Surgical Management of Psoriatic Arthritis and Reiter Syndrome in the Hand

Key Takeaway
Psoriatic arthritis of the hand presents unique biomechanical and surgical challenges, characterized by asymmetrical peripheral joint involvement, dactylitis, and severe interphalangeal joint destruction. Surgical intervention, primarily proximal interphalangeal joint arthrodesis, is indicated for fixed flexion contractures and instability. This guide details the clinical evaluation, radiographic hallmarks like the pencil-in-cup deformity, and step-by-step operative techniques to optimize functional outcomes while mitigating the heightened infection risks associated with psoriatic skin lesions.
Comprehensive Introduction and Patho-Epidemiology
Psoriatic arthritis (PsA) of the hand represents a formidable challenge in the realm of operative orthopedics, requiring a profound understanding of its unique patho-epidemiology to guide surgical decision-making. As a complex, chronic inflammatory arthropathy intrinsically associated with psoriasis, PsA is classified within the seronegative spondyloarthropathies. However, its manifestation in the upper extremity diverges significantly from other inflammatory conditions such as rheumatoid arthritis (RA) or degenerative conditions like osteoarthritis (OA). Epidemiologically, while psoriasis affects approximately 2% to 3% of the general population, up to 30% of these individuals will eventually develop psoriatic arthritis. Within this cohort, the presentation is highly heterogeneous. An estimated 25% of patients exhibit a polyarticular presentation that clinically mimics the symmetrical joint involvement of rheumatoid arthritis. Yet, a critical 5% to 10% of patients present with exclusive or predominant distal interphalangeal (DIP) joint involvement—a hallmark and highly specific feature of the disease that necessitates targeted surgical strategies.
The temporal relationship between the cutaneous manifestations of psoriasis and the onset of articular destruction is notoriously variable, complicating early diagnosis and intervention. In approximately 70% of cases, dermatologic manifestations precede joint symptoms, often by several years. However, in 15% to 20% of patients, the classic psoriatic skin rash develops only after the onset of arthritis (arthritis sine psoriasis). This temporal disconnect demands a high index of clinical suspicion from the hand surgeon, particularly when evaluating a patient with asymmetrical peripheral joint involvement, which is present in almost 95% of PsA cases. This marked asymmetry is a critical differentiating factor from the typically symmetrical, bilateral presentation of RA, and it fundamentally alters the biomechanical cascade of the hand, leading to unique, unilateral contractures and deformities that require highly individualized reconstructive approaches.
Reiter syndrome, now more accurately categorized within the spectrum of reactive arthritis, shares several pathophysiological pathways with PsA but possesses a distinct epidemiological and clinical profile. Classically defined by the triad of conjunctivitis, urethritis, and synovitis, reactive arthritis is typically triggered by a preceding genitourinary (e.g., Chlamydia trachomatis) or gastrointestinal (e.g., Salmonella, Shigella, Campylobacter) infection. Unlike the relatively equal gender distribution seen in PsA, reactive arthritis predominantly affects young adult males expressing the HLA-B27 antigen. The synovitis in Reiter syndrome is typically acute, asymmetrical, and oligoarticular, usually involving four or fewer joints. While it predominantly affects the large joints of the lower extremity, upper extremity involvement, including severe dactylitis and enthesitis of the hand and wrist, can occur and initially mimic acute psoriatic arthritis.
The clinical presentation of both PsA and reactive arthritis in the hand is driven by a triad of synovitis, enthesitis, and tenosynovitis. Dactylitis, colloquially known as the "sausage digit," is a classic manifestation resulting from severe, concurrent inflammation of the flexor tendon sheath and the adjacent interphalangeal joints. This diffuse swelling obliterates the normal topographical landmarks of the digit and leads to profound stiffness. Furthermore, the Kapasi, Ruby, and Calney classification system categorizes PsA patients into three distinct prognostic groups based on the temporal onset of arthritis relative to skin lesions. Type 1 is characterized by early joint involvement with late skin lesions, typically resulting in mild arthropathy. Type 2 features late joint involvement following established skin changes, often heralding a severe, rapidly progressive, and highly destructive form of arthritis (arthritis mutilans). Type 3 involves simultaneous onset, with highly unpredictable severity. Understanding these epidemiological and pathophysiological nuances is paramount for the orthopedic surgeon when determining the timing and extent of surgical intervention.
Detailed Surgical Anatomy and Biomechanics
The surgical management of the psoriatic hand requires an intimate understanding of the complex interplay between the articular structures, the extensor mechanism, and the surrounding soft-tissue envelope. In PsA, the primary anatomical epicenter of the disease is the enthesis—the insertion site of tendons, ligaments, and joint capsules into bone. The anatomical proximity of the nail matrix to the extensor tendon insertion at the distal interphalangeal (DIP) joint is of paramount clinical significance. The contiguous inflammatory process (enthesitis) spreads from the extensor terminal tendon insertion directly into the adjacent nail bed. Uniquely, the nails may separate from the nail bed (onycholysis) and exhibit a white, flaking discoloration near their distal borders. Ridging, hyperkeratosis, and pitting are common. Nalebuff observed that fingernail changes are present in approximately 15% of patients with joint involvement. Therefore, the presence of nail dystrophy strongly correlates with underlying psoriatic enthesopathy and can guide the diagnosis even in the absence of widespread cutaneous plaques.
The radiographic progression of psoriatic arthritis in the hand is characterized by a paradoxical combination of aggressive bone resorption and exuberant bone proliferation, fundamentally altering the biomechanics of the digit. Key radiographic hallmarks include acro-osteolysis (resorption of the terminal phalangeal tufts) and the classic "pencil-in-cup" deformity. This deformity arises from the severe tapering (osteolysis) of the distal ends of the phalanges and metacarpals, combined with the hypertrophic cupping (proliferation) of the proximal ends of the adjacent phalanges. Biomechanically, this results in profound multidirectional joint instability. The collateral ligaments, normally responsible for varus/valgus stability, become completely attenuated or detached as their bony insertions resorb. Furthermore, there is a strong predilection for the interphalangeal (DIP and PIP) joints, with a notable sparing of the metacarpophalangeal (MCP) joints—a pattern inverse to that typically seen in rheumatoid arthritis. In severe cases of arthritis mutilans, this osteolysis leads to the "opera-glass hand" (la main en lorgnette), where the digits become telescopically unstable and functionally useless.
Differentiating the pathoanatomy of PsA from other arthropathies is critical for accurate surgical planning. Osteoarthritis (OA) typically presents with Heberden's nodes at the DIP joints and Bouchard's nodes at the PIP joints. Biomechanically, OA is driven by asymmetrical cartilage loss, subchondral sclerosis, and marginal osteophyte formation, leading to angular deformities rather than the aggressive central erosions and multidirectional instability seen in PsA.

Fig. 70-4 Osteoarthritic hands with Heberden (distal interphalangeal) and Bouchard (proximal interphalangeal) nodes on both index fingers and thumbs. Note angular changes at distal joints as a result of loss of joint cartilage and instability.
Systemic Lupus Erythematosus (SLE) presents a different biomechanical challenge. SLE often manifests with Jaccoud's arthropathy, characterized by severe but passively reducible subluxations and dislocations. The primary pathology in SLE is capsuloligamentous laxity rather than the erosive bone destruction characteristic of PsA. Furthermore, SLE may be complicated by systemic vasculitis, leading to digital ischemia and frank necrosis of the fingertips, a vascular pathology entirely distinct from the inflammatory enthesitis of PsA.
Fig. 70-5 Vasculitis associated with lupus erythematosus resulted in necrosis of fingertips in a 33-year-old woman.
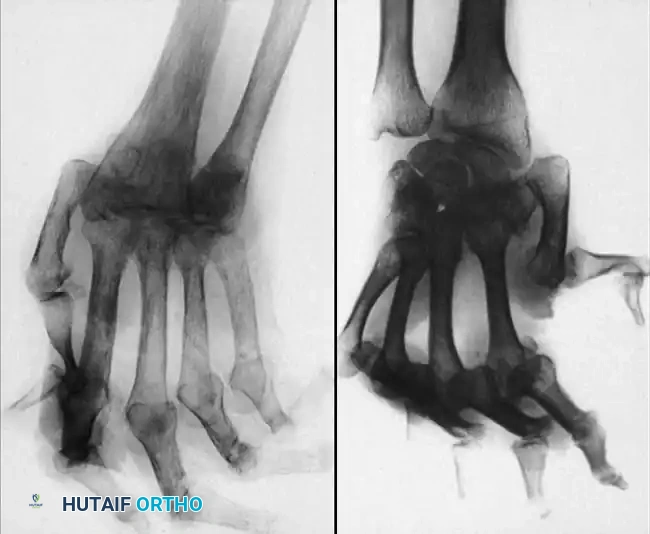
Fig. 70-6 A and B, Typical radiographs of hand and wrist in patients with systemic lupus erythematosus. Note joint dislocations without erosive changes or joint space narrowing. (From Nalebuff EA: Surgery of psoriatic arthritis of the hand, Hand Clin 12:603, 1996.)
The soft-tissue envelope in the psoriatic patient presents a unique surgical hazard. Psoriatic plaques are heavily colonized by skin flora, particularly Staphylococcus aureus. The local inflammatory milieu compromises the microvascular circulation, making the dorsal skin over the interphalangeal joints particularly vulnerable to necrosis following surgical incision. The surgeon must respect the delicate dorsal venous network; aggressive retraction or poorly planned incisions can lead to catastrophic soft-tissue breakdown, exposing underlying hardware or arthrodesis sites. This compromised soft-tissue envelope is a primary reason why silicone implant arthroplasty, often utilized in RA, is fraught with high infection rates and is generally contraindicated in the psoriatic hand.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in the psoriatic hand requires a meticulous balance between the functional deficits of the patient, the severity of articular destruction, and the state of the overlying soft-tissue envelope. Contractures of the proximal interphalangeal (PIP) joints remain the most common indication for surgical intervention. In a landmark report of 25 patients with psoriatic arthritis, Belsky et al. found PIP joint involvement in 22 patients, illustrating the stark natural history of the disease: many patients develop spontaneous fusion or fixed flexion contractures exceeding 90 degrees. Surgery is indicated when these contractures severely impede the functional cascade of the hand, preventing adequate grasp or causing recurrent skin breakdown in the palm due to the impingement of the fingertip. Additionally, profound multidirectional instability resulting from the "pencil-in-cup" deformity, which renders pinch maneuvers impossible, is an absolute indication for stabilization via arthrodesis.
In contrast, the surgical indications for Reiter syndrome (reactive arthritis) are exceedingly rare. The natural history of Reiter syndrome is generally favorable, with approximately 90% of patients experiencing a complete remission of symptoms after several weeks to months of conservative management utilizing nonsteroidal anti-inflammatory drugs (NSAIDs), targeted physical therapy, and occasionally intra-articular corticosteroid injections. The disease is primarily characterized by acute inflammation rather than structural destruction in its early phases. Operative intervention in Reiter syndrome is reserved strictly for the small minority (approximately 10%) of chronic patients who develop fixed, debilitating contractures or severe secondary osteoarthritis after years of persistent, refractory inflammation. In these rare chronic cases, the surgical principles and techniques mirror those applied to end-stage psoriatic arthritis.
Contraindications to surgery in the psoriatic hand are heavily influenced by dermatological and systemic factors. The presence of active, scaling psoriatic plaques directly over the planned surgical incision is a strict contraindication due to the unacceptably high risk of postoperative surgical site infection. Nalebuff strongly recommended scheduling elective surgical procedures for psoriatic arthritis during the summer months; ultraviolet exposure typically causes psoriatic skin lesions to regress, thereby significantly reducing colonization and infection risk. Furthermore, active systemic infections, profound immunosuppression (often secondary to biologic disease-modifying antirheumatic drugs [DMARDs]), and a lack of patient compliance regarding postoperative immobilization and rehabilitation are significant contraindications.
| Category | Psoriatic Arthritis (PsA) | Reiter Syndrome (Reactive Arthritis) |
|---|---|---|
| Primary Indications | Fixed PIP flexion contractures (>60-90 degrees); Multidirectional instability ("pencil-in-cup"); Pain refractory to maximal biologic/DMARD therapy; Spontaneous ankylosis in non-functional positions. | Chronic, fixed contractures failing prolonged conservative therapy; Severe secondary osteoarthritis in the late, destructive phase (rare, <10% of patients). |
| Surgical Procedures | PIP/DIP Arthrodesis (Gold Standard); Tenosynovectomy for severe dactylitis; Tendon transfers for extensor ruptures. | Arthrodesis (only in chronic destructive phase); Synovectomy/Debridement (exceedingly rare). |
| Absolute Contraindications | Active psoriatic plaques over the surgical incision; Active systemic infection; Severe vascular compromise of the digit. | Acute inflammatory phase of the disease; Active genitourinary or gastrointestinal infection; Spontaneous remission expected. |
| Relative Contraindications | Silicone implant arthroplasty (due to high infection risk); Uncontrolled systemic disease requiring high-dose immunosuppression; Poor patient compliance. | Oligoarticular presentation responding to NSAIDs; Mild enthesitis without structural joint destruction. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful surgical outcomes in the psoriatic hand. The initial clinical assessment must go beyond evaluating joint mobility and stability; it requires a comprehensive dermatological survey. The surgeon must map the location of active psoriatic plaques and assess the quality of the skin over the dorsal interphalangeal joints. If plaques are present near the surgical site, preoperative coordination with a dermatologist to optimize topical or systemic therapy is mandatory. Furthermore, the patient's current pharmacological regimen, particularly the use of biologic agents (e.g., TNF-alpha inhibitors, IL-17 inhibitors), must be carefully reviewed. While guidelines vary, many institutions recommend holding certain biologic agents for one to two dosing cycles prior to elective bony procedures to mitigate the risk of deep infection, balancing this against the risk of a systemic disease flare.
Radiographic templating is critical due to the highly variable bone stock encountered in PsA. Standard posteroanterior, true lateral, and oblique radiographs of the hand are obtained. The surgeon must meticulously assess the degree of osteolysis versus sclerosis. In digits exhibiting the "pencil-in-cup" deformity, the medullary canal of the proximal phalanx may be entirely obliterated by sclerotic bone, while the middle phalanx may be profoundly osteopenic. Templating involves selecting the appropriate size of Kirschner wires (typically 0.035 or 0.045 inches) or headless compression screws (ranging from 1.5 mm to 2.4 mm). If screw fixation is planned, the surgeon must ensure that the remaining bone stock is sufficient to achieve adequate thread purchase; if the bone is severely osteopenic or the canal is excessively wide, tension band wiring or crossed K-wires may be the more prudent biomechanical choice.
Patient positioning and anesthesia are standardized to optimize surgical efficiency and safety. The patient is placed supine on the operating table with the operative arm extended on a rigid, radiolucent hand table to facilitate intraoperative fluoroscopy. Regional anesthesia, typically an ultrasound-guided axillary or supraclavicular brachial plexus block, is preferred over general anesthesia as it provides excellent intraoperative operating conditions, preemptive analgesia, and profound postoperative pain control, which facilitates early rehabilitation. A well-padded pneumatic tourniquet is applied to the upper arm. Following exsanguination of the limb using an Esmarch bandage, the tourniquet is inflated to 250 mm Hg (or 100 mm Hg above the patient's systolic blood pressure).
Meticulous skin preparation is a critical step in mitigating the heightened infection risk in this patient population. Chlorhexidine-alcohol solutions are generally preferred over iodine-based solutions due to their superior residual antimicrobial activity. However, the surgeon must take immense care to gently prep over any dormant psoriatic plaques without causing mechanical abrasion. Scrubbing these areas aggressively can induce the Koebner phenomenon—the development of new psoriatic lesions at sites of skin trauma—which can severely complicate wound healing. The hand is then draped in a standard sterile fashion, leaving the fingertips exposed to assess capillary refill upon tourniquet deflation.
Step-by-Step Surgical Approach and Fixation Technique
Because implant arthroplasty carries an unacceptably high risk of periprosthetic infection and early mechanical failure in the psoriatic hand, proximal interphalangeal (PIP) and distal interphalangeal (DIP) joint arthrodesis remains the absolute gold standard for achieving a stable, painless, and functional digit. The goal of PIP arthrodesis is to provide a stable post for pinch and grasp. The angle of fusion must be meticulously tailored to the specific digit to optimize the functional cascade of the hand: typically, the index finger is fused at 35 to 40 degrees of flexion, the long finger at 45 degrees, the ring finger at 50 degrees, and the small finger at 55 to 60 degrees. DIP joints are generally fused in 0 to 10 degrees of flexion.
The surgical approach begins with a dorsal longitudinal or a dorsal lazy-S incision centered over the PIP joint. The lazy-S incision is often preferred as it reduces the risk of linear scar contracture over the joint dorsal surface. Full-thickness skin flaps, including the subcutaneous tissue and the delicate dorsal venous network, are carefully elevated. Dissection must be precise to avoid devascularizing the thin dorsal skin. The extensor mechanism is thus exposed. A longitudinal tenotomy is performed directly through the central slip of the extensor tendon, splitting it down the midline to expose the underlying joint capsule. The capsule is incised, and the collateral ligaments are sharply excised from their proximal attachments on the proximal phalanx. This complete release is essential to allow for full joint exposure, hyperflexion, and mobilization of the articular surfaces.
Joint preparation requires aggressive debridement, particularly in cases of severe "pencil-in-cup" deformity. The remaining sclerotic, eburnated bone must be resected to expose healthy, bleeding cancellous bone, which is a prerequisite for successful arthrodesis. Using an oscillating microsaw or manual rongeurs, the articular surfaces of the proximal and middle phalanges are removed. A "cup and cone" reaming technique is highly recommended. This involves using a convex reamer on the proximal phalanx and a concave reamer on the middle phalanx. The cup and cone method provides superior bony apposition, maximizes the surface area for osteogenesis, and, crucially, allows the surgeon to fine-tune the flexion angle and rotational alignment in a multi-axial fashion prior to definitive fixation. Alternatively, flat opposing cuts can be utilized, though this requires precise angular saw cuts to achieve the desired flexion cascade.
Rigid internal fixation is critical due to the poor bone stock often encountered. Two primary techniques are utilized: tension band wiring and headless compression screws.
* Tension Band Wiring: Two parallel 0.035-inch Kirschner wires are driven antegrade through the middle phalanx, exiting distally. The joint is reduced at the predetermined angle, and the wires are driven retrograde into the proximal phalanx. A 24-gauge stainless steel wire is then passed through a transverse drill hole made 1 cm proximal to the fusion site in the proximal phalanx. The wire is looped in a figure-of-eight fashion over the protruding dorsal ends of the K-wires and tightened to provide dynamic compression across the arthrodesis site. The K-wires are cut short and bent to prevent migration.
* Headless Compression Screws: If the medullary canal diameter and bone stock permit, a single axial headless compression screw provides excellent rigid fixation. A guide wire is passed centrally across the reduced joint, the length is measured, and the appropriate screw is advanced until the trailing head is completely buried beneath the subchondral bone. This technique eliminates the issue of prominent hardware irritating the thin dorsal skin.
Following rigid fixation and fluoroscopic confirmation of alignment, the wound is irrigated. The extensor mechanism (central slip) is reapproximated using 4-0 absorbable sutures to cover the hardware. The skin is closed with 4-0 or 5-0 non-absorbable monofilament sutures using a tension-free technique. A bulky, non-adherent soft dressing is applied, followed by a well-molded volar plaster splint immobilizing the digit in the fused position.
Complications, Incidence Rates, and Salvage Management
The surgical management of the psoriatic hand is fraught with potential complications, driven by the systemic inflammatory nature of the disease, the compromised soft-tissue envelope, and the frequently poor bone stock. Infection is the most feared and arguably the most common severe complication. Belsky et al. explicitly warned that the risk of deep periprosthetic infection is significantly higher after implant arthroplasty in PsA patients compared to those with rheumatoid disease, approaching 15% to 20% in some historical cohorts. Even with arthrodesis, superficial surgical site infections occur at a higher rate than in the general population due to the colonization of psoriatic plaques by Staphylococcus aureus. Meticulous preoperative skin care and the avoidance of incisions through active plaques are critical preventative measures.
Nonunion and delayed union represent significant mechanical complications. The incidence of nonunion following PIP arthrodesis in the psoriatic hand ranges from 5% to 12%, largely attributable to the sclerotic, avascular nature of the bone in advanced disease (the "pencil" portion of the pencil-in-cup deformity) and the concurrent use of biologic or systemic DMARD therapies that may impair osteogenesis. Hardware failure, including K-wire migration or breakage, is also a risk, particularly if the tension band construct is inadequate or if the patient is non-compliant with postoperative immobilization. Furthermore, the thin dorsal skin is highly susceptible to necrosis or breakdown over prominent K-wires, necessitating hardware removal once clinical union is achieved.
Salvage management for these complications requires a stepwise, aggressive approach. Superficial infections are managed with targeted oral antibiotics and local wound care. Deep space infections or osteomyelitis require immediate operative debridement, hardware removal, and the placement of an antibiotic spacer, followed by a prolonged course of intravenous antibiotics directed by deep tissue cultures. Once the infection is eradicated, revision arthrodesis with autologous bone grafting (typically harvested from the distal radius or iliac crest) and robust internal fixation (e.g., a locking mini-plate) is required. For aseptic nonunions, revision surgery involves taking down the pseudoarthrosis, aggressive re-debridement to bleeding bone, structural bone grafting, and upgrading the fixation construct to a compression screw or plate if bone stock allows.
| Complication | Estimated Incidence in PsA | Preventative Measures | Salvage Management |
|---|---|---|---|
| Superficial Skin Infection | 5% - 10% | Avoid incising through active plaques; operate in summer months; chlorhexidine prep. | Oral antibiotics (anti-staphylococcal); local wound care; close observation. |
| Deep Infection / Osteomyelitis | 2% - 5% (Arthrodesis) >15% (Arthroplasty) |
Hold specific biologics perioperatively; meticulous sterile technique; prophylactic IV antibiotics. | Immediate hardware removal; aggressive surgical debridement; IV antibiotics; delayed revision with bone graft. |
| Nonunion / Delayed Union | 5% - 12% | "Cup and cone" aggressive debridement to bleeding bone; rigid compression fixation. | Revision arthrodesis; structural autograft (distal radius/iliac crest); upgraded rigid fixation (plate/screw). |
| Hardware Prominence / Skin Necrosis | 10% - 15% (with K-wires) | Bury K-wire ends deep to extensor tendon; utilize headless compression screws when possible. | Local wound care; early hardware removal once radiographic union is confirmed (typically 6-8 weeks). |
| Malunion / Improper Cascade | 3% - 5% | Precise intraoperative templating; fluoroscopic confirmation of cascade prior to definitive fixation. | Corrective closing wedge osteotomy and revision internal fixation if functionally limiting. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation of the psoriatic hand following arthrodesis requires a delicate balance between protecting the surgical construct and preventing profound stiffness in the adjacent, non-operated joints. The rehabilitation protocol is generally divided into three distinct phases, requiring close collaboration between the orthopedic surgeon and a specialized certified hand therapist (CHT).
Phase I: Protection and Edema Control (Weeks 0 to 4)
Immediately postoperatively, the digit is immobilized in a bulky soft dressing and a rigid volar plaster splint. The primary goals during this phase are the protection of the arthrodesis site, strict edema control, and the promotion of wound healing. The hand must be kept elevated above the level of the heart to minimize dependent swelling, which can severely compromise the dorsal skin flaps. At 10 to 14 days, the initial dressing is removed, sutures are extracted, and a custom-fabricated thermoplastic splint is applied. This splint immobilizes the fused joint but should be designed to allow free active range of motion (AROM) of the metacarpophalangeal (MCP) and distal interphalangeal (DIP) joints (if not fused). Patients are instructed to perform hourly AROM exercises of the uninvolved joints to prevent secondary contractures and promote tendon gliding. If K-wires are left exposed percutaneously, meticulous pin tract care using half-strength hydrogen peroxide or chlorhexidine is initiated to prevent superficial infections.
Phase II: Clinical Union and Transition (Weeks 4 to 8)
At approximately 4 to 6 weeks postoperatively, clinical union is assessed. The presence of a painless, stable joint to gentle manual stress, combined with early bridging trabeculae on follow-up radiographs, marks the transition to Phase II. The rigid thermoplastic splint is gradually weaned, initially transitioning to buddy taping to the adjacent digit for lateral support during daily activities. The splint may still be worn at night or during high-risk activities. Active and active-assisted range of motion exercises for the entire hand are intensified. Gentle passive range of motion (PROM) can be initiated for the adjacent, non-operated joints, but aggressive passive stretching across the arthrodesis site is strictly avoided. Modalities such as fluidotherapy or paraffin baths may be utilized by the hand therapist to address persistent stiffness and improve tissue compliance.
Phase III: Strengthening and Return to Function (Weeks 8 to 12+)
By 8 to 12 weeks, solid radiographic union is typically observed. If percutaneous K-wires were utilized, they are routinely removed in the clinic at this stage. The focus of therapy shifts toward progressive strengthening and the restoration of functional grip and pinch mechanics. Isometric strengthening exercises are introduced, progressing to dynamic strengthening using therapeutic putty and hand grippers. Patients must be counseled extensively regarding their expected outcomes; while the arthrodesis provides a stable, painless post, the overall dexterity and grip strength of the hand will be permanently altered. Occupational therapy focuses on adaptive strategies and ergonomic modifications for activities of daily living. For patients with Reiter syndrome who underwent surgery for chronic deformities, the rehabilitation protocol is similar, though concurrent management of systemic enthesitis (e.g., Achilles tendinitis, plantar fasciitis) by physical therapy remains a critical component of their overall functional recovery.
Summary of Landmark Literature and Clinical Guidelines
The surgical management algorithms for psoriatic arthritis and Reiter syndrome in the hand have been shaped by several decades of landmark orthopedic literature and evolving rheumatological guidelines. The foundational understanding of surgical indications in PsA is heavily derived from the seminal work of Belsky, Feldon, Millender, and Nalebuff. In their classic retrospective reviews, they delineated the natural history of the psoriatic hand, highlighting the rapid progression to spontaneous fusion or severe flexion contractures of the PIP joints. Crucially, Belsky et al. provided the definitive warning against the use of silicone implant arthroplasty in this patient population. Their documentation of unacceptably high infection rates and early mechanical failure solidified PIP and DIP joint arthrodesis as the enduring gold standard—a paradigm that remains largely unchallenged in contemporary hand surgery.
Dr. Edward Nalebuff further refined the clinical approach to the psoriatic hand by identifying key diagnostic and prognostic markers. He was instrumental in correlating the presence of fingernail changes (pitting, onycholysis) with underlying distal interphalangeal joint enthesopathy. Furthermore, Nalebuff introduced the highly practical, though unconventional, clinical pearl of scheduling elective reconstructive procedures during
