AAOS Shoulder MCQs (Set 4): Rotator Cuff, Instability & Fractures | Board Review

Key Takeaway
This high-yield question set for the AAOS/ABOS exams covers essential shoulder topics. Focus on diagnosing and managing rotator cuff tears, understanding various forms of shoulder instability, and recognizing common shoulder fractures. Ideal for residents preparing for OITE and board certification.
AAOS Shoulder MCQs (Set 4): Rotator Cuff, Instability & Fractures | Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 50-year-old electrician who is right-hand dominant has had right shoulder pain and stiffness after sustaining an electric shock 2 months ago. An AP radiograph obtained at the time of injury was considered negative, and the patient was diagnosed with a shoulder sprain. The patient now reports continued shoulder pain and restricted motion. AP and axillary radiographs and a CT scan are shown in Figures 41a through 41c. Management should consist of
Explanation
Question 2
Figure 42 shows the radiograph of a 70-year-old woman who has had a painful near ankylosis of her dominant elbow for 1 year. Treatment should consist of
Explanation
Question 3
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of
Explanation
Question 4
A 25-year-old man underwent a Putti-Platt repair for recurrent anterior dislocation of his right shoulder 9 months ago. He reports no further episodes of instability but continues to have severely restricted motion, with external rotation limited to less than 0 degrees with the arm at the side. He has pain at the ends of range of motion and restricted activities of daily living despite undergoing nearly 9 months of physical therapy. Radiographs of the shoulder show no arthritic changes. Management should now consist of
Explanation
Question 5
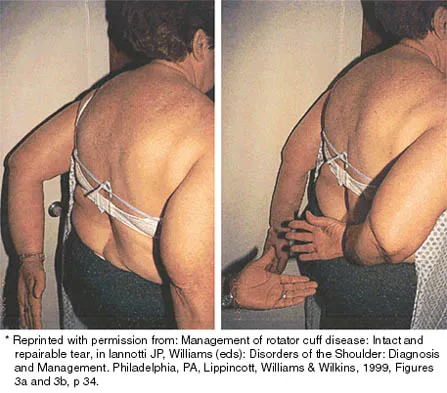
A 43-year-old bus driver sustains a hyperextension injury to her arm and shoulder 4 months after undergoing an open Bankart repair. Examination reveals increased external rotation, anterior shoulder pain, and internal rotation weakness. Her examination also reveals the findings shown in Figure 44. What is the most likely diagnosis?
Explanation
Question 6
Radial nerve palsy is most commonly associated with which of the following types of humeral fractures?
Explanation
Question 7
A 30-year-old firefighter sustained a longitudinal pulling injury to the arm while attempting to move a heavy object during a fire. Figure 45 shows an MRI scan of the elbow. Initial management should consist of
Explanation
Question 8
Which of the following is considered a reasonable goal for arthroplasty surgery in rotator cuff arthropathy?
Explanation
Question 9
What is the best surgical approach for the scapular fracture shown in Figure 46?
Explanation
Question 10
Management of a grade IV osteochondritis dissecans lesion of the capitellum should consist of
Explanation
Question 11
What preoperative factor correlates best with the outcome of rotator cuff repair?
Explanation
Question 12
A 55-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing left shoulder pain for the past 2 years despite nonsurgical management. No focal weakness is noted during examination of the shoulder. AP and axillary radiographs are shown in Figures 47a and 47b. Treatment should consist of
Explanation
Question 13
When elevating the arm, the ratio of scapulothoracic to glenohumeral motion over the total range of motion is best described as
Explanation
Question 14
Figure 48 shows the initial AP chest radiograph of a 21-year-old motorcycle rider who sustained multiple injuries after striking a telephone pole at high speed. What is the most significant radiographic finding leading to a diagnosis?
Explanation
Question 15
A 21-year-old man who underwent repair of a distal biceps tendon rupture using a two-incision approach 4 months ago now reports difficulty gaining rotation of his forearm. Figures 49a and 49b show the AP and lateral radiographs. What is the most likely cause of his problem?
Explanation
Question 16
A 53-year-old man reports acute, severe left shoulder pain after undergoing abdominal surgery 10 days ago. Initial management, consisting of anti-inflammatory drugs, physical therapy, and a subacromial injection of corticosteroid, fails to provide relief. Reexamination of the shoulder 2 months after the onset of symptoms reveals atrophy of the infraspinous and supraspinous fossa and profound weakness of active abduction and external rotation. His neck is supple with a full range of motion. Plain radiographs and an MRI scan of the shoulder are normal. What diagnostic study should be performed next in the evaluation of this patient?
Explanation
Question 17
A 58-year-old reports pain and stiffness in his left shoulder following a seizure episode. Diagnosis at the time of the seizure is a frozen shoulder, and management consists of an aggressive physical therapy program of stretching exercises. Four months later he continues to have shoulder pain and has not gained any additional range of motion. A CT scan is shown in Figure 50. Management should now consist of
Explanation
Question 18
When conducted at near physiologic strain rates, tensile studies of the inferior glenohumeral ligament (IGHL) have shown that the
Explanation
Question 19
Manipulation under anesthesia for resistant frozen shoulder should be avoided in patients with
Explanation
Question 20
A patient who sustained a cerebrovascular accident (CVA) 18 months ago has a long-standing spastic adduction contracture of the shoulder with a rigid block to passive external rotation. Significant hygiene problems exist with maceration and continued skin breakdown. Management should consist of
Explanation
Question 21
A patient with degenerative osteoarthritis of the sternoclavicular (SC) joint reports constant pain, discomfort, and marked prominence and instability of the SC joint following medial clavicle resection. Which of the following procedures is most likely to produce these signs and symptoms?
Explanation
Question 22
A 26-year-old man has had a 2-year history of pain and stiffness after sustaining a comminuted olecranon fracture. Treatment at the time of injury consisted of open reduction and internal fixation with tension band wiring. Examination reveals motion of 45 degrees to 110 degrees and pain throughout the arc of motion. Resisted flexion and extension are painful. Forearm rotation is normal. Radiographs are shown in Figure 51. Treatment should consist of
Explanation
Question 23
What is the most common cause of rotator cuff injury in high school athletes?
Explanation
Question 24
A 16-year-old boy with osteochondritis dissecans of the capitellum has intermittent symptoms of catching and locking. Examination is unremarkable. Radiographs reveal a loose body anteriorly with a diameter of 10 mm. To remove the loose body, elbow arthroscopy is being considered. Which of the following procedures would minimize the risk of neurovascular complication during the procedure?
Explanation
Question 25
Examination of the shoulder seen in Figure 52 shows atrophy and tenderness of the infraspinous fossa and profound weakness in external rotation. The supraspinous fossa shows normal muscle bulk. What is the most likely cause of this condition?
Explanation
Question 26
A 24-year-old collegiate rugby player presents with recurrent anterior shoulder instability. A CT scan reveals 26% anterior glenoid bone loss.
What is the most appropriate definitive management?

Explanation
Question 27
A 45-year-old man presents with severe shoulder pain and restricted external rotation following a grand mal seizure. Radiographs confirm a locked posterior shoulder dislocation with a reverse Hill-Sachs lesion involving 35% of the articular surface. Which of the following is the most appropriate surgical treatment?
Explanation
Question 28
A 32-year-old competitive volleyball player reports vague posterior shoulder pain and weakness with external rotation. Examination shows isolated atrophy of the infraspinatus. MRI reveals a multiloculated cystic structure at the spinoglenoid notch.
What associated intra-articular pathology is most likely present?

Explanation
Question 29
A 75-year-old man presents with chronic right shoulder pain and an inability to actively elevate his arm above 40 degrees. Passive range of motion is full. Radiographs reveal superior migration of the humeral head with an acromiohumeral interval of 3 mm. MRI confirms a massive, retracted tear of the supraspinatus and infraspinatus with Goutallier stage 4 fatty infiltration. His deltoid is functional. What is the most appropriate definitive management?
Explanation
Question 30
A 22-year-old collegiate linebacker presents with recurrent anterior shoulder instability. He has had 5 dislocations over the past two seasons. A 3D CT scan reveals 25% anterior glenoid bone loss. What is the most appropriate surgical management?
Explanation
Question 31
A 45-year-old man presents to the emergency department with severe left shoulder pain following a generalized tonic-clonic seizure. On examination, his arm is locked in internal rotation, and he has 0 degrees of external rotation. Radiographs demonstrate a 'lightbulb' sign on the AP view. A CT scan reveals an anteromedial humeral head impaction fracture involving 30% of the articular surface. Which of the following is the most appropriate surgical treatment?
Explanation
Question 32
A 68-year-old woman falls onto her outstretched arm and sustains a displaced 4-part proximal humerus fracture. She has a history of severe osteoporosis. Her tuberosities are widely displaced, and the anatomic neck is fractured. Which of the following factors is most predictive of humeral head avascular necrosis in this patient?
Explanation
Question 33
A 55-year-old man presents with anterior shoulder pain and weakness following a fall while water skiing. On physical examination, he has full passive range of motion. When the patient places the palm of his hand on his opposite shoulder, he is unable to resist the examiner pulling the hand away anteriorly. Which tendon is most likely injured?
Explanation
Question 34
A 32-year-old elite volleyball player complains of vague posterior shoulder pain and weakness with external rotation. Examination shows isolated atrophy of the infraspinatus fossa with normal supraspinatus bulk. Which of the following is the most likely etiology?
Explanation
Question 35
A 24-year-old rock climber undergoes diagnostic arthroscopy for recurrent anterior shoulder instability. The surgeon identifies a deep, engaging posterolateral humeral head defect. To prevent this lesion from engaging the anterior glenoid rim during abduction and external rotation, the surgeon performs a Remplissage. Which structure is tenodesed into the humeral defect?
Explanation
Question 36
A 40-year-old man presents with right shoulder weakness 3 weeks after a motor vehicle collision. He complains of pain at the base of his neck and shoulder. On physical examination, forward flexion of the arm against resistance results in medial translation and prominent winging of the scapula. Injury to which of the following nerves is the most likely cause?
Explanation
Question 37
A 65-year-old man sustains a traumatic anterior shoulder dislocation. After closed reduction in the emergency department, he presents 2 weeks later complaining of inability to raise his arm. He has no numbness or tingling. Radiographs are normal. Physical examination reveals active forward elevation to 45 degrees and a positive drop arm test. What is the most appropriate next step in management?
Explanation
Question 38
A 28-year-old man falls onto his lateral shoulder and sustains a closed midshaft clavicle fracture. Which of the following is considered an indication for operative fixation to prevent nonunion and symptomatic malunion?
Explanation
Question 39
A 35-year-old male bodybuilder feels a sudden pop in his anterior axilla while performing a heavy bench press. He presents with ecchymosis, swelling, and a loss of the anterior axillary fold. MRI confirms a complete rupture of the pectoralis major tendon. Where does this rupture most commonly occur?
Explanation
Question 40
A 45-year-old recreational tennis player has persistent shoulder pain despite 6 months of conservative management. An MRI arthrogram reveals an articular-sided partial-thickness supraspinatus tendon tear measuring 7 mm in depth (approximately 60% of the tendon thickness). What is the recommended surgical management?
Explanation
Question 41
A 45-year-old manual laborer presents with chronic shoulder weakness. MRI demonstrates a massive, retracted supraspinatus and infraspinatus tear with Goutallier grade 4 fatty infiltration. The subscapularis and teres minor are intact, and there is no glenohumeral arthritis. Which of the following is the most appropriate surgical option?
Explanation
Question 42
A 22-year-old rugby player has recurrent anterior shoulder instability. CT scan indicates 28% anterior glenoid bone loss.
What is the most appropriate management?
Explanation
Question 43
A 65-year-old female undergoes open reduction and internal fixation of a 3-part proximal humerus fracture. Six weeks postoperatively, radiographs show varus collapse of the humeral head and superior screw cutout. Which of the following intraoperative factors most likely contributed to this complication?
Explanation
Question 44
A 74-year-old man presents with pseudoparalysis of the right shoulder and severe glenohumeral osteoarthritis.
Which of the following biomechanical changes is achieved by the most appropriate surgical treatment for this condition?

Explanation
Question 45
A 35-year-old man presents with a locked posterior shoulder dislocation after a seizure. CT scan confirms a reverse Hill-Sachs lesion involving 25% of the anterior articular surface. What is the most appropriate surgical treatment?
Explanation
Question 46
A 42-year-old recreational tennis player has persistent anterior shoulder pain. MRI shows a Type II SLAP tear. After 6 months of failed physical therapy, surgery is planned. Compared to SLAP repair, primary biceps tenodesis in this demographic is associated with:
Explanation
Question 47
A 28-year-old woman presents with isolated lateral scapular winging that worsens when she abducts her arm against resistance. She had a cervical lymph node biopsy 3 months ago. What is the most appropriate initial management?
Explanation
Question 48
A 62-year-old male presents with weakness in internal rotation. On physical exam, he is instructed to place his hand on his contralateral shoulder and resist the examiner's attempt to pull the hand away. Which specific structure is being isolated and tested?
Explanation
Question 49
A 30-year-old male cyclist falls directly on his shoulder. Radiographs reveal a Type V acromioclavicular (AC) joint injury. Which of the following accurately describes the pathologic anatomy of this injury pattern?
Explanation
Question 50
Which of the following is the most significant combination of risk factors for nonunion in a midshaft clavicle fracture treated nonoperatively?
Explanation
Question 51
During an arthroscopic rotator cuff repair, the surgeon evaluates the long head of the biceps tendon for instability. Which of the following structures forms the primary medial restraint to medial subluxation of the biceps tendon within the bicipital groove?
Explanation
Question 52
A 45-year-old man presents with anterior shoulder pain and weakness after a fall with his arm externally rotated. He has a positive bear-hug test and increased passive external rotation compared to the contralateral side. What is the most likely diagnosis?
Explanation
Question 53
A 22-year-old rugby player has recurrent anterior shoulder instability. A CT scan reveals 26% anterior glenoid bone loss. Which of the following is the most appropriate surgical intervention?
Explanation
Question 54
A 35-year-old man presents to the ER after a generalized seizure. His arm is locked in internal rotation. Radiographs show a "lightbulb" sign on the AP view. What is the most common associated bony defect?
Explanation
Question 55
A 72-year-old man presents with pseudoparalysis of the shoulder and chronic massive, irreparable tears of the supraspinatus and infraspinatus. His teres minor and subscapularis are intact. Radiographs show severe glenohumeral osteoarthritis with superior migration of the humeral head. What is the treatment of choice?
Explanation
Question 56
According to the Neer classification for proximal humerus fractures, what defines a "part" as being displaced?
Explanation
Question 57
A 28-year-old tennis player complains of shoulder weakness. On examination, there is lateral winging of the scapula, especially with attempted shoulder abduction. Which nerve is most likely injured?
Explanation
Question 58
During an arthroscopic evaluation of a 25-year-old with recurrent anterior shoulder instability, the surgeon notes avulsion of the inferior glenohumeral ligament from the anatomic neck of the humerus.
What is this lesion called?
Explanation
Question 59
A 32-year-old volleyball player presents with insidious onset of posterior shoulder pain and profound isolated weakness in external rotation. Atrophy is noted in the infraspinatus fossa, while the supraspinatus fossa is normal. Where is the most likely site of nerve entrapment?
Explanation
Question 60
A 65-year-old woman undergoes open reduction and internal fixation (ORIF) with a locked plate for a 3-part proximal humerus fracture. One year postoperatively, she complains of severe, grinding shoulder pain. Radiographs demonstrate intra-articular screw penetration. What was the most likely intraoperative technical error?
Explanation
Question 61
A 21-year-old cyclist falls directly onto his shoulder. Radiographs show a midshaft clavicle fracture. Which of the following is considered an absolute indication for operative fixation?
Explanation
Question 62
The rotator interval is a triangular space in the anterosuperior shoulder. Which of the following structures is anatomically located within the rotator interval?
Explanation
Question 63
A 26-year-old patient with recurrent anterior shoulder dislocations is found to have an "engaging" Hill-Sachs lesion during diagnostic arthroscopy. Which of the following procedures is most appropriate to combine with an arthroscopic Bankart repair?
Explanation
Question 64
A 22-year-old elite baseball pitcher presents with posterior shoulder pain during the late cocking phase of throwing. He has a positive Jobe relocation test and glenohumeral internal rotation deficit (GIRD).
What is the primary pathophysiologic mechanism?
Explanation
Question 65
A 30-year-old bodybuilder feels a sudden pop and pain in his anterior shoulder while performing a heavy bench press. Examination shows loss of the anterior axillary fold and weakness in internal rotation. MRI confirms a rupture of the pectoralis major at its humeral insertion. What is the recommended treatment?
Explanation
Question 66
Which type of Superior Labrum Anterior to Posterior (SLAP) tear is characterized by a bucket-handle tear of the superior labrum with the biceps anchor remaining solidly attached to the glenoid?
Explanation
Question 67
A 75-year-old female presents with chronic right shoulder pain, inability to actively elevate her arm past 40 degrees, and normal passive range of motion. Radiographs demonstrate severe glenohumeral osteoarthritis with superior migration of the humeral head articulating with the acromion. Which of the following is the most appropriate definitive surgical management?
Explanation
Question 68
A 20-year-old male collegiate rugby player presents with recurrent anterior shoulder instability. A 3D CT scan reveals 28% anterior glenoid bone loss. Which of the following procedures provides the most reliable long-term stability for this patient?
Explanation
Question 69
A 68-year-old female sustains a comminuted 4-part proximal humerus fracture after a ground-level fall. She has poor bone quality and severe comminution of the tuberosities.
Which of the following treatments provides the most predictable improvement in forward elevation?

Explanation
Question 70
A 35-year-old male presents to the emergency department with his arm locked in internal rotation following a generalized tonic-clonic seizure. An axillary radiograph confirms a posterior shoulder dislocation with an impaction fracture of the anteromedial humeral head involving 35% of the articular surface. What is the most appropriate surgical treatment?
Explanation
Question 71
A 45-year-old manual laborer presents with a massive, irreparable posterosuperior rotator cuff tear. He has an intact subscapularis, preserved glenohumeral cartilage, and profound weakness in external rotation. Which of the following tendon transfers is most appropriate to restore external rotation?
Explanation
Question 72
Which of the following glenoid morphologies (Walch classification) in the setting of primary osteoarthritis is characterized by a biconcave surface and posterior subluxation of the humeral head, and carries the highest risk of early glenoid component loosening in anatomic total shoulder arthroplasty?
Explanation
Question 73
A 26-year-old male presents with recurrent anterior shoulder instability. An MRI arthrogram reveals an intact anterior labrum but a complete avulsion of the inferior glenohumeral ligament from its humeral attachment, presenting as a 'J-sign'. What is the most likely diagnosis?
Explanation
Question 74
A 28-year-old professional baseball pitcher complains of posterior shoulder pain during the late cocking phase of throwing. Examination reveals a 25-degree Glenohumeral Internal Rotation Deficit (GIRD) compared to the contralateral side. This condition is primarily driven by contracture of which of the following structures?
Explanation
Question 75
A 32-year-old elite volleyball player presents with painless weakness in external rotation of her dominant shoulder. Examination reveals isolated atrophy of the infraspinatus fossa. The supraspinatus exhibits normal strength. Entrapment of the suprascapular nerve at which of the following locations best explains these findings?
Explanation
Question 76
A 30-year-old competitive weightlifter felt a sudden "pop" in his anterior shoulder while performing a heavy bench press. He now has significant ecchymosis on his proximal arm and loss of the anterior axillary fold contour. The vast majority of these injuries occur at which anatomic location?
Explanation
Question 77
A 40-year-old male sustains a distal third clavicle fracture. Radiographs confirm a Neer Type II fracture with superior displacement of the medial fragment.
What is the most appropriate management and primary rationale?

Explanation
Question 78
A 45-year-old female underwent a lymph node biopsy in the posterior triangle of her neck 3 weeks ago. She now complains of a severe ache in her shoulder and difficulty lifting her arm overhead. Physical examination reveals lateral winging of the scapula. Which nerve was most likely injured?
Explanation
Question 79
A 25-year-old male sustains a closed midshaft humerus fracture after a fall. Upon presentation, he has a wrist drop and inability to extend his fingers, but normal sensation in the axillary nerve distribution. Radiographs show acceptable alignment. What is the most appropriate initial management of the nerve injury?
Explanation
Question 80
A 55-year-old male falls forward on his outstretched arm. He presents with shoulder pain, a positive lift-off test, and a positive bear-hug test. Passive external rotation is increased compared to the contralateral side. Which structure is most likely injured?
Explanation
Question 81
A 50-year-old female with poorly controlled type II diabetes presents with an insidious onset of severe diffuse shoulder pain and a profound loss of both active and passive motion, particularly external rotation. Radiographs are normal. What is the most likely diagnosis?
Explanation
Question 82
A 24-year-old male with recurrent anterior shoulder instability undergoes arthroscopy. He is found to have an anterior Bankart lesion and a large Hill-Sachs defect that engages the anterior glenoid rim during abduction and external rotation. Glenoid bone loss is estimated at 10%. Which of the following is the most appropriate surgical treatment?
Explanation
Question 83
A 22-year-old collegiate baseball pitcher is diagnosed with a Type II SLAP tear after failing nonoperative management. What is the primary biomechanical mechanism responsible for this specific labral pathology in overhead throwers?
Explanation
Question 84
A 70-year-old female presents 1 year after an anatomic total shoulder arthroplasty performed for a complex proximal humerus fracture. She is unable to actively elevate her arm above 60 degrees. Radiographs show superior migration of the humeral head and resorption of the greater tuberosity. What is the primary cause of her functional deficit?
Explanation
Question 85
A 22-year-old competitive rugby player presents with recurrent anterior shoulder instability. A 3D computed tomography (CT) scan reveals 26% anterior glenoid bone loss. Which of the following is the most appropriate surgical intervention to minimize the risk of recurrent instability?
Explanation
Question 86
A 45-year-old heavy laborer presents with a massive, irreparable posterosuperior rotator cuff tear. He has intact subscapularis function, active forward elevation to 130 degrees, but a severe lag sign in external rotation. Radiographs show no glenohumeral osteoarthritis. What is the most appropriate surgical management?
Explanation
Question 87
A 78-year-old female with osteoporosis sustains a highly comminuted 4-part proximal humerus fracture with a split humeral head.
What is the most appropriate surgical management to maximize her functional outcome?
Explanation
Question 88
A 30-year-old professional volleyball player complains of vague posterior shoulder pain and isolated weakness in external rotation. An MRI reveals a paralabral cyst at the spinoglenoid notch. This finding is most commonly associated with which of the following concomitant pathologies?
Explanation
Question 89
A 25-year-old male presents with recurrent anterior shoulder dislocations. Imaging demonstrates an off-track engaging Hill-Sachs lesion with 12% anterior glenoid bone loss. Which of the following is the most appropriate arthroscopic surgical management?
Explanation
Question 90
Which of the following clinical scenarios represents an absolute indication for immediate operative fixation of an acute midshaft clavicle fracture?
Explanation
Question 91
A 55-year-old man presents with anterior shoulder pain and weakness with internal rotation. On examination, the examiner elevates the patient's arm to 90 degrees in the scapular plane, flexes the elbow to 90 degrees, and asks the patient to internally rotate against resistance. The patient is unable to maintain the hand against his opposite shoulder. Which structure is most likely injured?
Explanation
Question 92
A 45-year-old manual laborer undergoes shoulder arthroscopy for superior shoulder pain. A Type II SLAP tear is identified with no other intra-articular pathology. Based on current literature, what is the best surgical management for this patient to minimize postoperative stiffness and reoperation?
Explanation
Question 93
A 65-year-old male undergoes open reduction and internal fixation (ORIF) with a locking plate for a 3-part proximal humerus fracture. Six weeks postoperatively, radiographs demonstrate intra-articular screw penetration. What is the most common technical error during the index procedure leading to this complication?
Explanation
Question 94
A 35-year-old male sustains a severe seizure resulting in a locked posterior shoulder dislocation. CT imaging reveals a reverse Hill-Sachs lesion involving 25% of the anteromedial humeral head articular surface. What is the most appropriate management?
Explanation
Question 95
Which of the following preoperative factors has been most strongly correlated with structural failure (non-healing) following arthroscopic repair of a large rotator cuff tear?
Explanation
Question 96
A 40-year-old male sustains a high-energy trauma resulting in a severely displaced scapular fracture. Which of the following parameters is a widely accepted indication for operative fixation of a scapular neck/body fracture?
Explanation
Question 97
During an open Latarjet procedure, aggressive medial retraction of the conjoint tendon places a specific nerve at risk of traction injury. Which nerve is most vulnerable, and what is its expected distance from the tip of the coracoid?
Explanation
Question 98
During an arthroscopic rotator cuff repair, the surgeon identifies the 'comma sign' tissue dropping deep into the joint. Tracing this structure superiorly and laterally leads directly to the torn edge of which anatomical structure?
Explanation
None
