AAOS Sports Medicine Board Review (Set 2): Knee, Shoulder & Ankle Injuries

Key Takeaway
This high-yield Sports Medicine MCQ Set 2 targets key concepts for ABOS and OITE exams. It comprehensively covers the diagnosis, management, and surgical considerations for knee ligament injuries (ACL, PCL, MCL), shoulder instability, and prevalent ankle and foot sports trauma, preparing residents and fellows for board success.
AAOS Sports Medicine Board Review (Set 2): Knee, Shoulder & Ankle Injuries
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What type of exercise is used early in the rehabilitation process to safely stimulate co-contraction of the scapular and rotator cuff muscles?
Explanation
Question 2
Which of the following cardiac conditions is considered an absolute contraindication to vigorous exercise?
Explanation
Question 3
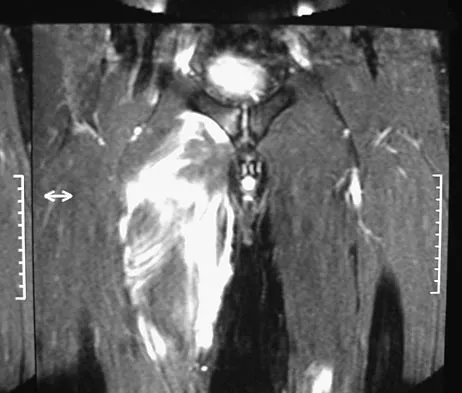
A 36-year-old professional baseball player reports the acute onset of severe right groin pain while attempting to avoid being hit by a baseball while at bat. Examination reveals tenderness, soft-tissue swelling, and ecchymosis in the right groin extending over the medial thigh. MRI scans are shown in Figures 8a and 8b. Management should consist of
Explanation
Question 4
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured?
Explanation
Question 5
Which of the following is considered the most common long-term effect on the spine of a professional race horse jockey?
Explanation
Question 6
An 18-year-old lacrosse player is diagnosed with infectious mononucleosis. What is the recommendation for return to play?
Explanation
Question 7
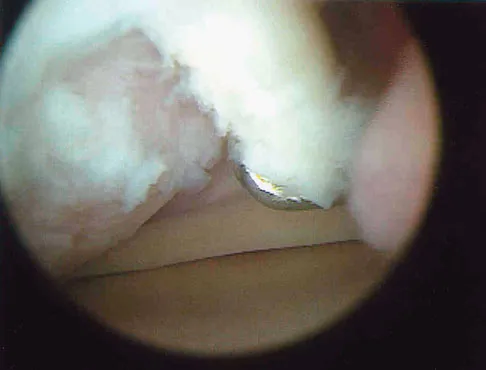
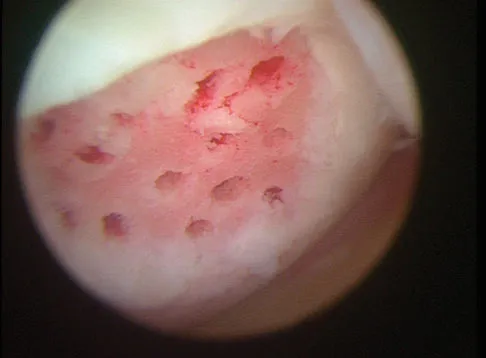
A 30-year-old patient reports chronic medial knee pain and swelling. Figure 9a shows an articular cartilage lesion observed during arthroscopy. The surgeon decides to treat the lesion with the microfracture technique seen in Figure 9b. A biopsy of the repaired tissue 1 year after treatment is likely to show which of the following findings?
Explanation
Question 8
A 24-year-old dancer reports posterior ankle pain when in the "en pointe" position. Examination reveals posteromedial tenderness, no pain reproduction with passive forced planter flexion, and pain with motion of the hallux. What is the most likely diagnosis?
Explanation
Question 9
Kinematic analysis of the medial and lateral menisci has demonstrated that the lateral meniscus has which of the following characteristics compared with the medial meniscus?
Explanation
Question 10
A 24-year-old professional basketball player reports the gradual onset of pain that is poorly localized to the left midfoot for the past 2 months. Examination reveals diffuse tenderness to palpation, full range of motion of the ankle and subtalar joint, and a normal neurovascular examination to the foot. An AP radiograph is shown in Figure 10. Definitive treatment should include
Explanation
Question 11
A 19-year-old college football player reports persistent weakness, tingling, and numbness of both upper extremities at half time. He states that these symptoms initially occurred after tackling an opposing player with his head early in the game. History reveals that he has had "burners" in the past that typically resolved within 15 to 30 minutes. Examination reveals pain-free cervical motion, weakness to shoulder abduction testing bilaterally, normal upper extremity reflexes, and decreased sensation over both shoulders and the upper arms. Appropriate initial management should consist of
Explanation
Question 12
Which of the following is the most relevant clinical factor in the maturation assessment of an adolescent female athlete contemplating anterior cruciate ligament (ACL) reconstruction?
Explanation
Question 13
A 28-year-old woman fell on her right wrist while rollerblading 2 days ago. She was seen in the emergency department at the time of injury and was told she had a sprain. Examination now reveals dorsal tenderness in the proximal wrist but no snuffbox or ulnar tenderness. Standard wrist radiographs are normal. What is the next most appropriate step in management?
Explanation
Question 14
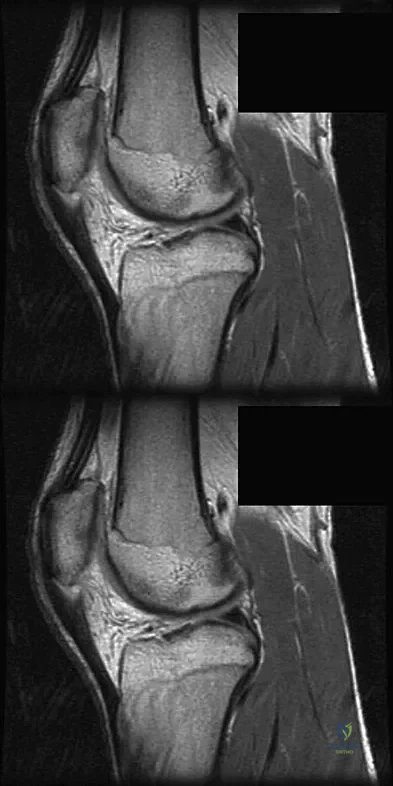
A 17-year-old basketball player and pole vaulter who has had anterior knee pain for the past 18 months now reports a recent inability to jump. Based on the MRI scan shown in Figure 11, management should consist of
Explanation
Question 15
Figures 12a through 12c show the radiographs of a 28-year-old professional baseball player who has ulnar-sided wrist pain and numbness and tingling in the fourth and fifth digits for the past 6 weeks. Management should consist of
Explanation
Question 16
Figure 13 shows the radiographs of a 20-year-old intercollegiate basketball player who was injured 6 weeks prior to the start of the season. What is the most appropriate treatment?
Explanation
Question 17
A 12-year-old boy reports the acute onset of pain and a pop over the right side of his pelvis while swinging a baseball bat during a Little League game. Radiographs reveal an avulsion of the anterior superior iliac spine with 2 cm of displacement. Management should consist of
Explanation
Question 18
Which of the following best describes heat stroke?
Explanation
Question 19
Which of the following factors is most critical to the success of a meniscal allograft transplantation?
Explanation
Question 20
What is the most common behavioral effect of anabolic steroid use in athletes?
Explanation
Question 21
What is the effect on knee kinematics following placement of an anterior cruciate ligament (ACL) graft at the 12 o'clock position?
Explanation
Question 22
The superior glenohumeral ligament primarily restrains
Explanation
Question 23
Which of the following best describes carbohydrate loading?
Explanation
Question 24
A 29-year-old quarterback falls onto his dominant shoulder and sustains the injury shown in Figures 14a and 14b. Management should consist of
Explanation
Question 25
A 27-year-old professional baseball pitcher who underwent arthroscopic olecranon debridement continues to have medial-sided elbow pain during late cocking. Physical examination reveals laxity and pain with valgus stress testing. What is the most likely cause of his pain?
Explanation
Question 26
A 12-year-old male with open physes sustains an ACL tear. Which surgical technique minimizes the risk of significant growth arrest?
Explanation
Question 27
A 20-year-old collegiate rugby player presents with recurrent anterior shoulder instability. A 3D CT scan reveals 25% anterior glenoid bone loss. What is the most appropriate surgical management?
Explanation
Question 28
The primary static stabilizer to varus opening of the knee at 30 degrees of flexion is the:
Explanation
Question 29
A 24-year-old hockey player sustains an external rotation injury to his ankle.
Radiographs demonstrate widening of the medial clear space. Which ligament is primarily ruptured first in this syndesmotic injury sequence?
Explanation
Question 30
A 32-year-old recreational volleyball player is diagnosed with a Type II SLAP tear. What differentiates a Type II from a Type I SLAP tear?
Explanation
Question 31
A 50-year-old woman feels a pop in her knee while squatting. MRI shows a medial meniscus posterior root tear and 4 mm of meniscal extrusion. Which of the following best describes the biomechanical consequence of this injury?
Explanation
Question 32
A 28-year-old male volleyball player presents with painless weakness in external rotation of his right shoulder. MRI reveals a paralabral cyst in the spinoglenoid notch. Which muscle is predominantly affected?
Explanation
Question 33
Compared to operative repair, functional bracing and early weight-bearing (non-operative management) of acute Achilles tendon ruptures in recreational athletes has been shown to result in:
Explanation
Question 34
During reconstruction of the medial patellofemoral ligament (MPFL), where is the anatomic femoral attachment (Schöttle's point) located?
Explanation
Question 35
A 25-year-old cyclist falls directly onto his shoulder. Radiographs show a 150% superior displacement of the clavicle relative to the acromion. This injury represents a complete tear of which of the following?
Explanation
Question 36
What is the most common location for an osteochondritis dissecans (OCD) lesion in the knee?
Explanation
Question 37
A 22-year-old collegiate baseball pitcher presents with vague posterior shoulder pain. Physical exam reveals a 25-degree loss of internal rotation (GIRD) compared to the contralateral side. This deficit is most commonly attributed to contracture of the:
Explanation
Question 38
A 29-year-old downhill skier catches an edge, forcibly dorsiflexing her ankle while the peroneals are contracted. She reports lateral ankle pain and a snapping sensation. Disruption of which structure is the primary cause of her pathology?
Explanation
Question 39
A 30-year-old male sustains a knee dislocation resulting in an acute Grade III MCL tear and a complete ACL rupture. What is the generally recommended initial management for the MCL injury?
Explanation
Question 40
A 26-year-old weightlifter feels a tearing sensation in his anterior chest while performing a heavy bench press.
Examination reveals loss of the anterior axillary fold. Where does the pectoralis major tendon most commonly rupture in this demographic?

Explanation
Question 41
A 21-year-old football lineman sustains an axial load to a plantarflexed foot. Radiographs demonstrate a 3mm diastasis between the base of the first and second metatarsals. What is the most appropriate treatment for this athlete?
Explanation
Question 42
A 24-year-old passenger sustains a dashboard injury in a motor vehicle collision.
Examination reveals a positive posterior drawer test. At what angle of knee flexion is the posterior cruciate ligament (PCL) the primary restraint to posterior tibial translation?
Explanation
Question 43
During a routine arthroscopic rotator cuff repair, a patient is noted to have an isolated, complete rupture of the subscapularis tendon. Which physical examination test would have been most definitively positive preoperatively?
Explanation
Question 44
A 22-year-old collegiate baseball pitcher reports deep shoulder pain during the late-cocking phase of throwing. He demonstrates a positive O'Brien test and a positive pronated load test. What is the most likely pathophysiologic mechanism of this injury?
Explanation
Question 45
A 17-year-old female soccer player sustains a noncontact deceleration injury to her knee, accompanied by a 'pop'.
Which of the following is an established intrinsic skeletal risk factor for this specific ligamentous injury?
Explanation
Question 46
A 26-year-old hockey player sustains an external rotation injury to his right ankle. Which of the following radiographic findings is the most reliable indicator of syndesmotic instability requiring operative intervention?
Explanation
Question 47
A 28-year-old professional tennis player presents with right shoulder pain. Physical examination reveals a glenohumeral internal rotation deficit (GIRD) of 25 degrees compared to the contralateral side, alongside normal overall arc of motion. What is the most appropriate initial treatment?
Explanation
Question 48
A 30-year-old male presents with knee pain after a dashboard injury. Physical examination reveals increased external tibial rotation of 15 degrees at 30 degrees of knee flexion, but symmetric external rotation at 90 degrees compared to the normal knee. Which structure is most likely injured?
Explanation
Question 49
A 45-year-old weightlifter feels a sudden tear in his chest while performing a heavy bench press. Examination reveals loss of the anterior axillary fold and weakness with internal rotation. The ruptured tendon typically inserts into which of the following anatomic locations?
Explanation
Question 50
A 25-year-old gymnast presents with recurrent lateral patellar instability. An MRI indicates a torn medial patellofemoral ligament (MPFL). During surgical reconstruction, where should the femoral tunnel be placed anatomically?
Explanation
Question 51
A 32-year-old manual laborer sustains a direct blow to the point of his shoulder. Radiographs demonstrate a 150% superior displacement of the clavicle relative to the acromion with an increased coracoclavicular distance. What is the most appropriate initial management?
Explanation
Question 52
A 50-year-old recreational runner presents with acute posteromedial knee pain after a minor squatting twisting injury. MRI demonstrates a medial meniscus posterior root tear with 4 mm of meniscal extrusion. If left untreated, this injury rapidly alters knee biomechanics to most closely resemble which of the following?
Explanation
Question 53
A 21-year-old collegiate volleyball player complains of vague, deep posterior shoulder pain.
She has normal strength with shoulder abduction, but notable weakness with external rotation when the arm is positioned at the side. At which anatomic site is the affected nerve most likely compressed?
Explanation
Question 54
A 19-year-old basketball player 'rolls' his ankle. MRI reveals an osteochondral lesion on the posteromedial aspect of the talar dome. What is the most common mechanism for this specific lesion?
Explanation
Question 55
A 28-year-old professional skier sustains a multi-ligamentous knee injury.
During surgical reconstruction of the posterolateral corner (PLC), an anatomic reconstruction technique is chosen. Which three primary structures must be addressed to restore stability to the PLC?
Explanation
Question 56
Improper tunnel placement is a frequent cause of anterior cruciate ligament (ACL) reconstruction failure. What is the primary kinematic consequence of placing the femoral tunnel too anteriorly?
Explanation
Question 57
A 25-year-old hockey player sustains a grade III acromioclavicular (AC) joint separation. If nonoperative management is chosen, what is the most likely long-term clinical outcome compared to early operative fixation?
Explanation
Question 58
A 22-year-old collegiate football player sustains a twisting ankle injury. Which physical examination finding has the highest specificity for diagnosing a syndesmotic (high ankle) sprain?
Explanation
Question 59
A 45-year-old active male presents with acute posterior knee pain and a palpable 'pop' while deep squatting. MRI reveals a complete medial meniscus posterior root tear. Left untreated, the biomechanical consequences of this injury are most equivalent to which of the following?
Explanation
Question 60
A 20-year-old rugby player presents with recurrent anterior shoulder instability. A 3D CT scan demonstrates 25% glenoid bone loss. Which surgical procedure is most indicated?
Explanation
Question 61
Historically, what is the primary biomechanical and clinical advantage of operative repair for acute Achilles tendon ruptures when compared to traditional cast immobilization?
Explanation
Question 62
A 28-year-old is involved in a motor vehicle collision and sustains a dashboard injury. Examination and MRI confirm an isolated Grade II Posterior Cruciate Ligament (PCL) tear. What is the recommended initial management?
Explanation
Question 63
A 24-year-old elite baseball pitcher presents with vague, deep shoulder pain during the late cocking phase of throwing. MRI confirms an isolated Type II SLAP tear. After confirming a glenohumeral internal rotation deficit (GIRD), what is the most appropriate initial management?
Explanation
Question 64
A 19-year-old gymnast presents with persistent medial ankle pain after an inversion injury 6 months ago. MRI reveals a 12 mm osteochondral lesion of the medial talar dome with intact overlying cartilage. If a 3-month trial of immobilization and non-weight bearing fails, what is the best initial surgical treatment?
Explanation
Question 65
The medial patellofemoral ligament (MPFL) provides the primary soft-tissue restraint to lateral patellar translation at which range of knee flexion?
Explanation
Question 66
A 30-year-old competitive powerlifter feels a sharp pop in his chest while attempting a heavy bench press. Exam reveals loss of the anterior axillary fold and weakness in internal rotation.
Where does the pectoralis major most commonly rupture in this scenario?
Explanation
Question 67
A 25-year-old alpine skier sustains a forced dorsiflexion and eversion injury to the ankle. She reports a painful snapping sensation over the lateral malleolus. Which anatomic structure is most likely compromised?
Explanation
Question 68
A 14-year-old boy presents with anterior knee pain and catching. Imaging shows an osteochondritis dissecans (OCD) lesion of the lateral aspect of the medial femoral condyle. MRI indicates fluid tracking behind the lesion, suggesting instability. His physes remain open. What is the most appropriate management?
Explanation
Question 69
An elite overhead throwing athlete presents with posterior shoulder pain during the late cocking phase. Which combination of intra-articular pathology is most characteristic of internal impingement?
Explanation
Question 70
A rugby player is tackled with a blow to the anteromedial tibia. Exam reveals increased varus laxity at 30 degrees of knee flexion but normal varus stability at 0 degrees. The dial test shows increased external rotation at 30 degrees, but it is symmetric to the contralateral side at 90 degrees. Which structures are most likely injured?
Explanation
Question 71
A 65-year-old male with a history of chronic shoulder aching feels a sudden pop with subsequent ecchymosis in his upper arm, creating a 'Popeye' deformity. He notes that his shoulder pain has actually improved since the event. What is the most appropriate treatment?
Explanation
Question 72
During a modified Broström-Gould procedure for chronic lateral ankle instability, adjacent tissue is mobilized and sutured to the distal fibula to augment the repair of the anterior talofibular and calcaneofibular ligaments. Which specific structure is utilized for this augmentation?
Explanation
Question 73
A 27-year-old male presents to the ER following a traumatic knee dislocation during a football game. The knee spontaneously reduced prior to arrival. An ankle-brachial index (ABI) is calculated to be 0.8. What is the next most appropriate step in management?
Explanation
Question 74
A 26-year-old professional volleyball player complains of vague posterior shoulder pain and profound weakness in external rotation.
MRI reveals a paralabral cyst in the spinoglenoid notch. Which muscle would exhibit isolated weakness on clinical exam?
Explanation
Question 75
A 21-year-old female presents with recurrent lateral patellar dislocations. An axial CT scan measures a tibial tubercle-trochlear groove (TT-TG) distance of 24 mm. Which procedure should be included in her definitive surgical plan to correct this specific pathomechanics?
Explanation
Question 76
A 17-year-old female high school soccer player is scheduled to undergo an anterior cruciate ligament (ACL) reconstruction. When discussing graft choices, which of the following is associated with the highest rate of clinical failure and need for revision in this specific patient demographic?
Explanation
Question 77
A 22-year-old competitive rugby player presents with recurrent anterior shoulder instability. Radiographs and a 3D CT scan demonstrate 25% anterior glenoid bone loss and an engaging Hill-Sachs lesion. What is the most appropriate definitive surgical management?
Explanation
Question 78
Recent meta-analyses comparing operative versus non-operative management of acute Achilles tendon ruptures utilizing modern functional rehabilitation protocols demonstrate that operative management is associated with:
Explanation
Question 79
A 55-year-old female sustains an acute posterior root tear of the medial meniscus. Biomechanically, if left untreated, this injury most closely approximates the tibiofemoral contact pressures seen in which of the following scenarios?
Explanation
Question 80
A 45-year-old recreational tennis player presents with persistent deep shoulder pain and mechanical catching. An MRI arthrogram reveals an isolated Type II SLAP tear. After failing 6 months of physical therapy, operative intervention is selected. Which of the following procedures is most likely to yield the highest patient satisfaction and lowest reoperation rate?
Explanation
Question 81
A 28-year-old male sustains a twisting injury to his knee. On physical examination, the Dial test reveals 20 degrees of increased external rotation of the tibia compared to the contralateral side at 30 degrees of knee flexion, but symmetric rotation is noted at 90 degrees of knee flexion. This finding is most consistent with an isolated injury to the:
Explanation
Question 82
A 24-year-old runner presents with chronic ankle pain following multiple severe ankle sprains. MRI demonstrates a wafer-shaped osteochondral lesion on the anterolateral aspect of the talar dome. Based on typical injury mechanics, this specific lesion is most likely the result of which mechanism?
Explanation
Question 83
A 20-year-old collegiate baseball pitcher complains of posterior shoulder pain during the late cocking phase of throwing. Examination demonstrates a 25-degree glenohumeral internal rotation deficit (GIRD) compared to the contralateral shoulder. The pathophysiology of internal impingement in this athlete most likely involves abnormal contact between the posterosuperior labrum and the:
Explanation
Question 84
A 32-year-old male sustains a high-energy knee dislocation. After closed reduction in the emergency department, his pedal pulses are symmetric and capillary refill is brisk. The Ankle-Brachial Index (ABI) is measured at 0.85. What is the most appropriate next step in management?
Explanation
Question 85
A 26-year-old male presents with persistent anterior knee pain. Imaging and diagnostic arthroscopy confirm an isolated 3.5 cm^2 symptomatic, full-thickness chondral defect on the medial femoral condyle. He has failed non-operative management. Which of the following cartilage restoration procedures is most appropriate for a lesion of this size?
Explanation
Question 86
A 25-year-old professional hockey player sustains a direct downward blow to the point of his right shoulder. Radiographs confirm a Type III acromioclavicular (AC) joint separation (complete disruption of AC and CC ligaments with 100% displacement). According to current literature, what is the most widely accepted initial management for this injury?
Explanation
Question 87
A 22-year-old soccer player sustains an acute knee injury. During physical examination, a positive pivot shift test is elicited. Which of the following structures is primarily responsible for the reduction of the lateral tibial plateau during the flexion phase of this clinical test?
Explanation
Question 88
A 24-year-old professional baseball pitcher complains of posterior shoulder pain during the late cocking phase of throwing. MRI arthrography reveals a partial-thickness articular-sided tear of the supraspinatus and posterosuperior labral fraying. What is the most likely pathomechanical cause of this condition?
Explanation
Question 89
A 21-year-old collegiate football player sustains an external rotation injury to his right ankle. Weight-bearing radiographs show no fracture, a tibiofibular clear space of 4 mm, and a normal medial clear space. An MRI demonstrates an isolated tear of the anterior inferior tibiofibular ligament (AITFL). What is the most appropriate management?
Explanation
Question 90
During a knee arthroscopy, a 30-year-old patient is noted to have a 1.5 cm longitudinal tear in the peripheral red-red zone of the medial meniscus. Which of the following factors most significantly enhances the expected healing rate of a meniscal repair in this patient?
Explanation
Question 91
A 19-year-old competitive rugby player presents with recurrent anterior shoulder instability. A 3D CT scan demonstrates 22% anterior glenoid bone loss and a non-engaging Hill-Sachs lesion. Which of the following is the most appropriate surgical intervention?
Explanation
Question 92
A 45-year-old recreational tennis player suffers an acute Achilles tendon rupture and elects to proceed with nonoperative management utilizing an early functional rehabilitation protocol. Compared to operative management, which of the following is true regarding his chosen treatment?
Explanation
Question 93
A 28-year-old motorcyclist sustains a dashboard injury to his knee. The dial test demonstrates 15 degrees of increased external rotation of the tibia compared to the contralateral side at 90 degrees of knee flexion, but symmetrical external rotation at 30 degrees. Which structure is most likely injured?
Explanation
Question 94
A 25-year-old cyclist falls directly onto his right shoulder. Radiographs demonstrate 150% superior displacement of the clavicle relative to the acromion, with significant widening of the coracoclavicular distance. The clavicle is not posteriorly displaced into the trapezius. According to the Rockwood classification, what type of injury is this, and what is the typical management?
Explanation
Question 95
A 32-year-old female sustains a knee dislocation (Schenck KD III) after a skiing collision. The knee is reduced in the emergency department. Her pedal pulses are palpable, but her Ankle-Brachial Index (ABI) is calculated to be 0.85. What is the most appropriate next step in management?
Explanation
Question 96
A 42-year-old manual laborer presents with anterior shoulder pain and mechanical catching. MRI reveals an isolated Type II SLAP tear. After 6 months of failed conservative management, he is scheduled for surgery. Based on current literature, what is the most appropriate surgical procedure for this patient?
Explanation
Question 97
A 24-year-old gymnast complains of persistent anterolateral ankle pain. MRI demonstrates a 1.2 cm x 1.0 cm osteochondral lesion of the anterolateral talar dome. She has failed 4 months of conservative therapy. What is the most appropriate initial surgical intervention?
Explanation
Question 98
During a medial patellofemoral ligament (MPFL) reconstruction for recurrent patellar instability, the femoral tunnel must be placed accurately to avoid altering graft kinematics. Which of the following describes the correct radiographic landmark (Schöttle's point) for the femoral origin of the MPFL?
Explanation
Question 99
A 30-year-old bodybuilder feels a sudden "pop" in his anterior shoulder while performing a heavy bench press. Examination shows loss of the normal anterior axillary fold and weakness in internal rotation. MRI confirms a complete rupture of the pectoralis major. At which specific anatomical location do the majority of these ruptures occur?
Explanation
Question 100
A 28-year-old marathon runner presents with lateral knee pain that worsens after 3 miles of running. Pain is localized to the lateral femoral epicondyle and is exacerbated when transitioning from flexion to extension at approximately 30 degrees. What is the primary pathophysiological mechanism of her condition?
Explanation
None
