AAOS Sports Medicine MCQs (Set 2): Knee Ligament & Rotator Cuff Injuries | Board Review
Key Takeaway
This high-yield question set for the AAOS/ABOS Sports Medicine exams (Set 2) covers essential topics including the diagnosis, treatment, and rehabilitation of knee ligament injuries (ACL, PCL, MCL), meniscal tears, and common rotator cuff pathologies. Prepare for your board review.
AAOS Sports Medicine MCQs (Set 2): Knee Ligament & Rotator Cuff Injuries | Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Initial repair of the large U-shaped rotator cuff tear shown in Figure 12 consists of closing the tear side-to-side to take advantage of margin convergence. The most significant biomechanical consequence of this repair step results in
Explanation
Question 2
A 15-year-old athlete collapses suddenly during practice and dies. What is the most likely cause of death?
Explanation
Question 3
A 17-year-old football player continues to have discomfort after sustaining a blow to his midthigh during a game 8 weeks ago. A plain radiograph is shown in Figure 13. What is the most appropriate management?
Explanation
Question 4
When standing, dorsiflexion of the great toe will accentuate
Explanation
Question 5
A 26-year-old professional rodeo bull rider sustained a grade III midshaft femoral fracture after being thrown from his bull. He underwent closed interlocking intermedullary nailing with a titanium rod, and his recovery was uneventful. Prior to returning to competition, the patient must
Explanation
Question 6
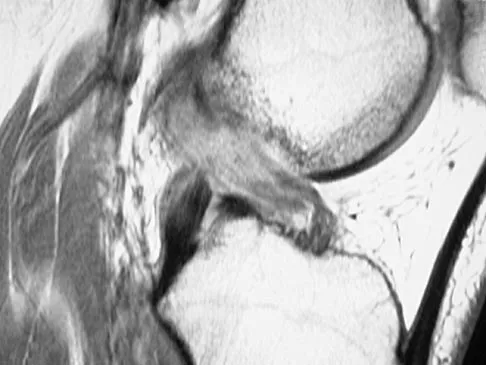
A 19-year-old soccer player feels a pop in his knee while making a cut and notes the development of an effusion over several hours. Examination reveals medial joint line tenderness, but the knee is stable to manual stress testing of all ligaments. Examination under anesthesia confirms a stable knee. What is the most critical factor in determining healing after repair of the lesion shown in Figure 14?
Explanation
Question 7
Which of the following tissues has the highest maximum load to failure?
Explanation
Question 8
A 20-year-old basketball player has tenderness and bruising after sustaining a blow to the knee. A radiograph is shown in Figure 15. What is the most likely diagnosis?
Explanation
Question 9
Reconstruction of the posterior cruciate ligament (PCL) via the inlay technique involves exposure of the PCL tibial insertion site by a posterior
Explanation
Question 10
A 36-year-old recreational tennis player sustains the injury shown in Figure 16. Management should consist of
Explanation
Question 11
Figure 17 shows the clinical photograph of a 45-year-old female tennis player who has right arm pain and weakness with elevation after undergoing a cervical biopsy several months ago. The cause of her shoulder weakness is damage to the
Explanation
Question 12
A collegiate rower reports the sudden onset of right chest pain while rowing. The athlete states that the pain is worse with deep inspiration and coughing. Examination reveals localized tenderness over the posterolateral corner of the eighth rib. What is the most likely diagnosis?
Explanation
Question 13
Figures 18a and 18b show the radiographs of a 13-year-old baseball player who sustained a patellar dislocation with an associated lateral femoral condyle fracture. What ligament is attached to this fragment?
Explanation
Question 14
Which of the following substances does not have androgenic effects?
Explanation
Question 15
A superior labrum anterior and posterior (SLAP) lesion doubles the strain in which of the following stabilizing structures?
Explanation
Question 16
What is the principal advantage of surgical repair for the lesion shown in Figure 19?
Explanation
Question 17
An 18-year-old high school football player sustains a left posterior hip dislocation that is reduced in the emergency department under IV sedation. Postreduction radiographs reveal a concentric reduction with no evidence of fracture or loose bodies within the joint. What is the most common complication of hip dislocations?
Explanation
Question 18
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals lumbar paraspinal spasm and a positive straight leg raising test. Deep tendon reflexes, motor strength, and sensation in the lower extremities are normal. Radiographic findings are normal. If symptoms persist for longer than a few weeks, what is the best course of action?
Explanation
Question 19
Examination of a 23-year-old female college basketball player who has had anterior knee pain for the past 3 weeks reveals tenderness and fullness over the inferior patella and proximal patellar tendon. There is no patellofemoral crepitus, patella apprehension sign, or anterior or posterior instability. Initial management should include
Explanation
Question 20
Which of the following findings is likely to be pathologic in a thin, well-conditioned endurance athlete?
Explanation
Question 21
Figure 20 shows the radiograph of a 21-year-old college basketball player who jammed his left index finger on the rim. He reports pain and tenderness over the dorsum of the distal interphalangeal (DIP) joint. Examination reveals that he is unable to actively extend the DIP joint; however, the skin is intact. Management should consist of
Explanation
Question 22
With a full-thickness articular cartilage injury, the body's healing response produces cartilage mainly composed of what type of collagen?
Explanation
Question 23
A relative contraindication for anteromedial tibial tubercle transfer for patellar instability is arthrosis in what portion of the patella?
Explanation
Question 24
An 18-year-old lacrosse player sustained a hamstring pull during a game. Examination the next day reveals ecchymosis through the posterior thigh and a palpable defect in the hamstring musculature in the middle third of the thigh. What is the most likely site of anatomic injury?
Explanation
Question 25
Figures 21a through 21c show the MRI scans of a 21-year-old football player who sustained a valgus knee injury while changing direction. Examination reveals swelling and tenderness along the medial aspect of the knee. There is a positive Lachman test, 3+ valgus laxity at 30 degrees, and 1+ valgus laxity at 0 degrees extension. The anterior drawer test is increased with the tibia in external rotation. The increase in the anterior drawer test with the tibia in external rotation is most likely the result of
Explanation
Question 26
Which of the following statements regarding the biomechanical properties of commonly used anterior cruciate ligament (ACL) grafts is true?
Explanation
Question 27
During arthroscopic repair of a massive, retracted superior rotator cuff tear, extensive medial mobilization is required. What is the generally accepted "safe zone" distance from the superior glenoid rim to avoid injury to the suprascapular nerve at the suprascapular notch?
Explanation
Question 28
Which bundle of the posterior cruciate ligament (PCL) serves as the primary restraint to posterior tibial translation at 90 degrees of knee flexion?
Explanation
Question 29
A 22-year-old football player sustains a valgus blow to the lateral aspect of his knee. Physical examination reveals medial joint line opening at 30 degrees of flexion but a stable knee in full extension. Which anatomical structure is the primary restraint being tested?
Explanation
Question 30
In a young, active patient with an irreparable posterosuperior rotator cuff tear (supraspinatus and infraspinatus) but an intact subscapularis, which of the following tendon transfers is biomechanically and clinically most appropriate to restore external rotation and elevation?
Explanation
Question 31
A 24-year-old athlete sustains a combined ACL and posterolateral corner (PLC) injury. If the surgeon reconstructs only the ACL and fails to address the PLC, what is the most likely biomechanical consequence?
Explanation
Question 32
Understanding the anatomical "footprint" of the rotator cuff is essential for proper repair. The supraspinatus footprint on the greater tuberosity is best described by which of the following medial-to-lateral dimensions?
Explanation
Question 33
An obese 35-year-old male sustains a low-velocity knee dislocation following a fall. After successful closed reduction, vascular evaluation reveals an Ankle-Brachial Index (ABI) of 0.8. What is the most appropriate next step in management?
Explanation
Question 34
Which of the following patient factors has been clinically demonstrated to have the most significant negative impact on tendon-to-bone healing and functional outcomes following arthroscopic rotator cuff repair?
Explanation
Question 35
A 9-year-old male (Tanner stage 1) sustains a midsubstance ACL rupture while playing soccer. He experiences giving way during daily activities. What is the most widely recommended surgical approach to minimize the risk of growth arrest?
Explanation
Question 36
During clinical examination of a patient with shoulder pain, the examiner places the palm of the patient's hand on the opposite shoulder and attempts to pull the hand anteriorly while the patient resists. This test is highly specific for a tear of which tendon?
Explanation
Question 37
Which of the following functional criteria is widely accepted as a minimum objective requirement before an athlete is cleared to return to cutting sports following an ACL reconstruction?
Explanation
Question 38
A 45-year-old tennis player presents with persistent shoulder pain despite conservative management. MRI reveals a Partial Articular-Sided Supraspinatus Tendon Avulsion (PASTA) lesion that involves roughly 60% of the tendon thickness. What is the most appropriate surgical treatment?
Explanation
Question 39
Biomechanical studies have demonstrated that a medial meniscus posterior root tear alters knee joint kinematics in a manner functionally equivalent to which of the following conditions?
Explanation
Question 40
The anterolateral ligament (ALL) of the knee originates posterior and proximal to the lateral epicondyle and inserts on the proximal tibia midway between Gerdy's tubercle and the fibular head. What is its primary biomechanical role?
Explanation
Question 41
A 28-year-old competitive weightlifter feels a sudden pop and tearing sensation in his anterior chest while bench pressing. Examination reveals ecchymosis and loss of the normal axillary fold contour. If surgical repair is performed, the ruptured tendon should be reattached to which anatomical landmark?
Explanation
Question 42
A patient with knee instability is examined using the dial test. The examiner notes 15 degrees of increased external rotation of the affected limb compared to the normal limb at 30 degrees of knee flexion, but there is no side-to-side difference at 90 degrees of knee flexion. This finding strongly suggests an isolated injury to which structure?
Explanation
Question 43
During a massive rotator cuff repair, the surgeon opts to perform an open subpectoral biceps tenodesis. If retractor placement and dissection drift too far medial to the short head of the biceps/coracobrachialis, which nerve is at greatest risk of iatrogenic injury?
Explanation
Question 44
Which component of the posterolateral corner (PLC) of the knee is the primary restraint to external rotation of the tibia at 30 degrees of knee flexion?
Explanation
Question 45
A 32-year-old elite volleyball player presents with isolated weakness in external rotation of his dominant shoulder. Physical examination reveals atrophy isolated to the infraspinatus fossa, with normal supraspinatus bulk and strength. Magnetic resonance imaging (MRI) is most likely to reveal a paralabral cyst causing nerve compression at which anatomical location?
Explanation
Question 46
During an anatomic anterior cruciate ligament (ACL) reconstruction, failure to adequately recreate the posterolateral (PL) bundle will most likely result in a persistent deficit in which of the following biomechanical functions?
Explanation
Question 47
The rotator cable is a thick band of capsuloligamentous tissue that transfers forces from the rotator cuff muscles to the humerus. According to the "suspension bridge" model proposed by Burkhart, in which of the following tear patterns is near-normal cuff kinematics most likely maintained?
Explanation
Question 48
A 24-year-old professional athlete sustains an acute, isolated grade III posterior cruciate ligament (PCL) injury. If nonoperative management is chosen, which of the following rehabilitation protocols is most appropriate during the first 2 to 4 weeks?
Explanation
Question 49
A 22-year-old collegiate football player sustains a valgus blow to the knee. Physical examination reveals a grade III medial collateral ligament (MCL) sprain with significantly increased valgus laxity at both 0 and 30 degrees of knee flexion. This finding implies a concomitant injury to which of the following structures?
Explanation
Question 50
A 65-year-old man presents with severe shoulder pain, pseudoparalysis, and an irreparable massive rotator cuff tear. Radiographs show Hamada grade 3 changes (acetabularization of the acromion). Which of the following is the most appropriate definitive surgical treatment?
Explanation
Question 51
When comparing bone-patellar tendon-bone (BTB) autograft to quadrupled hamstring autograft for ACL reconstruction, which of the following is a recognized characteristic of the BTB autograft?
Explanation
Question 52
Accurate anatomic restoration is critical during rotator cuff repair. The native footprint of the supraspinatus tendon on the greater tuberosity is best described as having which of the following approximate dimensions?
Explanation
Question 53
During the evaluation of a suspected posterolateral corner (PLC) knee injury, the dial test is performed. An increase in external rotation of 15 degrees at 30 degrees of knee flexion, but no asymmetry at 90 degrees of flexion, most strongly suggests which of the following injury patterns?
Explanation
Question 54
In the evaluation of a partial-thickness articular-sided rotator cuff tear (PASTA lesion), surgical repair (either via transtendinous technique or tear completion) is generally indicated over simple arthroscopic debridement when the tear involves what percentage of the native tendon thickness?
Explanation
Question 55
A 28-year-old male is evaluated following a traumatic posterior knee dislocation that was immediately reduced in the emergency department. His foot is warm and well-perfused, but the Ankle-Brachial Index (ABI) of the injured extremity is 0.82. What is the most appropriate next step in management?
Explanation
Question 56
The Goutallier classification is utilized on imaging to grade fatty infiltration of the rotator cuff muscles, which correlates with repair prognosis. Which Goutallier grade is specifically defined as having more fat than muscle within the muscle belly?
Explanation
Question 57
A 10-year-old boy (Tanner stage I) sustains a midsubstance ACL rupture and experiences recurrent giving-way episodes despite bracing. What is the most appropriate surgical intervention to stabilize the knee while minimizing the risk of iatrogenic growth arrest?
Explanation
Question 58
Which of the following physical examination maneuvers is considered the most sensitive test for diagnosing a superior partial tear of the subscapularis tendon?
Explanation
Question 59
A 24-year-old skier sustains a twisting injury to the knee. A plain radiograph is shown in Figure 1.
The image reveals an avulsion fracture of the lateral tibial plateau (Segond fracture). This pathognomonic finding is most strongly associated with injury to which of the following structures?
Explanation
Question 60
A 65-year-old man presents with chronic weakness in external rotation and abduction. MRI reveals a massive, retracted tear of the supraspinatus and infraspinatus. Retraction of these tendons medial to the glenoid places which nerve at greatest risk of tethering and subsequent injury?
Explanation
Question 61
A patient presents with knee pain and instability after a dashboard injury. The dial test shows 15 degrees of increased external rotation of the tibia at 30 degrees of knee flexion compared to the contralateral side, but symmetric external rotation at 90 degrees. What is the most likely diagnosis?
Explanation
Question 62
A 45-year-old weightlifter feels a pop in his anterior shoulder while bench pressing. On examination, he has increased passive external rotation and a positive lift-off test. Which tendon is most likely injured?
Explanation
Question 63
When comparing bone-patellar tendon-bone (BPTB) autografts to hamstring autografts for primary ACL reconstruction, BPTB grafts are historically associated with a higher incidence of which of the following complications?
Explanation
Question 64
A 28-year-old baseball pitcher undergoes shoulder arthroscopy. A partial articular-sided supraspinatus tendon avulsion (PASTA) involving 60% of the tendon thickness is identified. What is the most appropriate surgical management?
Explanation
Question 65
A 25-year-old male is evaluated in the trauma bay following a high-velocity anterior knee dislocation. The knee is reduced, but the ankle-brachial index (ABI) is 0.8. What is the most appropriate next step in management?
Explanation
Question 66
Compared to single-row repair, biomechanical studies of double-row rotator cuff repair demonstrate which of the following characteristics?
Explanation
Question 67
A 21-year-old football player sustains a valgus blow to the knee. MRI confirms an isolated, acute grade III injury to the medial collateral ligament (MCL) at the femoral attachment. What is the recommended treatment?
Explanation
Question 68
In the evaluation of chronic rotator cuff tears, which of the following MRI findings is the most significant predictor of structural failure after an attempted rotator cuff repair?
Explanation
Question 69
During surgical reconstruction of the posterolateral corner (PLC) of the knee, the surgeon must reconstruct the primary static stabilizer to varus stress. Which structure inserts on the lateral aspect of the fibular head, anterior to the popliteofibular ligament?
Explanation
Question 70
A 72-year-old woman with pseudoparalysis and severe rotator cuff arthropathy is scheduled for a reverse total shoulder arthroplasty (RTSA). The biomechanical advantage of RTSA relies on shifting the center of rotation in which directions compared to the native shoulder?
Explanation
Question 71
A 9-year-old prepubescent soccer player with wide-open physes sustains a complete ACL tear. Nonoperative management has failed due to recurrent instability. What is the most appropriate surgical technique to minimize the risk of limb length discrepancy and angular deformity?
Explanation
Question 72
A 35-year-old man presents with acute, severe shoulder pain that lasted for two weeks, followed by painless weakness in external rotation and forward elevation. MRI shows no rotator cuff tear but diffuse edema in the supraspinatus and infraspinatus muscles. What is the most likely diagnosis?
Explanation
Question 73
The posterior cruciate ligament (PCL) is composed of two primary bundles. Which statement accurately describes the tensioning pattern of the larger bundle during normal knee range of motion?
Explanation
Question 74
A patient complains of anterior shoulder pain exacerbated by forward elevation, adduction, and internal rotation ("cross-body" movement). MRI reveals narrowing of the coracohumeral interval to 5 mm and subscapularis tendinosis. This presentation is most consistent with:
Explanation
Question 75
A 24-year-old athlete undergoes an anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. If the femoral tunnel is inadvertently placed too far anteriorly, what is the most likely biomechanical consequence during range of motion?
Explanation
Question 76
A 65-year-old man presents with chronic shoulder weakness. Magnetic resonance imaging reveals a massive, retracted tear involving both the supraspinatus and infraspinatus tendons. Medial retraction of the supraspinatus tendon past the glenoid rim places which of the following structures at the greatest risk of tethering or traction injury?
Explanation
Question 77
A 19-year-old soccer player sustains a valgus injury to his left knee. Examination shows 10 mm of medial joint space opening at 30 degrees of flexion with a firm endpoint, but no opening at 0 degrees of flexion. What is the most appropriate initial management?
Explanation
Question 78
A 45-year-old weightlifter feels a sudden pop in his shoulder while performing heavy bench presses. Physical examination reveals significantly increased passive external rotation compared to the contralateral side and a positive belly-press test. Which of the following structures is most likely injured?
Explanation
Question 79
During an isolated posterior cruciate ligament (PCL) reconstruction using an Achilles tendon allograft, the surgeon utilizes a tibial inlay technique rather than a transtibial tunnel technique. What is the primary biomechanical advantage of the tibial inlay technique?
Explanation
Question 80
A 70-year-old patient with a chronic rotator cuff tear is evaluated for potential surgical repair. Preoperative MRI demonstrates Goutallier stage 4 fatty infiltration of the infraspinatus muscle. Which of the following best describes this finding and its clinical implications?
Explanation
Question 81
A 30-year-old motorcyclist sustains a traumatic high-velocity knee dislocation. Following emergent closed reduction in the trauma bay, ankle-brachial indices (ABI) are measured at 0.8. What is the next most appropriate step in management?
Explanation
Question 82
A 55-year-old active manual laborer undergoes arthroscopic repair of a supraspinatus tear and is found to have a concurrent high-grade partial tear of the long head of the biceps tendon. He is heavily reliant on arm strength and explicitly expresses concern regarding postoperative cosmetic deformity and muscle cramping. Which of the following is the most appropriate management for the biceps tendon?
Explanation
Question 83
A 22-year-old collegiate football player sustains a direct blow to the anteromedial aspect of his knee. Examination reveals a positive dial test at 30 degrees of knee flexion, but symmetrical external rotation at 90 degrees of flexion. Which structural injury is most consistent with these physical examination findings?
Explanation
Question 84
Incorporating the concept of margin convergence during the repair of a massive, U-shaped rotator cuff tear provides which of the following primary biomechanical benefits?
Explanation
Question 85
Compared to a bone-patellar tendon-bone autograft, the use of a non-irradiated tibialis anterior allograft for anterior cruciate ligament reconstruction in a 16-year-old competitive athlete is associated with a significantly higher risk of which of the following complications?
Explanation
Question 86
A 72-year-old woman presents with severe shoulder pain and pseudoparalysis. Radiographs show significant superior migration of the humeral head with articulation against the acromion. Which of the following is an absolute contraindication to performing a reverse total shoulder arthroplasty in this patient?
Explanation
Question 87
In ACL reconstruction utilizing a quadrupled hamstring graft and a cortical suspension button (e.g., Endobutton) for femoral fixation, the "bungee cord effect" and "windshield wiper effect" are established mechanisms that most commonly lead to which of the following postoperative radiographic findings?
Explanation
Question 88
A 21-year-old collegiate baseball pitcher presents with chronic posterior shoulder pain primarily occurring during the late cocking phase of throwing. Magnetic resonance arthrography reveals a partial-thickness articular-sided tear of the posterior supraspinatus and anterior infraspinatus, along with posterosuperior labral fraying. What is the most likely diagnosis?
Explanation
Question 89
A 28-year-old recreational skier sustains an acute ACL tear. Concurrent injury to the posterior horn of the medial meniscus root is identified on preoperative MRI. If the medial meniscus root tear is left completely untreated at the time of ACL reconstruction, the knee biomechanics will most closely resemble which of the following states?
Explanation
Question 90
A 25-year-old athlete undergoes an anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone autograft. Which of the following is the most common complication associated with this specific graft choice when compared directly to a hamstring autograft?
Explanation
Question 91
A 65-year-old man presents with pseudoparalysis of the right shoulder and a massive, irreparable posterosuperior rotator cuff tear. Anteroposterior radiographs demonstrate an acromiohumeral interval of 3 mm with superior subluxation of the humeral head. Which of the following is the most appropriate definitive surgical treatment?
Explanation
Question 92
When assessing a patient with a suspected multiligamentous knee injury, the 'dial test' is performed. Increased external rotation of the tibia of 15 degrees compared to the contralateral side at 30 degrees of flexion, but equal rotation at 90 degrees of flexion, indicates an isolated injury to which of the following structures?
Explanation
Question 93
A 45-year-old male presents with weakness in internal rotation and a positive 'lift-off' test following a traumatic shoulder dislocation. MRI confirms an isolated, retracted tear of the subscapularis tendon. During arthroscopic repair, which specific anatomical landmark helps identify the superolateral border of the retracted subscapularis tendon?
Explanation
Question 94
A 30-year-old female undergoes arthroscopic evaluation for persistent shoulder pain. An articular-sided partial-thickness supraspinatus tear (PASTA lesion) is identified. The tear involves 60% of the tendon footprint depth. What is the most appropriate surgical management?
Explanation
Question 95
During posterior cruciate ligament (PCL) reconstruction, the surgeon targets the primary function of the larger, stronger bundle of the PCL. Which bundle is this, and at what knee position is it most taut?
Explanation
Question 96
A 19-year-old football player sustains a high-energy knee injury resulting in an acute knee dislocation. Following closed reduction, his distal pulses are palpable but seem slightly asymmetric. What is the most appropriate next step in management to rule out a sight-threatening complication?
Explanation
Question 97
A 28-year-old skier sustains an isolated Grade III medial collateral ligament (MCL) tear localized entirely to the proximal (femoral) attachment. What is the most appropriate initial management for this injury?
Explanation
Question 98
During an arthroscopic anterior cruciate ligament (ACL) reconstruction using an anteromedial portal technique for femoral tunnel drilling, what is the most significant surgical risk associated with this method compared to a traditional transtibial approach?
Explanation
Question 99
A 55-year-old male with a massive rotator cuff tear is being evaluated for surgical repair. The surgeon assesses muscle quality on the preoperative MRI. According to the Goutallier classification, Grade 3 fatty infiltration of the rotator cuff muscles is defined as:
Explanation
Question 100
A 24-year-old athlete undergoes evaluation for a revision anterior cruciate ligament (ACL) reconstruction. Preoperative computed tomography (CT) reveals significant widening of the previous tibial and femoral tunnels, both measuring 17 mm in diameter. What is the most appropriate surgical strategy?
Explanation
None
