AAOS Upper Extremity MCQs (Set 5): Shoulder, Elbow & Wrist Injuries | ABOS Review
Key Takeaway
This high-yield question set (Set 5) for the AAOS, ABOS, and OITE exams focuses on comprehensive upper extremity orthopedics. Topics include shoulder pathology, rotator cuff injuries, elbow fractures, ligamentous trauma, and common wrist & hand conditions, preparing you for board success.
AAOS Upper Extremity MCQs (Set 5): Shoulder, Elbow & Wrist Injuries | ABOS Review
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 38-year-old woman with diabetes mellitus reports a 6-week history of fever and pain localized to the right sternoclavicular joint. Local signs on examination include swelling about the joint, erythema, and increased warmth. Initial aspiration of the joint reveals Staphylococcus aureus. Radiographs reveal medial clavicular osteolysis. What is the most effective treatment at this time?
Explanation
Question 2
A patient has a humeral shaft fracture and is scheduled to undergo open reduction and internal fixation with a plate. What surgical approach will provide the greatest amount of exposure?
Explanation
Question 3
A 67-year-old woman is seen in the emergency department after falling at home. Radiographs before and after treatment are shown in Figures 49a and 49b, respectively. Which of the following best explains the 8-week postinjury clinical findings seen in Figure 49c?
Explanation
Question 4
What is the most common complaint in patients with a developmental radial head dislocation?
Explanation
Question 5
Which of the following has been associated with a decreased rate of glenoid component radiolucent lines?
Explanation
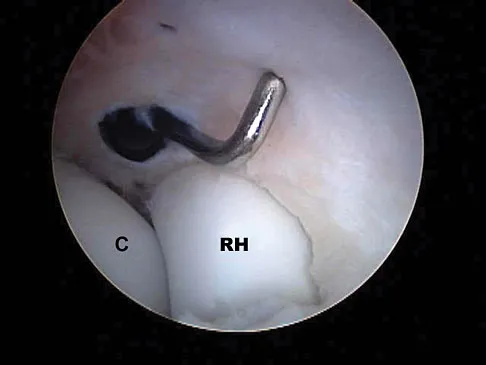
Question 6
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50?
Explanation
Question 7
Figure 51 shows the radiograph of a 42-year-old construction worker who has pain and limited motion in his dominant elbow. Management consisting of nonsteroidal anti-inflammatory drugs and cortisone has failed to provide relief. What is the next most appropriate step in treatment?
Explanation
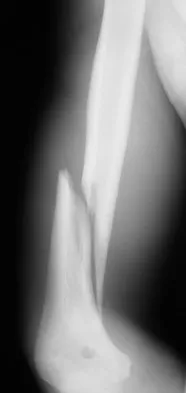
Question 8
A 35-year-old man sustained the closed injury shown in Figure 52 in his dominant extremity. Neurologic function is normal. Treatment should consist of
Explanation
Question 9
A 74-year-old man has had worsening left shoulder pain for the past 3 years. Extensive nonsurgical management has provided only minimal relief. Examination reveals limitations in motion due to pain but good rotator cuff strength. Radiographs are shown in Figures 53a and 53b. What surgical procedure is most appropriate?
Explanation
Question 10
The radiograph shown in Figure 54 reveals that the plate on the second metacarpal is acting in what manner?
Explanation
Question 11
Which of the following antibiotics is contraindicated in children?
Explanation
Question 12
Which of the following conditions is considered a relative contraindication to interscalene nerve block for patients scheduled to undergo shoulder surgery?
Explanation
Question 13
Figure 55 shows the radiograph of a 30-year-old man who sustained a closed comminuted fracture of the right clavicle. Examination reveals decreased sensation in the radial nerve distribution. Weakness is noted with shoulder abduction, internal rotation, and wrist extension. A displaced bone fragment is most likely pressing on what portion of the brachial plexus?
Explanation
Question 14
Which of the following characteristics is seen in patients with osteochondritis dissecans of the elbow?
Explanation
Question 15
Which of the following is considered an important component in treating the lesion shown in Figure 56?
Explanation
Question 16
A 22-year-old female collegiate javelin thrower has shoulder pain. She notes that her pain is primarily located in the posterior aspect of her shoulder, is exacerbated with throwing, and she experiences maximal tenderness in the extreme cocking phase of the throwing cycle. On examination, she reports deep posterior shoulder pain when the arm is abducted 90 degrees and maximally externally rotated to 110 degrees. This reproduces her symptoms precisely. Shoulder radiographs are normal. What is the most likely diagnosis?
Explanation
Question 17
A patient with rheumatoid arthritis has a rupture of the extensor digitorum communis to 4 and 5. You are planning to perform an extensor indicis proprius (EIP) tendon transfer. What effect will this have on index finger extension?
Explanation
Question 18
What is the most common complication following interscalene nerve block for shoulder surgery?
Explanation
Question 19
A 61-year-old woman with a long-standing history of rheumatoid arthritis reports progressive elbow pain for the past 12 months. She denies any recent trauma to the elbow; however, she notes increasing pain and decreased joint motion that are now compromising her function. Radiographs are shown in Figures 57a and 57b. What is the most appropriate treatment at this time?
Explanation
Question 20
What neurovascular structure is at greatest risk when creating a proximal anterolateral elbow arthroscopy portal?
Explanation
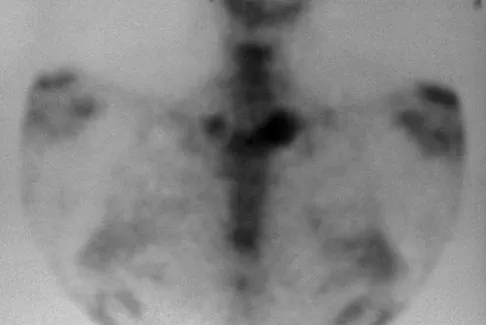
Question 21
A 52-year-old woman reports mild pain localized to the left sternoclavicular joint. History is notable for chronic renal failure requiring dialysis for the last 5 years. A clinical photograph, chest radiograph, and bone scan are shown in Figures 58a through 58c. What is the most likely diagnosis?
Explanation
Question 22
A 22-year-old college quarterback is tackled and sustains a reducible first carpometacarpal dislocation. What is the recommended treatment?
Explanation
Question 23
What is the most important stabilizing mechanism in the midrange of motion of the glenohumeral joint?
Explanation
Question 24
In a locking plate screw construct, axial forces are borne by which of the following?
Explanation
Question 25
What structure provides the most static stability for valgus restraint in the elbow?
Explanation
Question 26
A 45-year-old male falls from a ladder and sustains a complex elbow injury. Radiographs reveal a posterior elbow dislocation, a comminuted radial head fracture, and a Type II coronoid fracture. Operative intervention is planned. What is the recommended sequence of surgical reconstruction to restore elbow stability?
Explanation
Question 27
A 65-year-old active female sustains a distal radius fracture after a fall on an outstretched hand. Which of the following initial radiographic parameters is the most reliable predictor that nonoperative management in a cast will fail and result in unacceptable deformity?
Explanation
Question 28
A 22-year-old male sustains an acute proximal pole scaphoid fracture. Operative fixation is planned to minimize the risk of nonunion. Which surgical approach and screw trajectory provide the best biomechanical fixation and biological preservation of the proximal pole?
Explanation
Question 29
A 32-year-old male with a history of seizure disorder presents to the emergency department with severe shoulder pain and an inability to externally rotate his arm. An anteroposterior (AP) radiograph demonstrates a symmetrically rounded appearance of the humeral head. What is the most likely diagnosis?
Explanation
Question 30
A 19-year-old cyclist sustains a midshaft clavicle fracture after being thrown over the handlebars. Which of the following findings represents an absolute indication for open reduction and internal fixation?
Explanation
Question 31
A 7-year-old boy presents with a deformed forearm after a fall from monkey bars. Radiographs show an apex-volar angulated proximal ulnar shaft fracture and a posteriorly dislocated radial head. How is this specific injury pattern classified according to the Bado system?
Explanation
Question 32
An 18-year-old male sustains a complete distal biceps tendon rupture. He undergoes repair via a single-incision anterior approach. Which of the following nerves is most at risk of injury with this specific surgical approach?
Explanation
Question 33
A 45-year-old man falls on an outstretched hand and sustains a terrible triad injury of the elbow. What is the recommended surgical sequence for repairing these injuries?
Explanation
Question 34
A 24-year-old man presents with an open midshaft humerus fracture and an ipsilateral complete radial nerve palsy. What is the most appropriate management?
Explanation
Question 35
A 32-year-old woman falls from a height and sustains a comminuted radial head fracture, which is excised. Postoperatively, she reports persistent, severe wrist pain. Examination reveals tenderness over the distal radioulnar joint (DRUJ) and positive ulnar variance. Which of the following is the most likely diagnosis?
Explanation
Question 36
A 22-year-old man requires open reduction and internal fixation of a proximal pole scaphoid fracture. Which surgical approach provides the most direct access to the proximal pole while preserving its primary blood supply?
Explanation
Question 37
A 19-year-old collegiate rugby player with recurrent anterior shoulder instability undergoes imaging, which demonstrates a 25% anterior glenoid bone loss and an engaging Hill-Sachs lesion. Which of the following is the most appropriate surgical treatment?
Explanation
Question 38
When evaluating a displaced 4-part proximal humerus fracture, preservation of the blood supply to the humeral head is a critical concern. Which of the following arteries provides the primary blood supply to the articular segment of the humeral head?
Explanation
Question 39
A 45-year-old manual laborer presents with progressive wrist pain and a history of remote trauma. Radiographs demonstrate degenerative changes between the radial styloid and the scaphoid, as well as between the scaphoid and the entire scaphoid fossa of the radius. The radiolunate joint is spared. What is the correct SLAC wrist stage?
Explanation
Question 40
A 60-year-old woman undergoes volar locked plating for a distal radius fracture. Three months postoperatively, she returns with sudden inability to actively extend her thumb. What is the most likely cause of this complication?
Explanation
Question 41
A 32-year-old male weightlifter feels a pop in his anterior chest while performing a heavy bench press. Examination reveals an asymmetric chest wall and weakness with internal rotation. MRI confirms a complete tear of the pectoralis major tendon at its insertion. What is the recommended management?
Explanation
Question 42
A 7-year-old boy falls on an outstretched arm and sustains a Bado Type I Monteggia fracture-dislocation. What is the defining characteristic of this injury?
Explanation
Question 43
A 45-year-old man sustains a terrible triad injury of the elbow consisting of an elbow dislocation, radial head fracture, and coronoid fracture. What is the generally recommended surgical sequence of reconstruction?
Explanation
Question 44
A 62-year-old woman presents with the inability to flex her thumb interphalangeal joint 9 months after volar plate fixation of a distal radius fracture.
What is the most likely cause of her current symptoms?

Explanation
Question 45
Which of the following radiographic features is the most reliable predictor of ischemia and subsequent avascular necrosis of the humeral head following a proximal humerus fracture?

Explanation
Question 46
A 35-year-old man undergoes surgical repair of a distal biceps tendon rupture via a single-incision anterior approach. Postoperatively, he notes numbness over the lateral aspect of his forearm. Which nerve was most likely injured during the procedure?

Explanation
Question 47
A 22-year-old man presents with chronic wrist pain and is diagnosed with a scaphoid waist nonunion demonstrating a humpback deformity and no evidence of avascular necrosis. What is the most appropriate surgical treatment?
Explanation
Question 48
A 28-year-old man sustains a closed spiral fracture of the distal third of the humeral shaft (Holstein-Lewis fracture). On initial evaluation, he has a complete radial nerve palsy. What is the most appropriate initial management?
Explanation
Question 49
A 20-year-old football player presents with recurrent anterior shoulder instability. Advanced imaging demonstrates a 15% glenoid bone loss combined with a large, engaging Hill-Sachs lesion. Which of the following surgical procedures is most appropriate?

Explanation
Question 50
A 45-year-old woman falls on an outstretched hand and sustains a comminuted radial head fracture. Three weeks after isolated radial head excision, she develops progressive, severe wrist pain and prominence of the ulnar head. What is the underlying pathology?
Explanation
Question 51
A 30-year-old construction worker falls from a height. Radiographs reveal a dorsal perilunate dislocation. The patient urgently complains of severe numbness and tingling in the thumb, index, and middle fingers. Which nerve is most likely affected by this injury pattern?

Explanation
Question 52
A 45-year-old man sustains a terrible triad injury to his elbow. During surgical reconstruction, what is the recommended sequence of repair to restore elbow stability?
Explanation
Question 53
According to Hertel's criteria, which combination of radiographic findings is the most highly predictive of humeral head ischemia following a proximal humerus fracture?
Explanation
Question 54
A 25-year-old man falls on an outstretched hand and sustains a fracture of the scaphoid proximal pole. What is the primary anatomical reason this specific fracture pattern is at a high risk for avascular necrosis?
Explanation
Question 55
A 65-year-old woman undergoes volar plate fixation for a displaced distal radius fracture. Six months later, she presents with an inability to actively flex her thumb interphalangeal joint. What surgical error is most likely responsible for this complication?
Explanation
Question 56
A 30-year-old elite volleyball player complains of vague posterior shoulder pain and isolated weakness in external rotation. An MRI reveals a paralabral ganglion cyst. At what precise anatomic location is this cyst most likely compressing the affected nerve?
Explanation
Question 57
In Scapholunate Advanced Collapse (SLAC) of the wrist, which articular surface is typically spared from degenerative changes even in advanced stages (Stage III)?
Explanation
Question 58
A 45-year-old man falls on his outstretched hand and sustains a terrible triad injury of the elbow.
During the standard lateral surgical approach, which of the following structures is typically repaired last to restore elbow stability?
Explanation
Question 59
A 35-year-old male construction worker presents with chronic wrist pain and a known history of a scaphoid nonunion. Radiographs demonstrate advanced radiocarpal arthritis and capitolunate arthritis, but the radiolunate joint is completely spared. What is the most appropriate motion-preserving surgical procedure?
Explanation
Question 60
A 60-year-old man presents with chronic shoulder pain and weakness. On examination, he is unable to actively externally rotate his arm while it is held in 90 degrees of abduction (positive Hornblower's sign). This clinical finding indicates a deficiency in a muscle innervated by which of the following nerves?
Explanation
Question 61
A 22-year-old rugby player undergoes an open Latarjet procedure for recurrent anterior shoulder instability. Postoperatively, he presents with weakness in elbow flexion and forearm supination, as well as numbness over the lateral forearm. Which nerve was most likely injured during the procedure?
Explanation
Question 62
A 30-year-old woman falls on an outstretched hand and sustains a coronal shear fracture of the capitellum that extends into the lateral trochlear ridge (McKee modification of Bryan and Morrey Type IV). Which surgical approach provides the most optimal visualization for fixation of this specific injury?
Explanation
Question 63
A 55-year-old woman underwent volar locked plating of a distal radius fracture 6 months ago. She now presents with a sudden inability to actively flex the interphalangeal joint of her thumb. What is the most likely cause of this complication?
Explanation
Question 64
A 70-year-old woman sustains a highly displaced 4-part proximal humerus fracture.
According to Hertel's radiographic criteria, which of the following findings is the most reliable predictor of humeral head ischemia?
Explanation
Question 65
Which of the following is the most reliable radiographic predictor of humeral head ischemia following a proximal humerus fracture?
Explanation
Question 66
A 42-year-old man falls on an outstretched hand and sustains a "terrible triad" injury to his elbow. During surgical reconstruction, what is the recommended sequence of repair to restore elbow stability?
Explanation
Question 67
A 55-year-old woman undergoes volar locked plating for a distal radius fracture. Six months postoperatively, she is unable to actively flex the interphalangeal joint of her thumb. Which of the following technical errors most likely contributed to this complication?
Explanation
Question 68
A 32-year-old man presents with chronic wrist pain. Radiographs reveal a scaphoid nonunion with radioscaphoid arthritis, but preservation of the midcarpal and radiolunate joints. Which of the following is the most appropriate surgical treatment?
Explanation
Question 69
A 22-year-old competitive rugby player with recurrent anterior shoulder instability is found to have 25% anterior glenoid bone loss on a 3D CT scan. Which of the following is the most appropriate surgical intervention?
Explanation
Question 70
A 35-year-old woman sustains a displaced type I (Hahn-Steinthal) capitellum fracture. What is the most appropriate management?
Explanation
Question 71
A 40-year-old man sustains a highly comminuted radial head fracture, an interosseous membrane disruption, and a DRUJ dislocation. What is the most appropriate management strategy?
Explanation
Question 72
A 19-year-old male presents to the emergency department with dyspnea, dysphagia, and severe pain after a rugby tackle. Exam reveals a depression at the medial end of the clavicle. What is the most important next step in management?
Explanation
Question 73
A 45-year-old male laborer experiences a sudden "pop" in his anterior elbow while lifting a heavy box. On exam, the hook test is positive. Which of the following is true regarding nonoperative versus operative management of this injury?
Explanation
None
