Comprehensive Surgical Management of Arthritic Hand Disorders: Osteoarthritis, Rheumatoid, and Psoriatic Pathologies
Key Takeaway
Osteoarthritis is the most prevalent arthritic hand disorder, frequently affecting the trapeziometacarpal and interphalangeal joints. Surgical management requires a deep understanding of joint biomechanics, ligamentous integrity, and progressive deformity patterns. This guide details the pathophysiology, radiographic hallmarks, and step-by-step operative interventions for osteoarthritis, rheumatoid arthritis, and psoriatic arthritis of the hand, providing orthopedic surgeons with evidence-based protocols for arthroplasty, arthrodesis, and soft-tissue reconstruction to restore optimal hand function.
Comprehensive Introduction and Patho-Epidemiology
Arthritic disorders of the hand and wrist encompass a diverse spectrum of pathologies, primarily dominated by osteoarthritis (OA), rheumatoid arthritis (RA), and psoriatic arthritis (PsA). Each of these entities presents with a distinct patho-epidemiological profile, dictating unique patterns of joint destruction, soft-tissue attenuation, and subsequent biomechanical failure. Osteoarthritis represents the most ubiquitous arthritic condition affecting the upper extremity. While traditionally conceptualized as a purely mechanical "wear-and-tear" phenomenon, contemporary epidemiological data reveals a profound genetic and systemic biomechanical predisposition. The condition frequently presents unilaterally but demonstrates an equal predilection for the minor (non-dominant) hand as the dominant hand. The trapeziometacarpal (carpometacarpal or CMC) joint of the thumb is the most frequently surgically treated osteoarthritic joint, predominantly afflicting postmenopausal women. This demographic predilection suggests a hormonal component to capsuloligamentous laxity, which precipitates early articular shear and subsequent chondral degradation. Osteoarthritic degeneration is histologically characterized by progressive cartilage fragmentation, subchondral sclerosis, and marginal osteophyte formation. Clinically, these manifest as Heberden nodes at the distal interphalangeal (DIP) joints and Bouchard nodes at the proximal interphalangeal (PIP) joints, frequently accompanied by mucoid cysts that can induce secondary nail bed deformities due to germinal matrix compression.

FIGURE 73-4 Osteoarthritic hands with Heberden (distal interphalangeal) and Bouchard (proximal interphalangeal) nodes on both index fingers and thumbs. Note angular changes at distal joints as a result of loss of joint cartilage and instability.
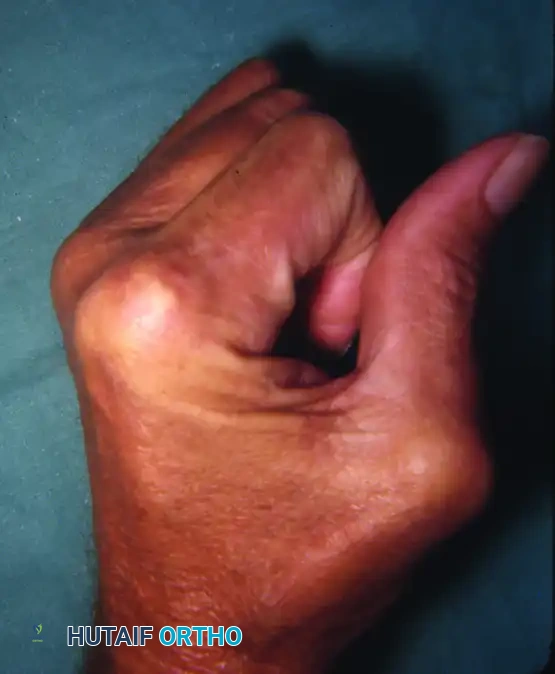
In stark contrast to the hypertrophic bone formation seen in OA, rheumatoid arthritis is a systemic autoimmune diathesis characterized by aggressive, erosive synovial hypertrophy known as pannus. This hyperplastic synovium acts as an invasive tumor-like tissue, releasing matrix metalloproteinases and inflammatory cytokines (TNF-alpha, IL-1, IL-6) that systematically decimate articular cartilage, subchondral bone, and critical capsuloligamentous constraints. The epidemiological footprint of RA shows a strong female preponderance, typically manifesting in the fourth to fifth decades of life. The disease is characterized by symmetrical polyarticular involvement. In the hand, this translates to profound biomechanical imbalances, leading to classic deformities. The profound osteolysis and structural collapse seen in end-stage erosive rheumatoid disease (arthritis mutilans) lead to the "main en lorgnette" or opera glass hand, where phalanges and metacarpals telescope into one another, creating redundant, wrinkled skin folds.
FIGURE 73-3 “Main en lorgnette” (opera glass hand). Late changes in progressive rheumatoid arthritis.
Psoriatic arthritis introduces a third, highly distinct inflammatory arthropathy, presenting a unique diagnostic and therapeutic challenge. Approximately 15% to 20% of patients develop the characteristic psoriatic skin plaques only after the onset of articular symptoms, necessitating a high index of clinical suspicion. Unlike RA, PsA is characterized by asymmetrical peripheral joint involvement and a profound predilection for the interphalangeal joints (DIP and PIP), often sparing the metacarpophalangeal (MCP) joints. The patho-epidemiology of PsA is defined by a paradoxical combination of severe osteolysis and florid bone proliferation. This manifests radiographically as acro-osteolysis of the terminal tufts and the pathognomonic "pencil-in-cup" deformity. Furthermore, the inflammatory cascade in PsA extends beyond the synovium to involve the entheses, leading to dactylitis ("sausage digits") and severe tenosynovitis. Kapasi, Ruby, and Calney classified PsA into three distinct temporal phenotypes: Type 1 (early joint, late skin involvement; generally mild), Type 2 (early skin, late joint involvement; severe destructive arthritis), and Type 3 (simultaneous onset; highly unpredictable destruction). Recognizing these distinct patho-epidemiological profiles is the foundational step in formulating an effective, individualized surgical strategy.
Detailed Surgical Anatomy and Biomechanics
A profound comprehension of the intricate surgical anatomy and biomechanics of the hand and wrist is paramount for the reconstructive surgeon. The trapeziometacarpal (CMC) joint of the thumb is a highly specialized biconcave-convex saddle joint. This unique geometric configuration permits a vast spatial arc of motion, encompassing flexion, extension, abduction, adduction, and opposition. However, this extensive mobility comes at the cost of inherent osseous stability. The joint relies heavily on a robust capsuloligamentous complex, most notably the anterior oblique ligament (commonly referred to as the volar beak ligament) and the dorsoradial ligament. Biomechanical studies have demonstrated that pinch forces generated at the tips of the digits are magnified up to 12-fold at the CMC joint. Consequently, attenuation of the volar beak ligament leads to dorsal and radial subluxation of the first metacarpal base. This subluxation alters the contact mechanics, concentrating massive shear forces on the volar-ulnar aspect of the trapezium, precipitating the classic pattern of chondral wear, subchondral sclerosis, and osteophyte formation seen in Eaton-Littler Stage II and III disease.
In the rheumatoid hand, the biomechanical collapse is driven by synovial infiltration and subsequent failure of specific anatomical constraints. Thumb deformities in RA are meticulously classified by Nalebuff, illustrating the predictable cascade of biomechanical failure. The Type I (Boutonnière) deformity, the most prevalent, initiates with synovitis at the metacarpophalangeal (MCP) joint. The hypertrophic pannus attenuates the extensor pollicis brevis (EPB) insertion and the dorsal capsule. Deprived of its dorsal constraints, the proximal phalanx subluxates volarly, establishing a fixed MCP joint flexion contracture. This volar migration alters the vector of the extensor pollicis longus (EPL) tendon, which subluxates ulnarly and volarly. The EPL's extension moment is consequently transferred entirely to the interphalangeal (IP) joint, driving it into severe hyperextension. Conversely, the Type III (Swan-Neck) deformity originates at the CMC joint. Synovitic destruction of the CMC capsule leads to dorsal-radial subluxation of the metacarpal base. To compensate for the resulting adduction contracture of the first ray, the patient forcibly hyperextends the MCP joint, which subsequently induces a secondary flexion deformity at the IP joint.

FIGURE 73-2 Thumb with fixed rheumatoid boutonnière deformity with metacarpophalangeal flexion and interphalangeal hyperextension (type I deformity).
The wrist serves as the critical functional foundation for the hand, and its biomechanical destruction in RA is particularly devastating. Carpal instability is initiated by synovitic disruption of the intrinsic and extrinsic intercarpal ligaments, most critically the radioscaphocapitate ligament. This failure precipitates rotatory subluxation of the scaphoid and subsequent carpal collapse. Concurrently, as the radiocarpal ligaments fail, the natural 22-degree ulnar inclination of the distal radius mechanically drives the entire carpus into ulnar translocation. At the distal radioulnar joint (DRUJ), destruction of the stabilizing ligaments (the triangular fibrocartilage complex and radioulnar ligaments) leads to Caput Ulnae Syndrome. The ulnar head dislocates dorsally, the carpus supinates, and the extensor carpi ulnaris (ECU) tendon subluxates volarly, losing its mechanical advantage as a wrist extensor. The eroded, prominent ulnar head functions as an internal abrasive saw against the overlying extensor tendons, frequently precipitating sequential attritional ruptures (Vaughan-Jackson syndrome), classically initiating at the extensor digiti minimi (EDM) and progressing radially to involve the common extensors.
Exhaustive Indications and Contraindications
The decision-making process for surgical intervention in arthritic hand disorders requires a meticulous balancing of patient symptomatology, functional demands, radiographic staging, and the specific underlying pathology. In osteoarthritis, surgery is primarily indicated for pain that is refractory to comprehensive conservative management, including rigid splinting, nonsteroidal anti-inflammatory drugs (NSAIDs), activity modification, and fluoroscopically guided intra-articular corticosteroid or hyaluronic acid injections. For CMC joint OA, the Eaton-Littler classification guides surgical indications. Stage I and early Stage II disease may be amenable to extra-articular ligament reconstruction or arthroscopic debridement. However, advanced Stage III (significant joint space narrowing, cystic changes, and osteophytes) and Stage IV (pan-trapezial involvement including the scaphotrapezial joint) are absolute indications for trapeziectomy with or without ligament reconstruction and tendon interposition (LRTI). DIP and PIP joint OA with severe pain, instability, or angular deformity are indications for arthrodesis or, in highly selected PIP cases, implant arthroplasty.
In rheumatoid arthritis, surgical indications are categorized into prophylactic, reconstructive, and salvage procedures. Prophylactic tenosynovectomy is urgently indicated when massive synovial proliferation threatens tendon integrity, particularly in the presence of dorsal wrist swelling that does not resolve with aggressive disease-modifying antirheumatic drug (DMARD) therapy. Caput Ulnae Syndrome with impending or actual tendon rupture is an absolute indication for a Darrach procedure (distal ulna resection) or a Sauvé-Kapandji procedure, combined with extensor tendon transfer or grafting. Reconstructive indications include severe ulnar drift and volar subluxation of the MCP joints, which profoundly impair grip and pinch mechanics; these are optimally managed with silicone implant arthroplasty (Swanson implants). Salvage procedures, such as total wrist arthrodesis, are indicated for end-stage pan-carpal destruction with severe pain and fixed deformity, prioritizing a stable, painless post over motion.
Psoriatic arthritis presents unique surgical indications driven by the rapid, destructive nature of the disease and severe soft-tissue contractures. The profound joint tropism for the PIP and DIP joints, combined with the propensity for spontaneous ankylosis in non-functional positions, frequently necessitates surgical correction. Arthrodesis is the workhorse procedure for PsA of the small joints. Implant arthroplasty is generally contraindicated in the PIP joints of PsA patients due to compromised bone stock (pencil-in-cup osteolysis), severe soft-tissue contractures, and an unacceptably high risk of deep postoperative infection secondary to skin flora colonization in psoriatic plaques.
Surgical Indications and Contraindications Matrix
| Pathology | Primary Surgical Indications | Relative Contraindications | Absolute Contraindications |
|---|---|---|---|
| Osteoarthritis (CMC) | Eaton-Littler Stage III/IV refractory to conservative care; severe rest pain; adduction contracture. | Moderate asymptomatic radiographic disease; non-compliant patient. | Active local infection; profound complex regional pain syndrome (CRPS). |
| Osteoarthritis (DIP/PIP) | Painful instability; severe angular deformity; recurrent mucoid cysts with nail bed deformity. | High functional demand for fine PIP motion (relative for fusion). | Active paronychia or felon; inadequate soft tissue coverage. |
| Rheumatoid Arthritis | Extensor tendon rupture (Vaughan-Jackson); Caput Ulnae Syndrome; severe MCP ulnar drift; fixed Nalebuff thumb deformities. | Poor medical optimization; active systemic flare; profound osteopenia (for certain implants). | Active joint infection; complete absence of motor units for tendon transfer. |
| Psoriatic Arthritis | Painful spontaneous ankylosis in non-functional position; severe PIP flexion contractures; dactylitis-induced tendon rupture. | Active, florid psoriatic plaques over the proposed surgical incision site. | Active local infection; severe acro-osteolysis precluding hardware purchase. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful reconstructive hand surgery, demanding meticulous clinical evaluation, advanced imaging, and strategic medical optimization. For trapeziometacarpal osteoarthritis, a dedicated radiographic series is mandatory. This must include a true anteroposterior (AP) view of the CMC joint (Robert's view) and a stress view to accurately assess the degree of radial subluxation and articular wear. The presence of scaphotrapezial-trapezoid (STT) joint arthritis must be definitively identified, as failure to recognize pan-trapezial disease will result in persistent postoperative pain if an isolated CMC arthroplasty is performed. In cases of rheumatoid and psoriatic arthritis, full hand and wrist series, including Brewerton views to assess early marginal erosions at the metacarpal heads, are essential. When planning for MCP or PIP joint arthroplasty using silicone implants, preoperative digital templating is required to estimate the appropriate implant size, ensuring the intramedullary stems will not excessively ream the attenuated cortices, which could precipitate intraoperative iatrogenic fractures.
Medical optimization in the inflammatory arthropathies requires close multidisciplinary collaboration with a rheumatologist. The perioperative management of DMARDs and biologic agents (e.g., TNF-alpha inhibitors, IL-17 inhibitors) is a critical consideration. While traditional guidelines advocated for the cessation of biologics prior to surgery to mitigate infection risk, contemporary evidence suggests that maintaining certain therapies may prevent severe postoperative disease flares that could equally compromise rehabilitation and soft-tissue healing. The precise timing of surgery is also an underappreciated variable, particularly in psoriatic arthritis. It is highly recommended to schedule elective surgical procedures for PsA patients during the summer months. Increased ambient ultraviolet (UV) light exposure during this season induces the regression of psoriatic skin lesions, thereby significantly reducing the local bacterial load (particularly Staphylococcus aureus colonization) and mitigating the elevated risk of perioperative surgical site infections.
Patient positioning and anesthesia are standardized to optimize surgical efficiency and patient safety. The patient is positioned supine on the operating table with the operative extremity extended onto a radiolucent hand table. Regional anesthesia, specifically a supraclavicular or axillary brachial plexus block, is the modality of choice, providing excellent intraoperative muscle relaxation and profound postoperative analgesia, thereby minimizing the need for systemic opioids. General anesthesia is reserved for patients with contraindications to regional blocks or those undergoing extensive, bilateral, or prolonged multi-joint reconstructions. A well-padded pneumatic tourniquet is applied to the proximal arm, typically inflated to 250 mmHg or 100 mmHg above the patient's systolic blood pressure, following exsanguination of the limb with an Esmarch bandage. Meticulous skin preparation with chlorhexidine-alcohol or povidone-iodine is performed, paying special attention to the web spaces and nail folds.
Step-by-Step Surgical Approach and Fixation Technique
Trapeziometacarpal Arthroplasty (LRTI) for Osteoarthritis
The Ligament Reconstruction and Tendon Interposition (LRTI) utilizing the flexor carpi radialis (FCR) remains a gold-standard reconstructive option for advanced CMC osteoarthritis.
1. Incision and Exposure: A Wagner or modified dorsal-radial curvilinear incision is utilized, centered over the CMC joint. The incision is carefully deepened through the subcutaneous tissues.
2. Nerve Protection: Meticulous dissection is paramount to identify, neurolyse, and gently retract the terminal sensory branches of the superficial radial nerve dorsally and the lateral antebrachial cutaneous nerve volarly. Retraction neuropraxia here is a common source of postoperative morbidity.
3. Capsulotomy and Trapeziectomy: A longitudinal or T-shaped capsulotomy is performed. The trapezium is typically firmly seated and surrounded by osteophytes. It is systematically fragmented using a sharp osteotome or rongeur and excised piecemeal. Surgical Warning: En bloc resection risks catastrophic injury to the underlying FCR tendon within its fibro-osseous groove. Furthermore, failure to adequately clear the medial osteophytes of the trapezium can lead to impingement against the index metacarpal base, resulting in persistent postoperative pain. Complete pan-trapezial clearance must be visually and fluoroscopically confirmed.
4. Tendon Harvest: The FCR tendon is harvested through a series of step-ladder transverse incisions in the volar forearm. The tendon is divided proximally at the musculotendinous junction and delivered into the CMC wound, leaving its critical distal insertion at the base of the second metacarpal intact.
5. Ligament Reconstruction: A drill hole (typically 3.2mm to 4.0mm) is created in the dorsal-radial base of the first metacarpal, directed from the articular surface exiting dorsally. The harvested FCR tendon is passed through this osseous tunnel from volar to dorsal. The first metacarpal is anatomically reduced, and the tendon is rigidly tensioned and sutured to the dorsal periosteum and capsule, effectively reconstructing the deficient volar beak ligament.
6. Interposition and Closure: The redundant length of the FCR tendon is folded upon itself to create an "anchovy" spacer. This is sutured into the trapeziectomy void to prevent proximal migration and subsidence of the first metacarpal. The dorsal capsule is meticulously repaired to augment stability.
Rheumatoid Wrist Reconstruction: Dorsal Tenosynovectomy and Darrach Procedure
For the rheumatoid patient presenting with Caput Ulnae Syndrome and impending extensor tendon rupture, prompt intervention is required.
1. Approach: A dorsal longitudinal incision is made in the midline of the wrist. Thickened subcutaneous tissue is elevated.
2. Retinaculum and Tenosynovectomy: The extensor retinaculum is divided, typically stepping the incision to preserve a portion of the extensor retinaculum (often the 6th compartment) to subsequently relocate and stabilize the ECU tendon. A radical tenosynovectomy is performed across all extensor compartments, meticulously excising the invasive pannus from the tendon substance while preserving the paratenon where possible.
3. Distal Ulna Resection (Darrach): The distal radioulnar joint capsule is opened. The distal ulna is subperiosteally exposed. An oscillating saw is used to resect the distal 1.5 to 2.0 cm of the ulna. The resection must be proximal to the sigmoid notch but conservative enough to prevent severe instability of the remaining ulnar stump. The volar capsule is repaired over the ulnar stump to interpose tissue between the bone and the carpus.
4. Tendon Repair/Transfer: If attritional ruptures are present (Vaughan-Jackson), side-to-side tenodesis of the ruptured distal stumps to adjacent intact tendons (e.g., EDM to ring finger EDC) or formal tendon transfers (e.g., EIP to EPL) are executed.
Psoriatic Arthritis: Proximal Interphalangeal (PIP) Joint Arthrodesis
Given the destructive nature of PsA, PIP arthrodesis is the procedure of choice for severe contractures or instability.
1. Approach: A dorsal longitudinal, curvilinear, or V-shaped incision is made over the affected PIP joint.
2. Exposure: The extensor mechanism is split longitudinally in the midline (splitting the central slip). The collateral ligaments are sharply excised from their phalangeal origins, allowing the joint to be "shotgunned" (hyperflexed) for maximal exposure.
3. Joint Preparation: The sclerotic articular surfaces and any remaining cartilage of the proximal and middle phalanges are resected using a microsaw or a sharp rongeur. The goal is to create flat, healthy, bleeding cancellous bone surfaces.
4. Positioning: The angle of fusion is meticulously tailored to the specific digit to optimize the functional cascade of the hand. The index finger is typically fused at 20° to 25° of flexion to facilitate fine pinch, while the angle progressively increases ulnarly, with the small finger fused at 40° to 50° to optimize power grip.
5. Fixation: Rigid osteosynthesis is achieved. While crossed Kirschner wires (0.045 inch) are traditional and cost-effective, modern techniques frequently utilize a dorsal tension band wire construct or a dedicated headless intramedullary compression screw, which provides superior biomechanical compression and higher union rates.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, reconstructive procedures for arthritic hand disorders carry a distinct profile of potential complications. The incidence and severity of these complications are heavily influenced by the underlying pathology, bone quality, and patient compliance with postoperative rehabilitation.
In trapeziometacarpal arthroplasty (LRTI), the most common radiographic complication is proximal subsidence of the first metacarpal. While mild subsidence (up to 25% of the trapeziectomy space) is common and often asymptomatic, severe subsidence can lead to impingement against the scaphoid or index metacarpal base, resulting in recurrent pain. Sensory nerve neuropraxia (superficial radial nerve) occurs in approximately 5-10% of cases but typically resolves spontaneously within 3 to 6 months.
In rheumatoid reconstructions, particularly silicone MCP arthroplasty, implant fracture and silicone synovitis are long-term concerns. The incidence of implant fracture increases with time, approaching 30% at 10 years; however, many fractured implants remain clinically functional as they have already facilitated the formation of a stable, aligned fibrous pseudocapsule. Infection in the rheumatoid patient is a catastrophic complication, exacerbated by systemic immunosuppression (DMARDs/biologics) and poor soft-tissue envelopes.
Psoriatic arthritis presents the highest risk of postoperative surgical site infections, particularly when operating through or adjacent to active psoriatic plaques. The altered skin flora and compromised barrier function necessitate aggressive perioperative antibiotic prophylaxis and meticulous soft-tissue handling. Nonunion following PIP or DIP arthrodesis occurs in approximately 5-8% of cases, often necessitating revision bone grafting and enhanced internal fixation.
Complications and Salvage Management Table
| Procedure / Pathology | Primary Complications | Estimated Incidence | Salvage / Management Strategy |
|---|---|---|---|
| LRTI (for CMC OA) | Metacarpal subsidence; Superficial radial neuropraxia; CRPS. | Subsidence (15-30%); Neuropraxia (5-10%); CRPS (1-3%). | Revision with rigid suspensionplasty (e.g., Mini TightRope); Neuroma excision; Aggressive hand therapy and sympathetic blocks for CRPS. |
| MCP Arthroplasty (RA) | Silicone implant fracture; Recurrent ulnar drift; Deep infection. | Fracture (20-30% at 10 yrs); Drift (10-15%); Infection (1-2%). | Revision silicone arthroplasty; Soft-tissue rebalancing; Implant removal, aggressive debridement, and conversion to resection arthroplasty or fusion. |
| Darrach Procedure (RA) | Ulnar stump instability (radioulnar impingement); Extensor tendon adhesions. | Stump instability (10-20%); Adhesions (15%). | Revision with soft-tissue stabilization (e.g., ECU tenodesis) or conversion to Sauvé-Kapandji; Tenolysis. |
| PIP Arthrodesis (PsA) | Nonunion/Pseudarthrosis; Deep infection; Malunion. | Nonunion (5-8%); Infection (3-5%); Malunion (2-4%). | Revision osteosynthesis with autologous bone graft (iliac crest or distal radius); Hardware removal and IV antibiotics; Corrective osteotomy. |
Phased Post-Operative Rehabilitation Protocols
The success of reconstructive hand surgery is inextricably linked to a meticulously designed, phased postoperative rehabilitation protocol, guided by a certified hand therapist (CHT). The protocols must be tailored to the specific procedure performed and the underlying tissue quality of the patient.
Phase 1: Maximum Protection (Weeks 0 to 4)
Immediately postoperatively, the primary goals are the protection of surgical repairs, mitigation of edema, and pain control. For an LRTI, the thumb is immobilized in a rigid, well-molded thumb spica cast or custom thermoplastic splint, encompassing the forearm and extending to the IP joint, positioning the thumb in palmar abduction and opposition. For rheumatoid MCP arthroplasties, a dynamic extension splint is fabricated within the first week to maintain MCP extension and radial alignment while allowing active flexion. Edema is aggressively managed with strict limb elevation, retrograde massage of exposed digits, and compressive stockinettes. Active range of motion (AROM) of all uninvolved joints (shoulder, elbow, and non-immobilized digits) is initiated immediately to prevent proximal stiffness.
Phase 2: Controlled Mobilization (Weeks 4 to 8)
At the 4-week mark, rigid immobilization is typically transitioned to a removable orthosis. For the LRTI patient, the cast is removed, and a custom short opponens splint is provided for wear between exercise sessions and at night. Gentle AROM of the CMC and MCP joints is initiated. Passive range of motion (PROM) and forceful stretching are strictly contraindicated to protect the healing ligament reconstruction. In the rheumatoid and psoriatic populations, mobilization must be carefully titrated against the inflammatory response; if joints become erythematous, warm, or excessively painful, the therapy intensity is immediately downgraded. Scar management techniques, including silicone gel sheeting and friction massage, are instituted to prevent tethering of the extensor mechanisms.
Phase 3: Strengthening and Functional Restoration (Weeks 8 to 12+)
By week 8, soft tissue healing is generally sufficient to tolerate progressive loading. Splint wear is gradually weaned to nighttime use only, or during heavy activities. Isometric strengthening is initiated, followed by isotonic exercises utilizing therapeutic putty, hand grippers, and graduated weights. For the LRTI patient, specific focus is placed on strengthening the first dorsal interosseous and the abductor pollicis brevis to dynamically stabilize the CMC joint. Return to unrestricted heavy manual labor or high-impact sports is typically delayed until 4 to 6 months postoperatively. In the rheumatoid and psoriatic populations, the goal is functional optimization rather than maximal strength, educating the patient on joint protection techniques and ergonomic adaptations to preserve the longevity of their reconstructions.
Summary of Landmark Literature and Clinical Guidelines
The contemporary surgical management of arthritic hand disorders is built upon a foundation of rigorous clinical research and landmark anatomical studies. An intimate familiarity with this literature is essential for the academic orthopedic surgeon.
Eaton and Littler (1969): This seminal paper established the radiographic staging system for trapeziometacarpal osteoarthritis that remains the global standard. Their classification (Stages I-IV) accurately correlates the degree of capsular laxity, articular wear, and pan-trapezial extension with specific surgical indications, forming the basis for modern algorithmic treatment.
Burton and Pellegrini (1986): This landmark study popularized the Ligament Reconstruction and Tendon Interposition (LRTI) utilizing the flexor carpi radialis. They provided the definitive biomechanical rationale for reconstructing the volar beak ligament to prevent metacarpal subsidence, demonstrating superior long-term outcomes compared to simple trapeziectomy in high-demand patients.
Swanson (1972): Alfred Swanson revolutionized the treatment of the rheumatoid hand with the introduction of the flexible silicone intramedullary hinge implant. His extensive clinical series demonstrated that the silicone implant acts not as a true joint replacement, but as a dynamic spacer that maintains alignment while the body forms a functional, encapsulating fibrous pseudocapsule. This concept remains the bedrock of modern MCP joint arthroplasty in inflammatory arthropathies.
Nalebuff (1968): Nalebuff's precise anatomical classification of rheumatoid thumb deformities (
