AAOS Shoulder Board Review MCQs (Set 2): Rotator Cuff, Instability & Proximal Humerus Fractures

Key Takeaway
This high-yield question set (Set 2) for the AAOS and ABOS orthopedic exams focuses on critical shoulder pathology. It covers rotator cuff tears, including diagnosis and surgical management, various forms of shoulder instability and associated treatments, and the classification and treatment principles for proximal humerus fractures.
AAOS Shoulder Board Review MCQs (Set 2): Rotator Cuff, Instability & Proximal Humerus Fractures
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
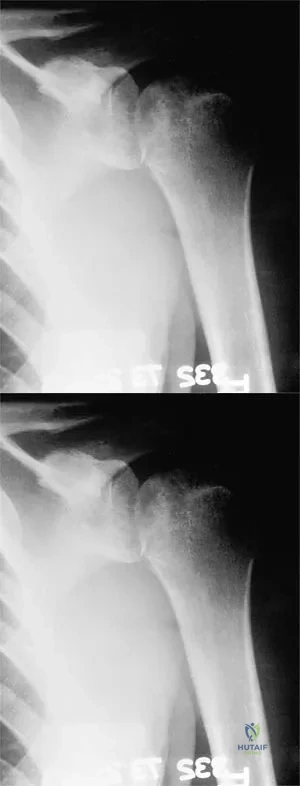
A 37-year-old electrician is diagnosed with a frozen shoulder after sustaining an electrical injury at work 2 weeks ago. Examination reveals that he cannot actively or passively externally rotate or abduct the arm. The glenohumeral joint and scapula move in a 1:1 ratio. Radiographs are shown in Figures 15a and 15b. The best course of action should be
Explanation
Question 2
An 80-year-old man has had increasing shoulder pain for the past 4 months. He reports that it began with soreness and stiffness after chopping some wood. A coronal MRI scan is shown in Figure 16. Initial management should consist of
Explanation
Question 3
Figure 17 shows the radiograph of a 25-year-old professional football player who has superior shoulder pain that prevents him from sports participation. History reveals that he sustained a shoulder injury that was treated with closed reduction and temporary pinning 3 years ago. The best course of action should be
Explanation
Question 4
A 54-year-old man undergoes total shoulder arthroplasty for osteoarthritis. Despite compliance with an early passive range-of-motion exercise program, he does not regain more than 90 degrees of elevation, 10 degrees of external rotation, and has internal rotation to the fifth lumbar vertebra. At 6 months, his motion fails to improve. Radiographs are shown in Figures 18a and 18b. What is the best course of action?
Explanation
Question 5
A 47-year-old patient has had persistent pain and weakness after undergoing a reamed intramedullary nailing for a midshaft humerus fracture 8 months ago. There is no evidence of infection. Radiographs are shown in Figures 19a and 19b. Management should consist of
Explanation
Question 6
An 18-year-old man sustained closed humeral shaft and forearm fractures of his dominant arm in a motor vehicle accident. Neurovascular examination is intact, and his condition is stable. The best course of action for management of the injuries should be
Explanation
Question 7
A 32-year-old woman has had pain and a visibly growing mass in the shoulder for 3 years but denies any history of trauma. Examination reveals a swollen, boggy shoulder mass. The AP radiograph and MRI scan are shown in Figures 20a and 20b. Figures 20c through 20e show a portion of the excised mass and the photomicrographs of the biopsy specimen. What is the most likely diagnosis?
Explanation
Question 8
What is the most important factor regarding the risk of recurrent instability in a patient with an acute anterior dislocation of the shoulder?
Explanation
Question 9
A 25-year-old man injured his dominant shoulder after falling on his outstretched arm 4 months ago. Examination reveals that he cannot lift his arm above 90 degrees, and he has pronounced medial scapular winging. Management should consist of
Explanation
Question 10
Treatment of adhesive capsulitis has a high failure rate when the underlying cause is
Explanation
Question 11
Figure 21 shows the AP radiograph of a 41-year-old patient who sustained a closed bicolumnar fracture of the distal humerus that resulted in a painful nonunion. What is the best initial construct for rigid stabilization of this fracture pattern?
Explanation
Question 12
Figure 22 shows the radiographs of a 16-year-old boy who injured his elbow in a fall 1 year ago. Although he has no pain, he reports restricted forearm rotation and elbow flexion. What is the most likely diagnosis?
Explanation
Question 13
A 55-year-old man has had progressive right shoulder pain for the past 2 years. Examination reveals active elevation to 120 degrees, external rotation to 20 degrees, and internal rotation to the sacrum. AP and axillary radiographs are shown in Figures 23a and 23b. Which of the following procedures would result in the most predictable long-term pain relief?
Explanation
Question 14
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?
Explanation
Question 15
A right-handed 24-year-old woman underwent an arthroscopic Bankart repair for recurrent anterior dislocations 9 months ago. Despite extensive physical therapy for 8 months, the patient has very limited range of motion (elevation to 130 degrees and external rotation to 10 degrees with the arm at the side). Shoulder radiographs are normal. The next step in management should consist of
Explanation
Question 16
A patient with deficient anteroinferior bone stock undergoes a Latarjet procedure that transfers a portion of the coracoid to the glenoid rim and secures it with two screws. After surgery, the patient reports numbness on the anterolateral forearm. To verify the diagnosis, what muscle should be tested for strength?
Explanation
Question 17
A 34-year-old woman has had painful snapping and popping in the elbow since falling while in-line skating 6 months ago. The popping also occurs when she pushes off with her hands to rise from a seated position. Initial radiographs were normal, and she was told that she had sprained her elbow. Examination reveals few findings except that she is very apprehensive when the forearm is forcefully supinated with the elbow extended or partially flexed. A radiograph taken in that position is shown in Figure 24. Treatment should consist of
Explanation
Question 18
A 49-year-old woman noted pain in her right axilla 1 day after moving heavy furniture. Two weeks later, she now reports persistent numbness and paresthesias along the inner aspect of her upper arm radiating into the ulnar digits. Examination reveals full shoulder motion, tenderness over the first rib, and a decreased radial pulse with the shoulder placed overhead. What is the most likely diagnosis?
Explanation
Question 19
A patient has had a locked posterior dislocation of the shoulder for the past 6 months. After undergoing total shoulder arthroplasty that includes adequate anterior releases and posterior capsulorrhaphy, the patient still exhibits posterior instability intraoperatively. The postoperative rehabilitation regimen should include
Explanation
Question 20
Which of the following factors is associated with failure of arthroscopic excision of the distal clavicle?
Explanation
Question 21
Anterior subluxation in a throwing athlete is most commonly the result of
Explanation
Question 22
What is the most significant prognostic factor in nontraumatic osteonecrosis of the humeral head?
Explanation
Question 23
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?
Explanation
Question 24
Which of the following is considered a contraindication to functional bracing for the treatment of humeral shaft fractures?
Explanation
Question 25
A 20-year-old man with fascioscapulohumeral dystrophy has severe scapular winging of both shoulders. He can no longer abduct above 80 degrees, and it affects his activities of daily living. A clinical photograph is shown in Figure 26. Definitive management should consist of
Explanation
Question 26
A 22-year-old collegiate rugby player presents with his fourth anterior shoulder dislocation. A 3D CT scan reveals 26% anterior glenoid bone loss. What is the most appropriate surgical management?
Explanation
Question 27
A 55-year-old man falls on an outstretched arm and experiences a popping sensation in his right shoulder. On exam, he has increased passive external rotation compared to the contralateral side and weakness on the belly-press test. MRI confirms an isolated, complete tear of the subscapularis tendon. What is the most appropriate initial management?
Explanation
Question 28
A 65-year-old female presents with a 4-part proximal humerus fracture.
According to the Hertel criteria, which radiographic feature is most predictive of humeral head ischemia?
Explanation
Question 29
A 28-year-old man has recurrent anterior shoulder instability. Diagnostic arthroscopy reveals an engaging Hill-Sachs lesion and <10% glenoid bone loss. Which of the following is the most appropriate surgical treatment?
Explanation
Question 30
A 70-year-old woman presents with chronic, severe right shoulder pain and an inability to actively elevate her arm past 60 degrees (pseudoparalysis). Radiographs demonstrate superior migration of the humeral head with an acromiohumeral interval of 2 mm. MRI confirms massive, retracted tears of the supraspinatus and infraspinatus with fatty infiltration. What is the treatment of choice?
Explanation
Question 31
A 35-year-old man presents to the emergency department with shoulder pain after a generalized seizure. His arm is locked in adduction and internal rotation, with essentially no passive external rotation possible. An AP radiograph shows a 'lightbulb' sign. Which imaging view is most critical to confirm the diagnosis?
Explanation
Question 32
A 30-year-old elite volleyball player presents with painless weakness in external rotation of the dominant shoulder. Physical exam reveals isolated atrophy of the infraspinatus fossa. MRI shows a paralabral cyst in the spinoglenoid notch. What is the most likely associated intra-articular pathology?
Explanation
Question 33
The biomechanical 'suspension bridge' concept of the rotator cuff relies on force couples to maintain the humeral head centered on the glenoid. Which two muscles form the primary force couple in the transverse plane?
Explanation
Question 34
A 75-year-old woman sustains a minimally displaced 2-part surgical neck fracture of the proximal humerus. She is treated nonoperatively in a sling. To optimize functional outcomes and prevent adhesive capsulitis, when should gentle pendulum exercises and passive range of motion begin?
Explanation
Question 35
An 18-year-old female gymnast complains of bilateral shoulder pain and a sensation of 'slipping'. On exam, she has a positive sulcus sign and apprehension in multiple positions. Beighton score is 6/9. What is the most appropriate initial management?
Explanation
Question 36
A 24-year-old throwing athlete is diagnosed with a Type II SLAP tear via MRI arthrogram. Diagnostic arthroscopy confirms a 'peel-back' lesion of the superior labrum. When placing suture anchors for repair, where is the optimal location to restore biomechanics and prevent internal impingement?
Explanation
Question 37
A 31-year-old man suffers a traumatic anterior shoulder dislocation. MRI reveals a 'J-sign' involving the inferior glenohumeral ligament (IGHL) complex. This indicates a Humeral Avulsion of the Glenohumeral Ligament (HAGL) lesion. Which of the following is true regarding this condition?
Explanation
Question 38
During open reduction and internal fixation of a proximal humerus fracture, a deltopectoral approach is utilized. Which two nerves supply the muscles that form the internervous plane for this approach?
Explanation
Question 39
A patient presents with anterior shoulder pain exacerbated by internal rotation and forward elevation. MRI demonstrates a narrowed coracohumeral interval (<6 mm). Subcoracoid impingement syndrome is suspected. This condition is most strongly associated with pathology of which structure?
Explanation
Question 40
The Latarjet procedure provides stability through a 'triple effect'. Which structure provides the dynamic 'sling effect' when the arm is abducted and externally rotated?
Explanation
Question 41
A 45-year-old heavy laborer has a massive, retracted, and irreparable subscapularis tendon tear. He complains of severe weakness with lifting objects in front of his body. Which tendon transfer is the most appropriate primary option to restore function?
Explanation
Question 42
A 55-year-old physically active man presents with an irreparable posterosuperior rotator cuff tear (supraspinatus and infraspinatus). The subscapularis is completely intact, and there is no glenohumeral arthritis. He has a severe external rotation lag. Which tendon transfer is most appropriate?
Explanation
Question 43
A 72-year-old female undergoes open reduction and internal fixation with a locking plate for a displaced 3-part proximal humerus fracture. Osteoporotic bone is noted during surgery. What is the most common hardware-related complication postoperatively?
Explanation
Question 44
The 'terrible triad' of the shoulder is a distinct clinical entity commonly seen in middle-aged or older patients following high-energy trauma. Which three injuries comprise this triad?
Explanation
Question 45
A 32-year-old man sustains a displaced 3-part proximal humerus fracture after a high-speed motorcycle accident. An axillary nerve injury is suspected. Which clinical finding is the most reliable indicator of axillary nerve dysfunction?
Explanation
Question 46
A 21-year-old collegiate rugby player presents with his fourth anterior shoulder dislocation. A 3D CT scan is obtained to evaluate bone stock.
The imaging reveals 25% anterior glenoid bone loss. What is the most appropriate definitive surgical management?
Explanation
Question 47
A 65-year-old female sustains a proximal humerus fracture after a mechanical fall. According to Hertel's criteria, which of the following radiographic findings is the most reliable predictor of humeral head ischemia?
Explanation
Question 48
A 72-year-old male presents with long-standing shoulder pain and an inability to actively elevate his arm above 45 degrees. Radiographs demonstrate an acromiohumeral distance of 3 mm.
MRI reveals massive, retracted supraspinatus and infraspinatus tears with grade 4 fatty infiltration. What is the most appropriate surgical treatment?

Explanation
Question 49
A 28-year-old offensive lineman presents with deep posterior shoulder pain and clicking during bench pressing. Examination reveals a positive jerk test. If an MRI arthrogram is obtained, it is most likely to show a labral tear at which clock-face location on the right glenoid?
Explanation
Question 50
A 45-year-old male presents with acute shoulder pain and weakness after falling on an outstretched arm while skiing. Physical examination demonstrates increased passive external rotation compared to the contralateral side and a positive belly-press test. Which of the following structures is most likely injured?
Explanation
Question 51
A 24-year-old male is undergoing arthroscopic evaluation for recurrent anterior shoulder instability. Diagnostic arthroscopy reveals an 'engaging' Hill-Sachs lesion, but pre-operative CT scan showed minimal glenoid bone loss (<10%). Which of the following is the most appropriate management strategy?
Explanation
Question 52
When performing a reverse total shoulder arthroplasty for a 4-part proximal humerus fracture in an elderly patient, anatomic healing of the greater tuberosity to the proximal humerus shaft is most critical for restoring which of the following active motions?
Explanation
Question 53
A 62-year-old woman undergoes open reduction and internal fixation with a locked plate for a 3-part proximal humerus fracture.
Which of the following is the most common complication associated with this specific procedure?

Explanation
Question 54
A 19-year-old gymnast presents with bilateral shoulder pain and a sensation of her shoulders 'slipping' during routines. She has a positive sulcus sign bilaterally and generalized ligamentous laxity. Supervised physical therapy has failed to improve her symptoms after 6 weeks. What is the next best step in management?
Explanation
Question 55
During an arthroscopic rotator cuff repair, the surgeon evaluates the normal anatomical footprint on the greater tuberosity. Which of the following best describes the normal insertion site of the supraspinatus tendon?
Explanation
Question 56
A 22-year-old rugby player has recurrent anterior shoulder instability. CT scan with 3D reconstruction demonstrates 25% anterior glenoid bone loss. What is the most appropriate definitive management?
Explanation
Question 57
A 70-year-old man presents with an inability to actively elevate his right arm above 45 degrees, though passive elevation is full. Radiographs show superior migration of the humeral head with an acromiohumeral interval of 3 mm. MRI confirms a massive, retracted rotator cuff tear with Goutallier grade 4 fatty infiltration of the supraspinatus and infraspinatus. What is the best treatment option?
Explanation
Question 58
A 65-year-old woman sustains a 3-part proximal humerus fracture. According to Hertel's criteria, which of the following radiographic findings is most strongly predictive of humeral head ischemia?
Explanation
Question 59
A 34-year-old man has chronic posterior shoulder pain and limited external rotation following a seizure 3 months ago. Radiographs confirm a missed posterior dislocation with an associated reverse Hill-Sachs defect involving 35% of the articular surface. The joint is reducible but unstable in internal rotation. What is the most appropriate management?
Explanation
Question 60
A 45-year-old man presents with anterior shoulder pain and weakness after a forceful external rotation injury. He demonstrates increased passive external rotation compared to the contralateral side. Which physical examination test is most sensitive and specific for his likely injury?
Explanation
Question 61
A 55-year-old woman undergoes locking plate osteosynthesis for a 4-part proximal humerus fracture. Six months later, she presents with severe pain and a mechanical block to motion. Radiographs show fracture healing but the superior-most locking screws are protruding through the articular surface. What intraoperative step is most critical to prevent this complication?
Explanation
Question 62
In the setting of recurrent anterior shoulder instability, the addition of an arthroscopic remplissage (infraspinatus tenodesis) to a Bankart repair is most appropriately indicated for which of the following scenarios?
Explanation
Question 63
A 50-year-old laborer undergoes a latissimus dorsi tendon transfer for an irreparable posterosuperior rotator cuff tear. To function effectively, the transferred latissimus dorsi primarily replicates the function of which native muscle?
Explanation
Question 64
A 72-year-old right-hand-dominant woman sustains a minimally displaced 2-part surgical neck fracture of the proximal humerus. She lives alone and has well-controlled diabetes. What is the most appropriate initial management?
Explanation
Question 65
A 28-year-old volleyball player presents with posterior shoulder pain and weakness in external rotation. MRI reveals a paralabral cyst in the spinoglenoid notch and a superior labral tear. Which physical examination finding is most likely to be present?
Explanation
Question 66
The concept of the "suspension bridge" model of the rotator cuff, described by Burkhart, emphasizes the importance of which intact structures in maintaining normal glenohumeral kinematics despite a supraspinatus tear?
Explanation
Question 67
A 45-year-old man sustains a severe fracture-dislocation of the proximal humerus. During an open reduction through a deltopectoral approach, brisk arterial bleeding is encountered near the inferior border of the subscapularis. Which vessel is most likely injured?
Explanation
Question 68
A 24-year-old swimmer presents with anterior shoulder pain and apprehension. An MR arthrogram demonstrates a "J-sign" with extravasation of contrast inferiorly. What is the most likely diagnosis?
Explanation
Question 69
In performing a superior capsular reconstruction (SCR) for an irreparable supraspinatus tear, the graft is typically attached medially to the superior glenoid and laterally to the greater tuberosity. What is the primary biomechanical goal of this procedure?
Explanation
Question 70
In the treatment of a comminuted 4-part proximal humerus fracture with a reverse total shoulder arthroplasty, anatomic healing of the greater tuberosity is most strongly associated with which functional outcome?
Explanation
Question 71
During a Latarjet procedure, the coracoid process is osteotomized and transferred to the anterior glenoid. Which muscle tendon units are transferred with the coracoid to provide a dynamic "sling" effect?
Explanation
Question 72
A 22-year-old rugby player presents with recurrent anterior shoulder dislocations. Advanced imaging demonstrates 25% glenoid bone loss and an engaging Hill-Sachs lesion. What is the most appropriate definitive surgical management?
Explanation
Question 73
A 65-year-old female sustains a comminuted 4-part proximal humerus fracture. Which of the following radiographic findings is most predictive of avascular necrosis of the humeral head?
Explanation
Question 74
A 55-year-old laborer suffers from chronic shoulder pain and pseudoparalysis of external rotation. MRI reveals a massive, retracted, and fatty-infiltrated tear of the supraspinatus and infraspinatus with an intact subscapularis. Which of the following tendon transfers is most appropriate for restoring active external rotation?
Explanation
Question 75
A 45-year-old male presents with shoulder pain and weakness in internal rotation after a fall. Which of the following physical examination tests is most sensitive and specific for evaluating a tear of the upper border of the subscapularis tendon?
Explanation
Question 76
A 30-year-old weightlifter presents with vague posterior shoulder pain and a positive jerk test. Nonoperative management has failed. Imaging shows a posterior labral tear without significant glenoid bone loss. What is the most appropriate surgical intervention?
Explanation
Question 77
A 24-year-old professional baseball pitcher is diagnosed with an isolated Type II SLAP tear after failing 6 months of physical therapy. What is the recommended surgical management?
Explanation
Question 78
A 78-year-old female undergoes a reverse total shoulder arthroplasty for a severely comminuted 4-part proximal humerus fracture. What is the most critical surgical step for ensuring optimal functional external rotation and joint stability?
Explanation
Question 79
A 22-year-old throwing athlete experiences posterior shoulder pain during the late cocking phase. An MRI arthrogram reveals a partial articular-sided supraspinatus tendon tear and posterosuperior labral fraying. This condition is primarily associated with which of the following pathomechanics?
Explanation
Question 80
A 32-year-old athlete presents with isolated weakness in external rotation of the shoulder. MRI reveals a paralabral cyst causing nerve compression. Where is the cyst most likely located and which muscle will demonstrate isolated atrophy?
Explanation
Question 81
A 72-year-old man presents with progressive pseudoparalysis and severe glenohumeral osteoarthritis secondary to a massive rotator cuff tear. Which of the following is an absolute contraindication to performing a reverse total shoulder arthroplasty in this patient?
Explanation
Question 82
A 60-year-old female undergoes open reduction and internal fixation of a 2-part surgical neck humerus fracture with a locking plate. Postoperatively, radiographs show that the fracture has collapsed into varus. Which of the following technical errors most likely contributed to this complication?
Explanation
Question 83
A 65-year-old male undergoes an arthroscopic biceps tenotomy for a symptomatic superior labral tear and associated biceps tendinopathy. Compared to biceps tenodesis, biceps tenotomy is associated with a significantly higher incidence of which of the following?
Explanation
Question 84
A 19-year-old gymnast presents with bilateral shoulder pain and multidirectional instability. On examination, she has a positive sulcus sign that does not diminish when the arm is placed in external rotation. This finding specifically indicates incompetence of which of the following structures?
Explanation
Question 85
A 28-year-old male bodybuilder feels a pop in his anterior chest while performing a heavy bench press. Examination reveals an asymmetric chest wall contour and weakness in internal rotation. Which of the following describes the most common anatomic location of a pectoralis major rupture in this demographic?
Explanation
Question 86
A 35-year-old skier sustains an acute shoulder dislocation and presents with continued apprehension and instability. An MRI arthrogram reveals extravasation of contrast inferiorly into the axillary pouch, demonstrating a classic "J-sign". What is the most likely diagnosis?
Explanation
Question 87
A 68-year-old female sustains a 4-part proximal humerus fracture. Which of the following radiographic features is the most reliable predictor of humeral head ischemia?
Explanation
Question 88
A 22-year-old rugby player presents with recurrent anterior shoulder instability. CT evaluation demonstrates a 25% anteroinferior glenoid bone loss (an "inverted pear" glenoid). What is the most appropriate surgical management?
Explanation
Question 89
A 72-year-old man presents with chronic shoulder pain and inability to actively elevate his arm above 45 degrees, though passive ROM is full. MRI shows massive, retracted tears of the supraspinatus and infraspinatus with Goutallier grade 4 fatty infiltration. What is the best treatment option?
Explanation
Question 90
During an arthroscopic stabilization for recurrent shoulder instability, an engaging Hill-Sachs lesion is noted with minimal glenoid bone loss. Which of the following procedures is indicated to address the humeral defect?
Explanation
Question 91
A 60-year-old woman undergoes open reduction and internal fixation with a locking plate for a 3-part proximal humerus fracture. What is the most common complication specifically associated with this fixation method?
Explanation
Question 92
A 28-year-old overhead athlete presents with persistent shoulder pain. MRI arthrogram reveals a partial articular-sided supraspinatus tendon avulsion (PASTA) involving 60% of the tendon footprint. Conservative management has failed. What is the recommended surgical approach?
Explanation
Question 93
A 35-year-old man presents with shoulder pain and a locked arm in internal rotation after a first-time seizure. Radiographs reveal a posterior shoulder dislocation with an anteromedial humeral head defect (reverse Hill-Sachs lesion) involving 35% of the articular surface. What is the most appropriate surgical treatment?
Explanation
Question 94
When treating a 4-part proximal humerus fracture in an elderly patient with a reverse total shoulder arthroplasty, which of the following factors is most critical for achieving active external rotation postoperatively?
Explanation
Question 95
A 55-year-old male sustains an acute traumatic anterior shoulder dislocation. After successful reduction, he complains of profound weakness in internal rotation. Which of the following physical examination tests is most sensitive for diagnosing an upper subscapularis tendon tear?
Explanation
Question 96
During an arthroscopy for recurrent anterior shoulder instability, the surgeon identifies an Anterior Labroligamentous Periosteal Sleeve Avulsion (ALPSA) lesion. How does this pathology differ anatomically from a classic Bankart lesion?
Explanation
Question 97
Which of the following best describes the fundamental biomechanical alteration achieved by a classic Grammont-style reverse total shoulder arthroplasty in a patient with advanced rotator cuff arthropathy?
Explanation
Question 98
During an open reduction and internal fixation of a proximal humerus fracture using an extended deltopectoral approach, which nerve is at greatest risk of iatrogenic injury when mobilizing the inferior capsule and placing retractors inferior to the humeral head?
Explanation
Question 99
A 30-year-old professional volleyball player presents with posterior shoulder pain and isolated weakness in external rotation. MRI reveals a paralabral cyst located in the spinoglenoid notch. This finding is most commonly associated with which of the following concomitant labral pathologies?
Explanation
Question 100
A 28-year-old male sustains a shoulder dislocation and subsequent recurrent instability. An MRI arthrogram demonstrates extravasation of contrast into the axillary pouch in a U-shape, replacing the normal V-shaped axillary recess. What is the most likely diagnosis?
Explanation
None
