic arthritis, bone stock is often severely compromised. A cup-and-cone reamer system (convex reamer for the proximal phalanx head, concave for the middle phalanx base) is highly recommended. This technique maximizes cancellous bone contact area while allowing precise, multi-planar angular adjustments.
4. Positioning and Fixation: The joint is positioned in the pre-calculated functional cascade angle. Rigid fixation is paramount. Depending on the remaining bone stock, fixation is achieved using either a 1.5mm or 2.0mm headless compression screw inserted antegrade or retrograde, or crossed 0.045-inch Kirschner wires supplemented with a dorsal tension band wire if the bone is excessively osteopenic.
5. Closure: The extensor mechanism is reapproximated with non-absorbable monofilament sutures, and the skin is closed loosely to accommodate post-operative swelling.
Metacarpophalangeal (MCP) Joint Resection Arthroplasty
MCP joint deformities in psoriatic arthritis may present as severe flexion contractures or paradoxical hyperextension deformities. Resection arthroplasty utilizing silicone interpositional implants (Swanson or similar designs) remains an effective method to preserve joint motion, realign the digits, and correct ulnar drift.
1. Approach Based on Deformity (Nalebuff's Principles):
* Flexion Deformity: Approached through a standard transverse dorsal incision over the metacarpal heads. The extensor hood is incised longitudinally on the ulnar side of the EDC tendon. The metacarpal head is resected at the metaphyseal flare using an oscillating microsaw. Extensive soft-tissue releases, including the volar plate and tight collateral ligaments, are performed to correct the volar subluxation and flexion contracture.
* Hyperextension Deformity: If the MCP joint is hyperextended in conjunction with PIP joint flexion, Nalebuff recommended a palmar incision. This allows direct release of the contracted dorsal structures and volar subluxation, facilitating metacarpal head resection.
2. Canal Preparation and Implant Insertion: The medullary canals of the metacarpal and proximal phalanx are broached. Rectangular rasps are used to prevent rotational instability of the implant. A trial implant is inserted to assess tension; the implant should sit flush against the resected bone ends without buckling during full flexion or extension.
3. Soft Tissue Balancing: The radial collateral ligament is often reconstructed or reefed to prevent recurrent ulnar drift. The EDC tendon is centralized over the joint and stabilized with a radial sagittal band reefing.
Gout Tophus Excision and Tenosynovectomy
Surgical intervention for gout requires meticulous dissection due to the infiltrative nature of tophi.
1. Approach: Incisions are planned to allow extensile exposure while avoiding incisions directly over massive, poorly vascularized tophi, which can lead to skin necrosis.
2. Debulking: Complete excision of a tophus is rarely possible without sacrificing critical native structures. The goal is aggressive debulking. A scalpel and curette are used to shell out the chalky urate deposits.
3. Tenosynovectomy: When tophi infiltrate the flexor or extensor tendon sheaths, a meticulous tenosynovectomy is performed. The tendon must be inspected for attrition; if more than 50% of the tendon substance is destroyed, a primary tendon transfer (e.g., EIP to EPL) or interposition graft may be required.
4. Carpal Tunnel Decompression: If tophi are present within the carpal canal causing median neuropathy, a standard or extended carpal tunnel release is performed alongside flexor tenosynovectomy.
Complications, Incidence Rates, and Salvage Management
The complication profile in the surgical management of inflammatory and crystal arthropathies is significantly higher than in standard elective hand surgery, driven by poor bone stock, compromised soft-tissue envelopes, and profound systemic inflammation.
Stiffness is the most ubiquitous complication following psoriatic hand surgery. Despite meticulous surgical technique and aggressive post-operative therapy, the aggressive fibrotic nature of psoriatic arthritis often leads to limited range of motion. Patients must be extensively counseled pre-operatively that the primary goals are pain relief and functional positioning, not the restoration of normal kinematics.
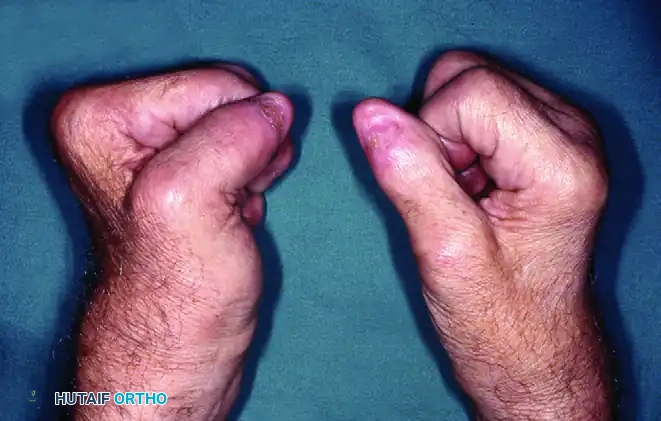
FIGURE 5: Right hand demonstrating limited finger flexion following metacarpophalangeal joint resection arthroplasty in a psoriatic patient.

FIGURE 6: The same right hand demonstrating limited finger extension. Postoperative stiffness remains a significant challenge in psoriatic arthroplasty.
Infection and wound dehiscence are major concerns, particularly in tophaceous gout where the overlying skin is attenuated and poorly vascularized. Urate crystals inhibit normal wound healing, and secondary bacterial colonization of ulcerated tophi is common.
| Complication | Estimated Incidence | Pathophysiology & Risk Factors | Salvage Management |
|---|---|---|---|
| Severe Post-Operative Stiffness | 40% - 60% (PsA Arthroplasty) | Aggressive periarticular fibrosis; enthesial inflammation; prolonged immobilization. | Intensive hand therapy; dynamic splinting; rarely, secondary surgical tenolysis/capsulotomy (often yields diminishing returns). |
| Wound Dehiscence / Necrosis | 15% - 25% (Gout Tophus Excision) | Poor dermal vascularity over tophi; microvascular thrombosis in PsA; premature suture removal. | Prolonged local wound care; healing by secondary intention; full-thickness skin grafting or local rotational flaps if critical structures are exposed. |
| Arthrodesis Nonunion | 5% - 10% | Severe osteolysis (arthritis mutilans); inadequate bone contact; failure of rigid fixation; biologic use. | Revision arthrodesis with autologous bone grafting (iliac crest or distal radius) and upgraded rigid internal fixation (e.g., locking plates). |
| Silicone Implant Fracture | 10% - 20% at 10 years | Material fatigue; recurrent deformity placing shear stress on the implant hinge. | Revision arthroplasty with implant exchange; conversion to arthrodesis if bone stock is critically depleted. |
| Ischemic Digit Loss | < 2% | Exacerbation of pre-existing microvascular disease; excessive tourniquet time; tight dressings. | Immediate removal of all dressings; dependent positioning; intra-arterial vasodilators (calcium channel blockers); digital periarterial sympathectomy; auto-amputation. |
Phased Post-Operative Rehabilitation Protocols
The post-operative management of inflammatory and crystal arthropathies requires a delicate, highly customized balance between protecting surgical repairs and preventing catastrophic stiffness. Close collaboration with a certified hand therapist (CHT) is mandatory.
Phase 1: Immobilization and Tissue Healing (Days 1 to 14)
Following PIP arthrodesis or MCP arthroplasty, the hand is immediately immobilized in the operating room in a bulky, non-compressive "boxing glove" dressing reinforced with a volar plaster splint. The wrist is held in 20° to 30° of extension. For MCP arthroplasties, the MCP joints are supported in neutral alignment to prevent recurrent volar subluxation and ulnar drift. Elevation is strictly enforced to minimize edema, which is a primary driver of post-operative fibrosis. Given the high incidence of microvascular compromise and delayed healing in psoriatic and tophaceous patients, skin sutures are left in place significantly longer than usual—typically 14 to 21 days—to prevent catastrophic wound dehiscence.
Phase 2: Early Protected Mobilization (Weeks 2 to 6)
For PIP arthrodesis, the fused joints remain continuously protected in static splints until radiographic evidence of bony union is observed, typically around 6 to 8 weeks. However, the adjacent MCP and DIP joints must be actively mobilized to prevent tethering of the flexor and extensor mechanisms.
For MCP resection arthroplasties, dynamic extension splinting is initiated within 3 to 5 days post-operatively. An outrigger splint is fabricated to guide the alignment of the developing pseudo-capsule. The dynamic slings maintain the MCP joints in full extension and neutral radial/ulnar deviation while allowing active flexion against the resistance of the rubber bands. This early motion is critical to mold the encapsulating fibrous tissue around the silicone spacer, optimizing the arc of motion.
Phase 3: Strengthening and Late Remodeling (Weeks 6 to 12+)
Once clinical and radiographic healing is confirmed, static and dynamic splints are gradually weaned. Progressive strengthening exercises, focusing on intrinsic muscle balance and grip strength, are introduced. Patients must be educated on joint protection techniques and ergonomic adaptations to prevent placing excessive shear forces on the reconstructed joints. Medical co-management with rheumatology continues seamlessly, ensuring that systemic biologic and urate-lowering therapies are optimized to prevent disease recurrence in the native and reconstructed tissues.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of these complex arthropathies is guided by decades of evolving literature and modern rheumatologic guidelines.
The foundational principles of MCP joint reconstruction were established by Swanson in the 1960s with the introduction of the flexible silicone hinge implant. Swanson's concept of "resection arthroplasty with implant interposition" revolutionized the treatment of severe MCP deformities by providing a stable spacer around which a functional pseudo-capsule could form. Nalebuff later refined the surgical approaches to complex hand deformities, particularly detailing the algorithm for addressing combined intrinsic-plus and intrinsic-minus postures, emphasizing the necessity of addressing the primary deforming force (e.g., the volar palmar approach for severe hyperextension deformities).
In the modern era, the landscape of surgical intervention has been dramatically altered by the advent of biologic DMARDs. Literature over the past two decades demonstrates a significant decline in the incidence of arthritis mutilans and the overall need for salvage arthrodesis in psoriatic patients who are successfully managed with TNF-alpha and IL-17 inhibitors. The American College of Rheumatology (ACR) and the National Psoriasis Foundation (NPF) continually update perioperative guidelines, currently recommending a nuanced approach to withholding biologics based on the specific drug's half-life, balancing the risk of perioperative infection against the risk of a severe, stiffness-inducing disease flare.
For crystal arthropathies, the European League Against Rheumatism (EULAR) and the ACR provide strict guidelines on the management of hyperuricemia. Surgical literature emphasizes that surgical debulking of tophi, while historically viewed as a last resort, is highly efficacious for preserving tendon integrity and nerve function when executed prior to catastrophic structural failure. The integration of advanced medical therapies with precise, biomechanically sound surgical reconstruction remains the cornerstone of restoring function and quality of life in patients suffering from psoriatic and crystal-induced arthropathies of the hand.
