AAOS Sports Medicine MCQs (Set 4): Knee Ligament, Rotator Cuff & Concussion | Board Review

Key Takeaway
This high-yield question set for the AAOS/ABOS Sports Medicine exams (Set 4) focuses on critical areas including diagnosis and management of acute knee ligament injuries, common rotator cuff pathologies, and the latest guidelines for sports-related concussion assessment and return-to-play protocols.
AAOS Sports Medicine MCQs (Set 4): Knee Ligament, Rotator Cuff & Concussion | Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Closure of the rotator cuff interval results in elimination of which direction of shoulder instability?
Explanation
Question 2
In overhead athletic activities, the kinetic chain generates what percentage of force from the leg and trunk segments of the chain?
Explanation
Question 3
A 40-year-old right-handed professional football player reports persistent right wrist pain after falling during a game 5 days ago. A radiograph is shown in Figure 21. Management should consist of

Explanation
Question 4
A 29-year-old ultramarathoner, who is halfway into a 50-mile race, is sweating profusely. He suddenly collapses, is unresponsive, and has violent muscle contractions. Prior to these symptoms, he had been drinking water at every water stop (every 1 mile). What is the most likely diagnosis?
Explanation
Question 5
A 12-year-old Little League pitcher reports lateral elbow pain and "catching." Examination reveals painful pronation and supination and tenderness over the lateral elbow. Radiographs are shown in Figures 22a and 22b. Initial management should consist of

Explanation
Question 6
Medial dislocation of the long head of the biceps tendon in the shoulder is most commonly caused by a
Explanation
Question 7
Tension force in the anterior cruciate ligament during passive range of motion is highest at
Explanation
Question 8
Compared to eumenorrheic athletes, amenorrheic athletes have more frequent occurrences of
Explanation
Question 9
Figure 23 shows the postoperative radiograph of a patient who underwent an anterior cruciate ligament (ACL) reconstruction (with bone-patella tendon-bone autograft) that failed. He initially had loss of flexion postoperatively. What is the most likely cause of this failure?

Explanation
Question 10
A 22-year-old man reports anterior knee pain, swelling, and is unable to perform a straight leg raise after undergoing endoscopic anterior cruciate ligament (ACL) reconstruction with a bone-patellar tendon-bone autograft 1 week ago. He is afebrile. Examination reveals a clean incision, moderate effusion, a weak isometric quadriceps contraction, active knee range of motion of 5 degrees to 45 degrees, and the patella is ballottable. Knee radiographs show postoperative changes with good femoral and tibial tunnel placements, and normal patellar height. What is the next most appropriate step in management?
Explanation
Question 11
A 46-year-old woman fell from her bicycle and sustained the injury shown in Figure 24. Which of the following ligaments has been disrupted?
Explanation
Question 12
The use of knee arthroscopy following total knee arthroplasty is most effective in treating which of the following conditions?
Explanation
Question 13
Significant anterior tibial translation occurs during which of the following rehabilitation exercises?
Explanation
Question 14
A 22-year-old volleyball player reports the insidious onset of superior and posterior shoulder pain. Radiographs are normal. An MRI scan is shown in Figure 25. What is the most specific physical examination finding?

Explanation
Question 15
A 20-year-old male lacrosse player sustains an anterior dislocation of the shoulder. He is extremely concerned about recurrent dislocations. Which of the following treatments has been shown to reduce the risk of recurrent dislocation?
Explanation
Question 16
A 43-year-old soccer player who had knee pain following a twisting injury underwent an arthroscopic meniscectomy 6 months ago. He continues to report posterior knee pain. Examination reveals soft-tissue fullness and tenderness just above the popliteal fossa, trace knee effusion, full range of knee motion, no instability, and negative meniscal signs. Radiographs show some mild medial joint space narrowing but no other bony changes. What is the next most appropriate step in management?
Explanation
Question 17
Figures 26a through 26c show the MRI scans of a 47-year-old man who underwent arthroscopic shoulder surgery 6 months ago and continues to have pain despite a prolonged course of rehabilitation. Management should now consist of
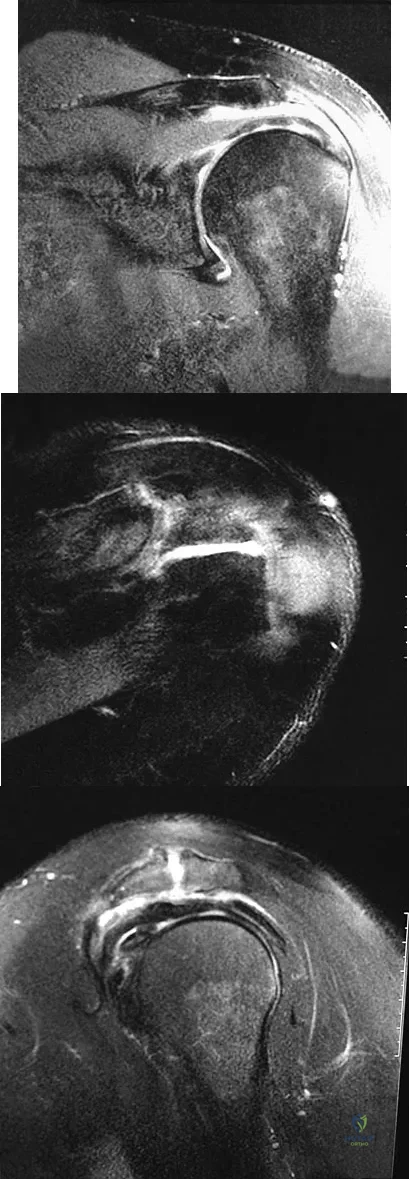
Explanation
Question 18
An 18-year-old rugby player has had pain in his ring finger after missing a tackle 1 week ago. Examination reveals tenderness in the distal palm, and he is unable to actively flex the distal interphalangeal (DIP) joint. Radiographs are normal. What is the most appropriate management?
Explanation
Question 19
Storage of musculoskeletal allografts by cryopreservation is achieved by
Explanation
Question 20
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with
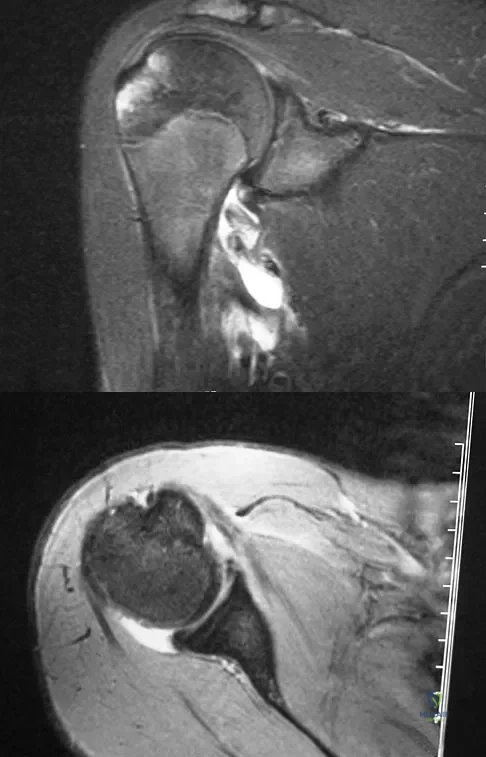
Explanation
Question 21
Closed-chain exercise differs from open-chain exercise in which of the following ways?
Explanation
Question 22
What procedure can eliminate a sulcus sign?
Explanation
Question 23
An eversion mechanism of injury is associated with which of the following ankle conditions?
Explanation
Question 24
Which of the following anatomic structures are in contact with internal impingement in the throwing athlete?
Explanation
Question 25
Second impact syndrome (SIS) after head injury is characterized by which of the following?
Explanation
Question 26
A 19-year-old collegiate soccer player sustains a concussion during a match. He is completely asymptomatic at rest 4 days post-injury and has normal neurocognitive testing. What is the correct next step in his management according to the standard stepwise return-to-play guidelines?
Explanation
Question 27
In a patient undergoing superior capsular reconstruction (SCR) for an irreparable posterosuperior rotator cuff tear, the graft is primarily designed to act as a static restraint against which abnormal kinematic motion?
Explanation
Question 28
A patient presents with a combined grade III posterior cruciate ligament (PCL) injury and posterolateral corner (PLC) injury. During biomechanical testing, isolated sectioning of the popliteofibular ligament would result in maximum increased external tibial rotation at which knee flexion angle?
Explanation
Question 29
Which of the following pathophysiological mechanisms is primarily responsible for the rapid deterioration and high mortality seen in Second Impact Syndrome?
Explanation
Question 30
A 55-year-old laborer has a massive, irreparable subscapularis tendon tear. He presents with severe weakness in internal rotation, a positive belly-press test, and pain. Which of the following tendon transfers is the most appropriate surgical option to restore function?
Explanation
Question 31
Which of the following is the most frequently reported complication associated with the use of a bone-patellar tendon-bone (BPTB) autograft for anterior cruciate ligament (ACL) reconstruction?
Explanation
Question 32
During the sideline evaluation of an athlete with a suspected concussion, the Vestibular/Ocular Motor Screening (VOMS) tool is utilized. Which of the following is NOT a standard component of this assessment?
Explanation
Question 33
When performing an arthroscopic rotator cuff repair, aggressive medial mobilization of a chronically retracted supraspinatus tendon places the suprascapular nerve at greatest risk of traction injury at which anatomic location?
Explanation
Question 34
In an anatomic posterolateral corner (PLC) reconstruction using the LaPrade technique, the fibular attachment of the fibular collateral ligament (FCL) graft should be placed:
Explanation
Question 35
According to the Goutallier classification evaluated on non-contrast CT or MRI, which stage of fatty infiltration in the rotator cuff musculature represents an equal amount of fat and muscle tissue?
Explanation
Question 36
A 25-year-old male presents with lateral knee pain after a rugby tackle. The Dial test demonstrates 15 degrees of increased external rotation compared to the contralateral knee at 30 degrees of flexion, but symmetric rotation at 90 degrees of flexion. What is the most likely diagnosis?
Explanation
Question 37
In the immediate sideline assessment of a suspected concussion using the SCAT tool, which of the following findings is considered a 'Red Flag' that necessitates immediate removal from play and emergency medical evaluation?
Explanation
Question 38
A 45-year-old overhead throwing athlete undergoes shoulder arthroscopy. A PASTA (Partial Articular Supraspinatus Tendon Avulsion) lesion is identified involving 60% of the tendon footprint. What is the most appropriate management?
Explanation
Question 39
A 22-year-old soccer player sustains an isolated Grade III medial collateral ligament (MCL) tear at the femoral insertion. What anatomic characteristic is the primary reason this injury often heals well with nonoperative management?
Explanation
Question 40
In the transverse plane of the shoulder, the dynamic glenohumeral force couple that acts to compress and stabilize the humeral head against the glenoid during active motion is primarily formed by the:
Explanation
Question 41
A 10-year-old female with wide-open physes sustains a complete midsubstance ACL tear. When planning an all-epiphyseal ACL reconstruction, which anatomical structure is at greatest risk of iatrogenic injury during femoral tunnel drilling?
Explanation
Question 42
Which of the following premorbid factors is most strongly associated with a prolonged recovery and the development of Post-Concussion Syndrome (PCS) following a sport-related mild traumatic brain injury?
Explanation
Question 43
A 35-year-old overhead athlete undergoes an MRI of the shoulder which reveals a type II SLAP tear and a paralabral cyst located in the spinoglenoid notch. Which isolated physical examination finding is most likely to be present?
Explanation
Question 44
A 29-year-old male sustains a knee dislocation (KD-III) with complete disruption of the ACL, PCL, and MCL. After closed reduction, his ankle-brachial index (ABI) is 0.7. What is the most appropriate next step in management?
Explanation
Question 45
Following an arthroscopic rotator cuff repair, a patient develops severe, global shoulder stiffness and pain out of proportion to the surgical intervention. Inflammatory markers are completely normal. What is the most effective initial management for this condition?
Explanation
Question 46
A 19-year-old college football player suffers a concussion during a game. He is symptom-free at rest 3 days later. Once the athlete is asymptomatic at rest, how many minimum days are required to complete the standard graduated return-to-play protocol before full-contact gameplay?
Explanation
Question 47
Which of the following anterior cruciate ligament (ACL) reconstruction graft choices is most uniquely associated with an increased risk of postoperative patellar fracture?
Explanation
Question 48
A 45-year-old male presents with weakness in external rotation and a massive, retracted posterosuperior rotator cuff tear. Retraction of the supraspinatus tendon medial to the glenoid rim is most likely to cause traction injury to the suprascapular nerve at which of the following anatomical locations?
Explanation
Question 49
A 25-year-old rugby player sustains a blow to the anteromedial aspect of his knee while it is fully extended and his foot is planted. Examination reveals a positive dial test at 30 degrees of knee flexion, but symmetric external rotation at 90 degrees compared to the contralateral side. Which structure is predominantly injured?
Explanation
Question 50
A 55-year-old smoker undergoes an arthroscopic rotator cuff repair. Nicotine primarily impairs tendon-to-bone healing by downregulating which of the following processes at the repair site?
Explanation
Question 51
Second impact syndrome, a rare but often fatal complication following a premature return to play after a concussion, is primarily driven by which of the following pathophysiological mechanisms?
Explanation
Question 52
During a posterior cruciate ligament (PCL) reconstruction, the surgeon aims to anatomically reconstruct the anterolateral (AL) bundle. Which of the following accurately describes the tensioning pattern of the native AL bundle of the PCL?
Explanation
Question 53
A 28-year-old professional baseball pitcher presents with shoulder pain. MRI arthrography reveals a partial articular-sided supraspinatus tendon avulsion (PASTA) involving 60% of the tendon footprint. After failing nonoperative management, what is the most appropriate surgical treatment?
Explanation
Question 54
A 22-year-old female skier sustains a twisting injury to her knee. Radiographs reveal a small avulsion fracture of the lateral tibial plateau (Segond fracture). This radiographic finding is pathognomonic for a concomitant injury to which of the following structures?
Explanation
Question 55
Superior capsular reconstruction (SCR) is considered for younger patients with massive, irreparable posterosuperior rotator cuff tears. The primary biomechanical goal of this procedure is to prevent which of the following?
Explanation
Question 56
Which of the following components of the Sport Concussion Assessment Tool 5 (SCAT5) is specifically designed to evaluate delayed recall?
Explanation
Question 57
A 30-year-old male sustains an isolated Grade III medial collateral ligament (MCL) tear of the knee. What is the most appropriate initial management for this injury?
Explanation
Question 58
During the physical examination of a patient with suspected rotator cuff pathology, the examiner performs the "belly-press" test. The patient is unable to maintain pressure on their abdomen without bringing their elbow posterior to the mid-coronal plane. This finding indicates weakness of which muscle?
Explanation
Question 59
A 28-year-old male is brought to the emergency department after a motorcycle collision with a grossly deformed left knee. Radiographs confirm a knee dislocation. After closed reduction, his pedal pulses are asymmetric. The ankle-brachial index (ABI) on the affected side is 0.75. What is the next most appropriate step in management?
Explanation
Question 60
A 24-year-old athlete sustains a knee injury. On examination, the dial test reveals increased external rotation of the tibia compared to the contralateral side at 30 degrees of knee flexion, but symmetrical external rotation at 90 degrees of knee flexion. This examination finding is most indicative of an isolated injury to which of the following structures?
Explanation
Question 61
During arthroscopic rotator cuff repair, an anatomic restoration of the footprint is desired. The normal supraspinatus footprint on the greater tuberosity has an average medial-to-lateral width of approximately:
Explanation
Question 62
A 16-year-old high school football player is diagnosed with a concussion after a helmet-to-helmet collision. According to the current Consensus Statement on Concussion in Sport, when is the athlete allowed to return to full competition?
Explanation
Question 63
A 55-year-old man presents with anterior shoulder pain and weakness. On examination, he is unable to hold his hand pressed against his abdomen when the elbow is brought anterior to the coronal plane. This finding (a positive Bear-hug or Belly-press test) is most sensitive for detecting a tear of which portion of the rotator cuff?
Explanation
Question 64
Second impact syndrome is a rare but potentially fatal complication occurring when a second concussive blow is sustained before full recovery from an initial concussion. The rapid mortality associated with this syndrome is primarily driven by:
Explanation
Question 65
A 22-year-old soccer player presents with a recurrent knee effusion and instability 4 months after an anterior cruciate ligament (ACL) reconstruction with bone-patellar tendon-bone autograft. What is the most common cause of early failure (within 6 months) following ACL reconstruction?
Explanation
Question 66
A 68-year-old woman with a massive, retracted rotator cuff tear involving the supraspinatus and entire infraspinatus presents with 'pseudoparalysis' of forward elevation. In the setting of an intact subscapularis, this pseudoparalysis indicates a disruption of which biomechanical force couple?
Explanation
Question 67
Which of the following factors is considered the strongest predictor of a prolonged recovery (post-concussion syndrome) following a sports-related concussion?
Explanation
Question 68
A radiograph of a 25-year-old skier demonstrates an elliptical cortical avulsion fracture of the lateral aspect of the proximal tibia, just distal to the articular surface (Segond fracture). This radiographic finding is virtually pathognomonic for an injury to which of the following structures?
Explanation
Question 69
When evaluating a patient for a rotator cuff repair, preoperative MRI is used to assess muscle quality via the Goutallier classification. Which Goutallier stage is defined as having equal amounts of fat and muscle within the rotator cuff muscle belly?
Explanation
Question 70
A 21-year-old collegiate hockey player sustains an isolated Grade III tear of the medial collateral ligament (MCL) at its femoral insertion. There is no meniscal or cruciate ligament pathology. What is the most appropriate initial management?
Explanation
Question 71
The rotator cuff interval is a triangular anatomic space in the anterior shoulder bounded by the supraspinatus superiorly, the subscapularis inferiorly, and the coracoid process medially. Which of the following structures passes through this interval?
Explanation
Question 72
According to the Canadian CT Head Rule, which of the following is an absolute indication for obtaining a non-contrast CT scan of the head in a 20-year-old concussed athlete with a Glasgow Coma Scale (GCS) score of 15?
Explanation
Question 73
The posterior cruciate ligament (PCL) is composed of two primary functional bundles. In which position of the knee is the anterolateral (AL) bundle of the PCL at its maximum tension?
Explanation
Question 74
Superior Capsular Reconstruction (SCR) is a joint-preserving surgical option for massive, irreparable posterosuperior rotator cuff tears. In this procedure, the graft is anchored medially to the superior glenoid and laterally to the:
Explanation
Question 75
A 28-year-old football player sustains a severe varus and hyperextension injury to his knee, resulting in a posterolateral corner (PLC) injury. Post-injury, he complains of numbness over the dorsum of his foot and an inability to dorsiflex his ankle. Which nerve is most likely injured?
Explanation
Question 76
Massive retraction of a supraspinatus tear medial to the glenoid rim significantly increases the risk of traction neuropathy to the suprascapular nerve. At which anatomic location does this traction most commonly tether and compress the nerve?
Explanation
Question 77
The acute neurometabolic cascade of a sports-related concussion begins immediately following biomechanical injury to the brain. This initial phase is characterized by an abrupt release of excitatory neurotransmitters (like glutamate) and a massive cellular efflux of which ion?
Explanation
Question 78
The anterolateral ligament (ALL) of the knee has gained attention as an important secondary restraint to internal tibial rotation. From its femoral origin near the lateral epicondyle, where is its primary insertion site on the tibia?
Explanation
Question 79
The anterior cruciate ligament (ACL) is anatomically composed of two bundles named for their tibial insertion sites. Which bundle is primarily responsible for rotational stability and is tightest in knee extension?
Explanation
Question 80
A 19-year-old collegiate soccer player sustains a concussion during a game. She undergoes a period of rest and is completely asymptomatic at rest 48 hours later. According to the standard graduated return-to-play protocol, what is the next step in her management?
Explanation
Question 81
A 25-year-old rugby player falls directly onto his flexed right knee. Examination reveals a positive posterior drawer test at 90 degrees of flexion. The dial test demonstrates 20 degrees of increased external rotation at 30 degrees of flexion, and 25 degrees of increased external rotation at 90 degrees of flexion compared to the contralateral knee. Which structures are injured?
Explanation
Question 82
A 35-year-old elite tennis player presents with a PASTA (Partial Articular Supraspinatus Tendon Avulsion) lesion involving 60% of the tendon footprint depth. He has failed 6 months of conservative management. What is the most appropriate surgical treatment?
Explanation
Question 83
A high school football player returns to play before completely resolving symptoms from a prior concussion. He sustains a seemingly minor blow to the head and rapidly collapses, progressing to a coma. This catastrophic cascade (Second Impact Syndrome) is primarily driven by:
Explanation
Question 84
When utilizing a bone-patellar tendon-bone (BTB) autograft for ACL reconstruction, placing the femoral tunnel too anteriorly (shallow) within the intercondylar notch will result in which of the following kinematic abnormalities?
Explanation
Question 85
A 72-year-old female presents with pseudoparalysis of the right shoulder and severe pain. Radiographs reveal superior migration of the humeral head with articulation against the acromion. MRI confirms a massive, retracted, irrepairable rotator cuff tear with significant fatty atrophy, but an intact deltoid muscle. What is the most appropriate definitive surgical option?
Explanation
Question 86
A 22-year-old collegiate skier sustains an isolated Grade III MCL tear of the left knee. There is valgus gapping at both 0 and 30 degrees, but ACL and PCL are intact on MRI. Which of the following represents the most widely accepted initial management?
Explanation
Question 87
Which of the following components of the SCAT5 (Sport Concussion Assessment Tool 5) is utilized specifically to assess an athlete's immediate memory?
Explanation
Question 88
A 26-year-old male presents for a revision ACL reconstruction. Preoperative CT scan demonstrates extensive femoral and tibial tunnel osteolysis, with both tunnels measuring 16 mm in diameter. What is the most appropriate next step in management?
Explanation
Question 89
During an arthroscopic rotator cuff repair, extensive medial mobilization of a massive, chronically retracted supraspinatus tear is required. Which neurological structure is at greatest risk of injury during this mobilization, particularly if releasing the coracohumeral ligament near the base of the coracoid?
Explanation
Question 90
A 28-year-old male sustains a traumatic knee dislocation (KD-III). Following closed reduction, examination reveals an inability to dorsiflex the foot and numbness over the dorsum of the foot.
Injury to which specific ligamentous complex of the knee is most highly associated with this neurologic deficit?
Explanation
Question 91
According to the Goutallier classification for rotator cuff fatty infiltration evaluated on MRI, a supraspinatus muscle belly that demonstrates equal amounts of fat and muscle tissue is classified as:
Explanation
Question 92
Following a concussive brain injury in an athlete, the initial neurometabolic cascade is characterized by an abrupt and massive release of which neurotransmitter, ultimately leading to a toxic intracellular influx of calcium?
Explanation
Question 93
A 10-year-old male (Tanner stage 1) sustains a complete ACL tear playing soccer. He has significant subjective instability. To minimize the risk of premature physeal closure and growth arrest, which of the following surgical techniques is most appropriate?
Explanation
Question 94
A 45-year-old recreational weightlifter feels a sharp pop in his anterior shoulder during a heavy bench press. Exam reveals increased passive external rotation and a distinctly positive belly-press test.
What other associated pathology must the surgeon be highly suspicious of during arthroscopic evaluation?

Explanation
None
