Shoulder Orthopedic MCQs (Set 1): Rotator Cuff & Instability | AAOS & ABOS Board Review

Key Takeaway
This high-yield question set (Set 1) for AAOS, ABOS, and OITE exams focuses on comprehensive shoulder pathology. It covers rotator cuff tears, glenohumeral instability, impingement syndrome, and arthroscopic techniques, providing essential practice for board certification.
Shoulder Orthopedic MCQs (Set 1): Rotator Cuff & Instability | AAOS & ABOS Board Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following statements best describes why the ulnar nerve is most prone to neuropathy at the elbow?
Explanation
Question 2
Figure 1 shows the radiograph of a 71-year-old man who has had increasing pain and weakness in his shoulder for the past 3 years. Nonsurgical management has failed to provide relief. Examination shows 130 degrees of active forward flexion and intact external rotation strength. During surgery, a 1- x 1-cm rotator cuff tear involving the supraspinatus is encountered. Treatment should include
Explanation
Question 3
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?
Explanation
Question 4
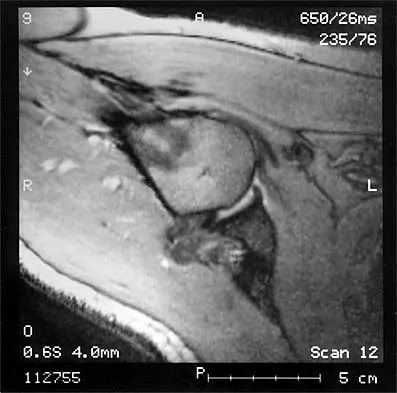
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?
Explanation
Question 5
Figure 3 shows the radiographs of a 32-year-old man who fell 12 feet onto his outstretched arm and sustained a fracture-dislocation of the elbow. Initial management consisted of closed reduction of the dislocation. Surgical treatment should now include repair or reduction and fixation of the
Explanation
Question 6
It is important to avoid which of the following exercises in the immediate postoperative period after humeral head replacement for an acute four-part fracture?
Explanation
Question 7
A 38-year-old man has winging of the ipsilateral scapula after undergoing a transaxillary resection of the first rib 3 weeks ago. What is the most likely cause of this finding?
Explanation
Question 8
A 73-year-old man who underwent repair of the left rotator cuff 6 years ago reports good pain relief but notes residual weakness of the left shoulder, especially with overhead tasks. He denies having pain at night and has minimal discomfort with activities of daily living but is dissatisfied with his shoulder strength. Radiographs show an acromiohumeral interval of 2 mm. Appropriate management should consist of
Explanation
Question 9
A 45-year-old woman has had progressive right shoulder pain for the past 6 months. She notes that the pain disrupts her sleep, she has pain at rest that requires the use of narcotic analgesics, and she has limited use of her left shoulder for most activities of daily living. History reveals the use of corticosteroids for systemic lupus erythematosus. Examination shows diminished range of motion. Radiographs of the right shoulder are shown in Figures 4a and 4b. Treatment should consist of
Explanation
Question 10
The relocation test is most reliable for diagnosing anterior subluxation of the glenohumeral joint when
Explanation
Question 11
A 16-year-old high school pitcher notes acute pain on the medial side of his elbow during a pitch. Examination that day reveals medial elbow tenderness, pain with valgus stress, mild swelling, and loss of extension. Plain radiographs show closed physes and no fracture. Which of the following diagnostic studies will best reveal his injury?
Explanation
Question 12
Figures 5a and 5b show the radiographs of a 45-year-old patient. What is the most likely diagnosis?
Explanation
Question 13
A 14-year-old boy sustains a twisting injury to his right shoulder and recalls feeling a snap during a wrestling match. Examination shows hesitancy to raise the arm away from the side, diffuse tenderness and swelling of the upper arm, and no evidence of neurovascular compromise. Figures 6a and 6b show an AP radiograph and MRI scan. What is the most likely diagnosis?
Explanation
Question 14
Figure 7 shows the radiograph of an otherwise healthy 65-year-old man who injured his right dominant shoulder while skiing 18 months ago. He did not seek treatment at the time of the injury. He now reports intermittent soreness when playing golf but has no other limitations. Examination reveals full range of motion and no tenderness, but he has slight pain with a crossed arm adduction stress test. He is neurologically intact. Initial management should consist of
Explanation
Question 15
Figure 8 shows the AP radiograph of a 33-year-old woman who sustained a midshaft clavicle fracture from a motorcycle accident 15 months ago. She continues to have significant pain with activities of daily living. Management should consist of
Explanation
Question 16
A 62-year-old patient with rheumatoid arthritis has had pain and instability of the elbow following total elbow replacement 2 years ago. A complete work-up, including aspiration and cultures, is negative. Figures 9a and 9b show the AP and lateral radiographs. Treatment should consist of
Explanation
Question 17
A 21-year-old football player reports increasing pain and a deformity involving his chest after colliding with another player during a scrimmage. Imaging studies confirm an anterior sternoclavicular dislocation. Management should consist of
Explanation
Question 18
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should
Explanation
Question 19
What is the most common contracture deformity of the spastic shoulder secondary to a cerebrovascular accident?
Explanation
Question 20
A 21-year-old collegiate pitcher has had pain in his dominant shoulder for the past 3 months despite management consisting of rest, rehabilitation, and an analysis of throwing mechanics. An arthroscopic photograph from the posterior portal is shown in Figure 10. The biceps anchor to the bone was not detached to probing. Treatment of the lesion to the left of the cannula should consist of arthroscopic
Explanation
Question 21
After humeral head replacement for four-part fractures, what is the most commonly reported difficulty?
Explanation
Question 22
Figures 11a and 11b show the AP and lateral radiographs of a 32-year-old patient on hemodialysis who has increasing elbow pain and a visibly growing mass over the extensor surface. Figure 11c shows the photomicrograph of the biopsy specimen. What is the most likely diagnosis?
Explanation
Question 23
A 52-year-old man who was a former high school pitcher now reports loss of elbow flexion and extension with pain at the extremes of motion. Nonsurgical management has failed to provide relief. Examination reveals movement from 50 degrees to 110 degrees and is painful only at the limits of motion. A radiograph is shown in Figure 12. Treatment should consist of
Explanation
Question 24
A 79-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing right shoulder pain for the past year, and nonsurgical management has failed to provide relief. Her neurologic examination is entirely normal, but she is unable to elevate her arm against gravity. An AP radiograph is shown in Figure 13. Treatment should consist of
Explanation
Question 25
A 22-year-old woman has had progressive upper extremity weakness for the past several years. History reveals no pain in her neck or shoulders. Examination reveals scapular winging of both shoulders and weakness in external rotation. She can abduct to only 120 degrees bilaterally, and there is mild supraspinatus weakness. She is otherwise neurologically intact with normal sensation and reflexes; however, she has difficulty whistling. A clinical photograph is shown in Figure 14. What is the most likely diagnosis?
Explanation
Question 26
A 22-year-old collegiate rugby player presents with his fourth anterior shoulder dislocation this season. A 3D CT scan of the shoulder reveals 26% anterior glenoid bone loss. Which of the following is the most appropriate surgical management to minimize his risk of recurrent instability?
Explanation
Question 27
A 68-year-old man presents with severe shoulder pain and an inability to actively elevate his arm past 45 degrees, though passive motion is full. MRI reveals a massive, retracted, and fatty-infiltrated tear of the supraspinatus and infraspinatus. The subscapularis and teres minor are intact. Radiographs show no significant glenohumeral osteoarthritis. What is the most reliable surgical option to restore active elevation?

Explanation
Question 28
A 35-year-old man presents to the emergency department with a locked posterior shoulder dislocation following a seizure. Following closed reduction, a CT scan reveals an anteromedial humeral head impaction fracture (reverse Hill-Sachs lesion) involving 30% of the articular surface. Which of the following is the most appropriate surgical treatment?
Explanation
Question 29
A 55-year-old woman is diagnosed with a massive, chronically retracted rotator cuff tear involving the supraspinatus and infraspinatus. She demonstrates profound weakness in external rotation. Electromyography (EMG) reveals denervation of the infraspinatus. What is the most likely mechanism of nerve injury in this setting?
Explanation
Question 30
A 19-year-old female gymnast complains of bilateral shoulder pain and a sensation of the shoulders "sliding out of joint." Physical exam demonstrates a positive sulcus sign bilaterally that persists in external rotation, positive apprehension tests, and generalized ligamentous laxity. What is the most appropriate initial management?
Explanation
Question 31
A 52-year-old construction worker complains of deep anterior shoulder pain, particularly when using a hammer. Examination reveals a positive O'Brien's active compression test and tenderness in the bicipital groove. MRI arthrogram demonstrates an isolated Type II SLAP tear. Nonoperative management has failed. What is the preferred surgical intervention?
Explanation
Question 32
Following a traumatic anterior shoulder dislocation, a 45-year-old man reports persistent anterior shoulder pain and significant weakness when trying to tuck his shirt into his pants behind his back. Which of the following physical examination tests is most sensitive and specific for evaluating the suspected torn structure?
Explanation
Question 33
A 25-year-old recreational athlete presents with recurrent anterior shoulder instability. A 3D CT scan shows 12% anterior glenoid bone loss and a large, engaging Hill-Sachs lesion. Which of the following surgical procedures is most appropriate to address both pathologies?
Explanation
Question 34
A 21-year-old elite collegiate baseball pitcher presents with pain in the posterior aspect of his throwing shoulder during the late cocking phase of throwing. He has glenohumeral internal rotation deficit (GIRD) of 25 degrees compared to his non-throwing arm. What is the most likely associated arthroscopic finding?
Explanation
Question 35
The normal direct tendon insertion of the rotator cuff onto the greater tuberosity is divided into four distinct histological zones. Which structure marks the boundary between uncalcified fibrocartilage and calcified fibrocartilage?
Explanation
Question 36
A 40-year-old man presents with anterior shoulder pain that worsens with cross-body adduction and internal rotation. Examination demonstrates focal tenderness over the coracoid process. MRI reveals a narrowed coracohumeral interval of 4 mm and edema in the lesser tuberosity. Which tendon is most at risk of attritional tearing in this syndrome?
Explanation
Question 37
During the late cocking phase of a throwing motion, the shoulder is in maximum abduction and external rotation. In this specific position, which capsuloligamentous structure provides the primary static restraint to anterior translation of the humeral head?
Explanation
Question 38
A 75-year-old woman has advanced rotator cuff tear arthropathy. Radiographs reveal superior migration of the humeral head with articulation against the acromion (acetabularization).
What biomechanical alteration is the primary driver of this superior head migration?

Explanation
Question 39
During an open repair of a massive, chronically retracted rotator cuff tear, the surgeon performs aggressive lateral mobilization of the supraspinatus tendon. Postoperatively, the patient is noted to have a new, isolated profound weakness in external rotation, with intact forward elevation. Injury to which structure most likely occurred during mobilization?
Explanation
Question 40
A 50-year-old male arrives in the emergency department with an acute anterior shoulder dislocation after a fall. Following successful closed reduction, he reports a patch of numbness over the lateral aspect of his shoulder and exhibits weakness when attempting to actively abduct the arm. Which nerve is most commonly injured in this injury pattern?
Explanation
Question 41
A 22-year-old collegiate rugby player presents with recurrent anterior shoulder instability. A 3D CT scan demonstrates 25% anterior glenoid bone loss. Which of the following is the most appropriate surgical management?
Explanation
Question 42
A 35-year-old overhead athlete complains of vague posterior shoulder pain and weakness. Physical examination reveals normal active forward elevation and abduction, but notable weakness in external rotation with the arm at the side. An MRI arthrogram reveals a paralabral cyst. Where is the cyst most likely located?
Explanation
Question 43
A 45-year-old construction worker presents with chronic, deep shoulder pain. MRI confirms an isolated Type II SLAP (Superior Labrum Anterior and Posterior) tear. Conservative management has failed. Which of the following surgical interventions is associated with the most reliable return to work and pain relief in this patient demographic?
Explanation
Question 44
A 65-year-old man is incidentally found to have an asymptomatic, 1.5 cm full-thickness supraspinatus tear on an MRI obtained for a suspected neck issue. He has full range of motion and 5/5 strength. What is the most accurate information regarding the natural history of his rotator cuff tear?
Explanation
Question 45
A 19-year-old collegiate rugby player presents with recurrent anterior shoulder instability. A 3D CT scan reveals 28% anterior glenoid bone loss. Which of the following is the most appropriate definitive management?
Explanation
Question 46
A 55-year-old woman is evaluated for right shoulder pain and weakness after a fall. On examination, she has increased passive external rotation compared to the contralateral side. The "belly-press" test is positive, but the "lift-off" test is negative. Which of the following statements best describes her pathology?
Explanation
Question 47
A 35-year-old man presents to the emergency department after a generalized tonic-clonic seizure. His arm is locked in internal rotation. Radiographs reveal a posterior shoulder dislocation. CT scan shows an anteromedial humeral head impression fracture (reverse Hill-Sachs lesion) involving 45% of the articular surface. What is the most appropriate surgical treatment?
Explanation
Question 48
A 17-year-old female gymnast complains of bilateral shoulder pain and a feeling of the shoulders "sliding out of place." Examination shows a positive sulcus sign bilaterally, positive apprehension, and generalized ligamentous laxity. There is no history of a discrete traumatic dislocation. What is the most appropriate initial management?
Explanation
Question 49
A 72-year-old man presents with chronic, severe right shoulder pain and an inability to actively elevate his arm past 40 degrees. Radiographs demonstrate superior migration of the humeral head with acromiohumeral articulation and severe glenohumeral osteoarthritis. MRI shows a massive, retracted supraspinatus and infraspinatus tear. What is the optimal surgical treatment?
Explanation
Question 50
During a Latarjet procedure for recurrent anterior shoulder instability, the conjoined tendon is retracted medially to expose the subscapularis. Which of the following nerves is at greatest risk of injury with overly aggressive medial retraction of the conjoined tendon?
Explanation
Question 51
A 28-year-old elite volleyball attacker presents with vague posterior shoulder pain and noticeable atrophy over the scapula. On examination, she has 5/5 strength in forward elevation but isolated 3/5 strength in external rotation with the arm at the side. What is the most likely pathological finding on MRI?
Explanation
Question 52
A 22-year-old rugby player presents with recurrent anterior shoulder instability. A 3D-CT scan demonstrates 28% anterior glenoid bone loss. Which of the following is the most appropriate surgical management?
Explanation
Question 53
A 72-year-old woman presents with severe shoulder pain, active forward elevation to 50 degrees, and a positive drop arm test. Radiographs show a superiorly migrated humeral head with severe glenohumeral osteoarthritis. MRI confirms a massive, retracted rotator cuff tear with grade 4 fatty infiltration. What is the most appropriate treatment?
Explanation
Question 54
A 45-year-old man falls on an outstretched hand and presents with weakness in internal rotation and a positive belly-press test. Which of the following structures is most commonly injured concomitantly with the suspected tendon tear?
Explanation
Question 55
A 35-year-old man presents to the emergency department locked in internal rotation after a generalized tonic-clonic seizure. Radiographs confirm a posterior shoulder dislocation. CT scan shows a reverse Hill-Sachs lesion involving 35% of the articular surface. Which of the following is the most appropriate treatment?
Explanation
Question 56
A 28-year-old elite volleyball attacker presents with painless, isolated weakness in external rotation of her dominant shoulder. MRI reveals a paralabral cyst. At which of the following anatomic locations is the cyst most likely compressing the affected nerve?
Explanation
Question 57
In the evaluation of a patient with a massive rotator cuff tear, which of the following factors on preoperative MRI is the strongest independent predictor of structural failure following surgical repair?
Explanation
Question 58
A 25-year-old male with recurrent anterior shoulder instability has a glenoid track evaluated on CT. He has 10% anterior glenoid bone loss and a large Hill-Sachs lesion that extends outside the glenoid track. What is the most appropriate surgical management?
Explanation
Question 59
A 30-year-old rugby player presents with recurrent anterior shoulder instability. MRI arthrogram shows no labral tear, but reveals contrast extravasation into the axillary pouch and the normal U-shape of the axillary recess is lost, appearing as a J-shape. What is the most likely diagnosis?
Explanation
Question 60
A 40-year-old overhead athlete undergoes shoulder arthroscopy for chronic pain. An articular-sided, partial-thickness supraspinatus tear (PASTA lesion) is identified. Debridement reveals the tear involves 60% of the tendon footprint thickness. What is the recommended management?
Explanation
Question 61
A 19-year-old gymnast complains of bilateral shoulder pain and a feeling of instability. Physical exam reveals generalized ligamentous laxity, a positive sulcus sign, and apprehension with anterior, posterior, and inferior translation. She has failed 6 months of targeted physical therapy. What is the next best step in management?
Explanation
Question 62
A 55-year-old woman presents with persistent anterior shoulder pain exacerbated by forward elevation and internal rotation. MRI reveals a narrowed coracohumeral interval measuring 5 mm, edema in the subcoracoid space, and a partial-thickness tear of the subscapularis tendon. What is the most likely diagnosis?
Explanation
Question 63
A 22-year-old collegiate baseball pitcher reports deep shoulder pain during the late cocking phase of throwing. MRI arthrogram demonstrates contrast extending between the superior labrum and the glenoid, and arthroscopy reveals the superior labrum and biceps anchor are completely detached from the superior glenoid. What type of SLAP tear is this?
Explanation
Question 64
During a Latarjet procedure, the coracoid process is osteotomized and transferred to the anterior glenoid. Which of the following nerves is at greatest risk of iatrogenic injury during the coracoid mobilization and transfer?
Explanation
Question 65
Reverse total shoulder arthroplasty (RTSA) is highly effective for patients with rotator cuff arthropathy. Which of the following best describes the primary biomechanical advantage of RTSA compared to anatomic total shoulder arthroplasty?
Explanation
Question 66
The "rotator cable" is a thick fibrous band of tissue running perpendicular to the supraspinatus and infraspinatus muscle fibers. Its primary function is to stress-shield which of the following adjacent structures?
Explanation
Question 67
A 26-year-old man presents to the emergency department with a locked left shoulder in internal rotation following a generalized tonic-clonic seizure. Radiographs reveal a posterior shoulder dislocation. Which of the following associated lesions is most likely present?
Explanation
Question 68
A 74-year-old man presents with chronic, severe shoulder pain and pseudoparalysis of the right arm. Examination demonstrates active forward elevation to 40 degrees and intact axillary nerve function.
Radiographs show severe superior migration of the humeral head with acetabularization of the acromion. What is the most appropriate surgical treatment?

Explanation
Question 69
A 29-year-old professional volleyball player presents with isolated external rotation weakness and posterior shoulder pain. MRI reveals a paralabral cyst. Compression of the suprascapular nerve at the spinoglenoid notch will result in denervation of which of the following muscles?
Explanation
Question 70
A 22-year-old rugby player presents with his fifth anterior shoulder dislocation.
3D CT imaging reveals 28% anterior glenoid bone loss. What is the most appropriate definitive surgical management?

Explanation
Question 71
A 24-year-old baseball pitcher presents with pain in the posterosuperior aspect of his throwing shoulder during the late cocking phase. Examination reveals a glenohumeral internal rotation deficit (GIRD) of 25 degrees. What is the primary underlying pathomechanism?
Explanation
Question 72
During an arthroscopic anterior stabilization for a patient with recurrent dislocations, an engaging Hill-Sachs lesion is identified. Which of the following procedures involves tenodesis of the infraspinatus tendon into the humeral defect?
Explanation
Question 73
A 30-year-old man sustains a shoulder dislocation. An MR arthrogram demonstrates extravasation of contrast into the axillary pouch, obliterating the normal U-shape and creating a "J-sign". This finding is pathognomonic for which of the following lesions?
Explanation
Question 74
During arthroscopy for recurrent anterior shoulder instability, the surgeon notes that the anterior labrum is completely torn and has medially displaced and healed along the anterior aspect of the glenoid neck. This pathology is correctly termed an:
Explanation
Question 75
A 19-year-old gymnast complains of vague, bilateral shoulder pain and a sensation of slipping. Examination reveals a prominent sulcus sign bilaterally, positive apprehension without a history of frank dislocation, and generalized ligamentous laxity. What is the most appropriate initial management?
Explanation
Question 76
A 45-year-old construction worker fell onto an outstretched arm and now complains of anterior shoulder pain and weakness. Clinical examination demonstrates a positive Gerber's lift-off test and increased passive external rotation. Which structure is most likely injured?
Explanation
Question 77
During an open Latarjet procedure, the surgeon places a self-retaining retractor medial to the conjoint tendon to expose the subscapularis. Excessive medial retraction in this area places which nerve at highest risk of injury?
Explanation
Question 78
A 35-year-old overhead athlete presents with posterior shoulder pain and isolated weakness of the deltoid and teres minor. An MRI demonstrates isolated muscular atrophy and localized vascular compression in the posterior shoulder. This syndrome is caused by compression of structures within boundaries that include all of the following EXCEPT:
Explanation
Question 79
A 52-year-old laborer presents with a massive, retracted supraspinatus and infraspinatus tear. The subscapularis is intact, the deltoid is highly functional, and there is no evidence of glenohumeral osteoarthritis on radiographs. Which of the following is the most appropriate surgical intervention?
Explanation
Question 80
A 42-year-old woman presents to the clinic with acute, extremely severe, burning shoulder pain that started spontaneously 2 weeks ago. The pain has now decreased, but she has developed profound weakness in shoulder abduction and external rotation. EMG demonstrates acute denervation. What is the most likely diagnosis?
Explanation
Question 81
A 50-year-old woman with severe adhesive capsulitis undergoes arthroscopic capsular release. The surgeon carefully releases the thickened structures within the rotator interval. Which of the following is NOT a normal anatomic component of the rotator interval?
Explanation
Question 82
When evaluating a patient for an anterior shoulder stabilization procedure, the Instability Severity Index Score (ISIS) is used to predict the risk of recurrence after an arthroscopic Bankart repair. Which of the following factors increases the ISIS score?
Explanation
Question 83
The transverse force couple of the shoulder is crucial for maintaining the humeral head centered within the glenoid during active elevation. This force couple relies on the balanced action of which of the following muscle groups?
Explanation
Question 84
A patient is evaluated for anterior shoulder pain. The examiner places the patient's arm in forward flexion, internal rotation, and cross-body adduction, which recreates the patient's sharp anterior pain. Imaging reveals a narrowed coracohumeral distance. What is the most likely diagnosis?
Explanation
Question 85
A 55-year-old physical laborer presents with persistent deep shoulder pain. MR arthrogram reveals a Type II SLAP tear. Given his age and occupation, what is the most appropriate surgical treatment if conservative management fails?
Explanation
Question 86
A 28-year-old weightlifter feels a sudden 'pop' in his axilla while performing a heavy bench press. He presents with extensive ecchymosis and loss of the anterior axillary fold. If a complete rupture of the pectoralis major occurred, which portion is typically the first to fail due to maximal eccentric stretch?
Explanation
Question 87
A 22-year-old collegiate rugby player presents with recurrent anterior shoulder instability. CT scan with 3D reconstruction reveals an "inverted pear" glenoid with 25% anterior bone loss. What is the most appropriate definitive management?
Explanation
Question 88
A 35-year-old man presents to the ER after a generalized tonic-clonic seizure. His shoulder is locked in internal rotation. Radiographs show a posterior shoulder dislocation. MRI reveals an anteromedial humeral head impaction fracture involving 35% of the articular surface. What is the most appropriate surgical management?
Explanation
Question 89
A 55-year-old man sustains a traumatic forced external rotation injury to his shoulder. He demonstrates a positive belly-press test and increased external rotation compared to the contralateral side. MRI confirms an isolated, full-thickness subscapularis tendon tear. During arthroscopic repair, which of the following additional findings is most likely to be encountered?
Explanation
Question 90
A 28-year-old elite volleyball player complains of vague posterior shoulder pain and isolated weakness in external rotation. Forward elevation and internal rotation strength are normal. MRI reveals a paralabral cyst in the spinoglenoid notch. This lesion most likely originated from which of the following pathologies?
Explanation
Question 91
A 30-year-old recreational skier presents with persistent anterior shoulder instability. An MRI arthrogram reveals extravasation of contrast into the axilla and a "J-sign" replacing the normal U-shaped inferior glenohumeral recess. What is the diagnosis?
Explanation
Question 92
Following an arthroscopic rotator cuff repair, a patient asks about the expected timeline for tendon-to-bone healing. Biomechanically, which type of collagen initially predominates at the healing tendon-bone interface before being remodeled into a stronger, more mature construct?
Explanation
Question 93
During diagnostic arthroscopy for recurrent anterior shoulder instability, the surgeon notes that the anterior labrum is avulsed but remains attached to the intact anterior scapular periosteum, having healed medially along the glenoid neck. This specific pathology is known as:

Explanation
Question 94
A 74-year-old female presents with severe right shoulder pain, pseudoparalysis, and a massive, irreparable rotator cuff tear. Radiographs show superior migration of the humeral head with an acromiohumeral distance < 2 mm. Which of the following is an absolute prerequisite for a successful Reverse Total Shoulder Arthroplasty (RTSA) in this patient?
Explanation
Question 95
A 19-year-old female competitive swimmer presents with bilateral shoulder pain and a feeling of "looseness." Examination reveals a positive sulcus sign, generalized ligamentous laxity (Beighton score 7/9), and no distinct history of trauma. Initial management for this condition should focus on:
Explanation
Question 96
When performing an open Latarjet procedure, the surgeon must be careful to avoid injury to the nerves innervating the subscapularis muscle. The upper and lower subscapular nerves are branches of which cord of the brachial plexus?
Explanation
Question 97
A 42-year-old recreational tennis player undergoes arthroscopy for refractory shoulder pain. A partial articular-sided tendon avulsion (PASTA) lesion of the supraspinatus is identified. At what depth of tendon involvement is completion of the tear and full-thickness repair generally recommended?
Explanation
Question 98
A 35-year-old laborer presents with persistent superior shoulder pain and impingement symptoms. An axillary radiograph reveals an unfused acromial apophysis (meso-acromiale) that is mobile on physical examination. After failing 6 months of conservative management, what is the recommended surgical intervention?
Explanation
Question 99
A 25-year-old professional baseball pitcher presents with pain during the late cocking phase of throwing and a "dead arm" sensation. MRI shows a Type II SLAP tear. If nonoperative management fails, what is the preferred surgical intervention to allow return to his prior level of competitive pitching?
Explanation
Question 100
The Latarjet procedure involves the transfer of the coracoid process with the attached conjoint tendon to the anterior glenoid neck. Which nerve is most at risk during the transfer and retraction of the conjoint tendon?
Explanation
None
