Upper Extremity Orthopedic MCQs (Set 1): Shoulder, Elbow, Hand & Wrist | AAOS/ABOS Exam Prep

Key Takeaway
This high-yield question set for the AAOS/ABOS exams covers critical upper extremity orthopedic topics. It includes multiple-choice questions on shoulder pathologies, elbow injuries, and various hand & wrist conditions, preparing candidates for board certification and OITE success.
Upper Extremity Orthopedic MCQs (Set 1): Shoulder, Elbow, Hand & Wrist | AAOS/ABOS Exam Prep
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
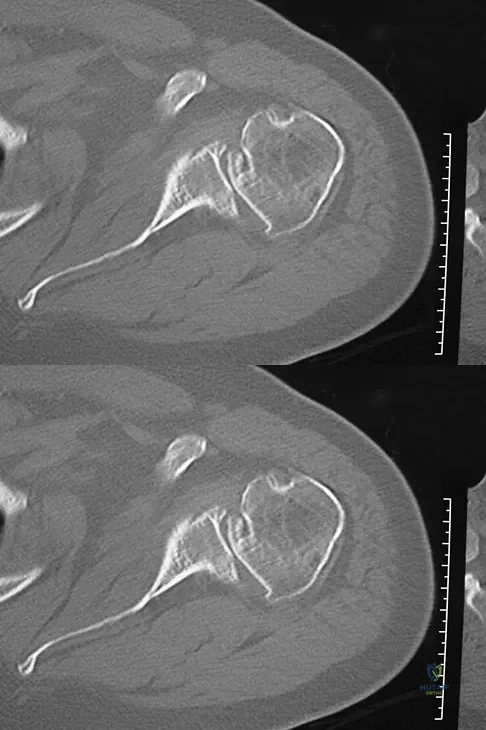
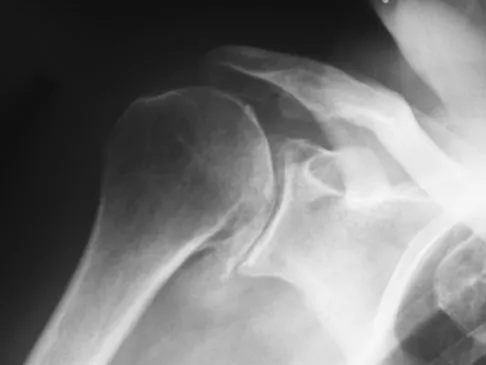
A 68-year-old man had a 3-year history of shoulder pain that failed to respond to nonsurgical management. Examination reveals forward elevation to 120 degrees and external rotation to 30 degrees. True AP and axillary radiographs and an axial CT scan are shown in Figures 1a through 1c. What management option would lead to the best long-term results?
Explanation
Question 2
A 66-year-old woman who previously underwent hemiarthroplasty 2 years ago for a fracture continues to have severe pain and loss of motion despite undergoing physical therapy. A radiograph is shown in Figure 2. What is the most likely reason that this patient has failed to improve her motion?
Explanation
Question 3
Baseball pitchers who have internal impingement will most likely demonstrate what changes in range of motion?
Explanation
Question 4
A 40-year-old woman underwent an arthroscopic acromioplasty and mini-open rotator cuff repair 4 weeks ago. At follow-up examination, the incision is painful, erythematous, and draining fluid. The patient is febrile and has an elevated WBC count. What infectious organism should be under high suspicion of causing this outcome?
Explanation
Question 5
What ligament is the primary stabilizer of the wrist following a proximal row carpectomy?
Explanation
Question 6
A 30-year-old right hand-dominant woman is seen in the trauma unit after a high-speed motor vehicle accident. She sustained a right shoulder anterior dislocation that is gently reduced under sedation. A CT scan is shown in Figure 3. If left untreated, the patient is at greatest risk for
Explanation
Question 7
Osteonecrosis of the humeral head is a rare complication seen after dislocation of the glenohumeral joint in skeletally immature patients. When this complication is encountered, treatment should consist of
Explanation
Question 8
A patient reports persistent anterior shoulder pain following a forceful external rotation injury to the shoulder. An MRI scan is shown in Figure 4. The patient remains symptomatic despite 3 months of nonsurgical management. Treatment should now consist of
Explanation
Question 9
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure 5. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion?
Explanation
Question 10
An MRI arthrogram of the elbow is shown in Figure 6. Based on these findings, what is the most likely diagnosis?
Explanation
Question 11
A 45-year-old woman awakens with the acute onset of burning left shoulder pain that radiates toward the axilla. She denies any history of trauma. On examination, she is unable to abduct her arm but has full passive shoulder motion. Her sensation is intact. Cervical spine examination reveals full range of motion and a negative Spurling's test. Radiographs and MRI studies are normal for the cervical spine and shoulder. What is the most likely diagnosis?
Explanation
Question 12
A 25-year-old woman returns for her first postoperative visit after arthroscopic thermal capsulorrhaphy for recurrent multidirectional instability. Examination reveals that the portals are healed, there is no swelling; and passive range of motion is within the normal range. However, she is unable to actively raise her arm. Shoulder radiographs are normal. What is the most likely cause of these findings?
Explanation
Question 13
Figure 7 shows a sagittal T1-weighted MRI scan. What muscle/tendon is identified by the arrow?
Explanation
Question 14
A 72-year-old man who underwent total shoulder arthroplasty 2 years ago slipped on ice and fell on his shoulder 3 weeks ago. Immediately after falling he was unable to elevate his arm. Motor examination reveals deltoid 5-/5, subscapularis 5-/5, external rotation 4-/5, and supraspinatus 2/5. Radiographs are shown in Figures 8a and 8b. What is the most likely diagnosis?
Explanation
Question 15
A 39-year-old man has had persistent right shoulder pain for the past 6 months. A formal physical therapy program has failed to provide relief, and an injection several months ago provided only short-term relief. Examination reveals a positive Neer and Hawkins test. There is no instability and the neurovascular examination is normal. Arthroscopy reveals a partial rotator cuff tear on the bursal side measuring 60% of the tendon thickness. What is the next most appropriate step in management?
Explanation
Question 16
The condition shown in Figures 9a and 9b is most likely the result of
Explanation
Question 17
A patient reports hyperesthesia over the base of the thenar eminence following volar locked plating of a distal radius fracture. A standard volar approach of Henry was used. What is the most likely cause of the hyperesthesia?
Explanation
Question 18
Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient?
Explanation
Question 19
Which of the following surgical devices employed for stabilization of the sternoclavicular joint is associated with the highest incidence of life-threatening complications?
Explanation
Question 20
Figure 11a shows the clinical photograph of a 46-year old woman who reports a 3-week history of pain and a "lump" at the base of her neck. She is otherwise in good health and denies any trauma. A 3-D reconstruction CT is shown in Figure 11b. What is the most likely diagnosis?
Explanation
Question 21
Figure 12a shows the clinical photograph of a 36-year-old man who has left shoulder pain and dysfunction after undergoing a lymph node biopsy 2 years ago. The appearance of the shoulder during abduction and a wall push-up maneuver is shown in Figures 12b and 12c, respectively. Which of the following procedures provides the best pain relief and function?
Explanation
Question 22
What is the most common cause for poor outcomes in patients who undergo total shoulder arthroplasty?
Explanation
Question 23
A 53-year-old man has had a long history of multiple joint symptoms, and he notes that the worst pain is from his left shoulder. A radiograph and MRI scan are shown in Figures 13a and 13b. Prior to surgical treatment of the shoulder, what is the most appropriate work-up?
Explanation
Question 24
A 52-year-old man underwent arthroscopic repair of a 1-cm supraspinatus tendon tear 3 weeks ago. He was doing well until he fell down three stairs. One week after the fall he continues to report pain similar to his preoperative pain. An MRI scan reveals a minimally retracted 1-cm supraspinatus tendon tear in the same location as his original tear. Management should now consist of
Explanation
Question 25
A 49-year-old woman with serologically proven rheumatoid arthritis has Larsen grade II radiographic changes in the elbow. Examination reveals a preoperative arc of flexion of less than 90 degrees and there is no instability. Nonsurgical management has failed to provide relief. What is the best treatment option?
Explanation
Question 26
A 22-year-old collegiate rugby player presents with recurrent anterior shoulder instability. An MRI reveals a 25% bony Bankart lesion of the anterior glenoid.
Which of the following surgical interventions provides the most reliable long-term stability for this patient?

Explanation
Question 27
A 72-year-old woman presents with severe shoulder pain and pseudoparalysis. Radiographs demonstrate severe glenohumeral osteoarthritis with superior migration of the humeral head articulating with the acromion.
Which of the following relies on the deltoid to restore active elevation in this setting?
Explanation
Question 28
In the surgical management of a 'terrible triad' injury of the elbow, which of the following structures is typically repaired last to ensure adequate stability?
Explanation
Question 29
A 24-year-old man sustains a proximal pole scaphoid fracture. The high risk of avascular necrosis (AVN) in this region is primarily due to which of the following anatomic characteristics?
Explanation
Question 30
A 55-year-old man presents with chronic wrist pain. Radiographs reveal Scapholunate Advanced Collapse (SLAC) Stage III, characterized by arthritis in the capitolunate joint. Which of the following articulations is typically spared in this condition?
Explanation
Question 31
A 48-year-old manual laborer sustains a Type II SLAP tear. Nonoperative management fails. What is the most appropriate surgical treatment to minimize postoperative stiffness and allow a predictable return to work?
Explanation
Question 32
When performing a Zone II flexor tendon repair, which of the following surgical techniques allows for the safest implementation of an early active motion rehabilitation protocol?
Explanation
Question 33
A 40-year-old weightlifter undergoes an anterior single-incision repair of a distal biceps tendon rupture. Postoperatively, he reports numbness over the lateral aspect of his forearm. Which nerve was most likely injured during the procedure?
Explanation
Question 34
During a carpal tunnel release, care must be taken to avoid injury to the recurrent motor branch of the median nerve. In the most common anatomical variation (extraligamentous), this branch originates:
Explanation
Question 35
In an unreduced Type III acromioclavicular (AC) joint separation, which of the following ligaments provides the primary restraint against superior translation of the clavicle?
Explanation
Question 36
A patient undergoes in situ decompression of the ulnar nerve for cubital tunnel syndrome. During the approach, the roof of the cubital tunnel is incised. What structure primarily forms the roof of this tunnel?
Explanation
Question 37
A 25-year-old gymnast complains of ulnar-sided wrist pain after a fall. Examination reveals a positive fovea sign and pain with ulnar deviation. MRI confirms a Palmer Type 1B tear of the Triangular Fibrocartilage Complex (TFCC). What is the appropriate surgical management if conservative treatment fails?
Explanation
Question 38
A 22-year-old collegiate rugby player presents with recurrent anterior shoulder instability after a primary traumatic dislocation. A 3D-CT scan reveals 25% anterior glenoid bone loss. What is the most appropriate definitive surgical management?
Explanation
Question 39
A 45-year-old manual laborer presents with chronic wrist pain. Radiographs demonstrate a scaphoid nonunion with radioscaphoid and capitolunate arthritis, but the radiolunate joint is completely preserved. What is the most appropriate surgical intervention?
Explanation
Question 40
A 35-year-old man falls on an outstretched hand, sustaining a 'terrible triad' injury of the elbow. During surgical reconstruction, what is the generally recommended sequence of repair to restore elbow stability?
Explanation
Question 41
An active 76-year-old woman sustains a highly comminuted 4-part proximal humerus fracture with a head-split component and severe osteopenia. Which surgical treatment provides the most predictable restoration of forward elevation?
Explanation
Question 42
A 28-year-old carpenter sustains a Zone II flexor tendon laceration. During repair, the surgeon chooses a 4-strand core suture technique instead of a 2-strand technique. What is the primary biomechanical advantage of this choice?
Explanation
Question 43
A 55-year-old woman undergoes volar locked plating for a comminuted distal radius fracture. Six months later, she presents unable to actively flex the interphalangeal joint of her thumb. What technical error during the initial surgery most likely caused this complication?
Explanation
Question 44
A 42-year-old bodybuilder feels a 'pop' in his anterior elbow followed by weakness in supination. He undergoes a classic two-incision distal biceps tendon repair. Which nerve is at greatest risk of injury during the posterolateral dissection of this approach?
Explanation
Question 45
A 55-year-old man presents with anterior shoulder pain following a fall. Physical examination reveals a positive lift-off test, a positive belly-press test, and passively increased external rotation compared to the contralateral side. What is the most likely diagnosis?
Explanation
Question 46
During a limited fasciectomy for Dupuytren's contracture, a surgeon meticulously dissects the spiral cord. The spiral cord alters normal anatomy by displacing the neurovascular bundle in which direction?
Explanation
Question 47
A 32-year-old woman sustains an isolated capitellum fracture that extends medially to include the lateral trochlear ridge (Dubberley Type 1B). What is the preferred surgical approach for optimal open reduction and internal fixation?
Explanation
Question 48
A 21-year-old collegiate baseball pitcher complains of vague posterior shoulder pain. Exam reveals 20 degrees of internal rotation and 130 degrees of external rotation. Which anatomic structure is most likely pathologically contracted?
Explanation
Question 49
A 26-year-old motorcyclist falls onto an extended wrist. Lateral radiographs show a 'spilled teacup' sign with the lunate displaced volarly. The capitate is aligned with the radius. What is the correct diagnosis?
Explanation
Question 50
A 24-year-old football player grabs an opponent's jersey and feels a pop in his ring finger. He cannot actively flex the DIP joint. Radiographs show a bony avulsion resting at the level of the PIP joint. What is the Leddy and Packer classification and optimal timing for surgery?
Explanation
Question 51
A 50-year-old woman with type 1 diabetes mellitus presents with recalcitrant adhesive capsulitis. After 9 months of failed physical therapy and intra-articular corticosteroid injections, she elects for surgery. What is the most appropriate next step in management?
Explanation
Question 52
A 13-year-old male gymnast presents with lateral elbow pain and clicking. MRI demonstrates osteochondritis dissecans (OCD) of the capitellum with an unstable, detached osteochondral fragment resting in situ. What is the most appropriate management?
Explanation
Question 53
A 30-year-old manual laborer has progressive dorsal wrist pain. X-rays reveal Kienbock's disease with sclerosis and collapse of the lunate, proximal migration of the capitate, and early secondary arthritic changes. The ulna variance is negative. What is the Lichtman classification and corresponding management?
Explanation
Question 54
A 45-year-old construction worker with chronic anterior shoulder pain exhibits a positive Speed's test. MRI reveals a Type II SLAP lesion with significant macroscopic degeneration of the biceps anchor. What is the most reliable surgical option?
Explanation
Question 55
A 72-year-old female presents with chronic right shoulder pain and an inability to actively raise her arm above 60 degrees. Radiographs, similar to those seen in advanced rotator cuff tear arthropathy, demonstrate superior migration of the humeral head with articulation at the acromion.
What is the most appropriate surgical intervention to restore functional elevation in this patient?
Explanation
Question 56
In the surgical management of a "terrible triad" injury of the elbow, which of the following represents the most accepted sequence of repair after exposing the joint?
Explanation
Question 57
A 55-year-old manual laborer presents with chronic dorsal wrist pain. Radiographs demonstrate advanced narrowing of the capitolunate joint, with relative sparing of the radiolunate joint.
This presentation is most consistent with which stage of Scapholunate Advanced Collapse (SLAC)?

Explanation
Question 58
A 22-year-old rugby player sustained a closed avulsion of the flexor digitorum profundus (FDP) tendon of the ring finger. Radiographs show no fracture. The tendon is palpable in the palm. What is the Leddy-Packer classification and maximum recommended time frame for primary repair?
Explanation
Question 59
A 45-year-old patient with type 1 diabetes mellitus presents with gradual onset of shoulder stiffness. Examination reveals a significant loss of active and passive external rotation with the arm at the side. What is the primary pathologic mechanism?
Explanation
Question 60
A 70-year-old man presents with an inability to actively raise his right arm above 40 degrees, despite intact passive range of motion. Radiographs reveal superior migration of the humeral head with articulation against the acromion and severe glenohumeral osteoarthritis.
Which of the following surgical options is the most appropriate management for this patient?
Explanation
Question 61
A 25-year-old male presents with a 9-month-old scaphoid waist fracture nonunion. MRI demonstrates no avascular necrosis of the proximal pole, and radiographs show no radiocarpal arthritis (SNAC wrist stage 0). What is the most appropriate surgical management?
Explanation
Question 62
A 35-year-old woman sustains a 'terrible triad' injury of the elbow (elbow dislocation, radial head fracture, and coronoid fracture). Surgical fixation is planned. What is the generally accepted sequence of repair to restore stability?
Explanation
Question 63
A 45-year-old female with poorly controlled diabetes mellitus presents with a 4-month history of severe shoulder pain and progressively restricted active and passive range of motion. Radiographs are normal. What is the classic pathologic finding associated with this condition?
Explanation
Question 64
A 32-year-old manual laborer presents with dorsal wrist pain. Radiographs reveal sclerosis of the lunate without collapse, and negative ulnar variance (Lichtman Stage II Kienboeck disease). What is the most appropriate definitive surgical treatment?
Explanation
Question 65
During a single anterior-incision repair of a distal biceps tendon rupture using an endobutton technique, the patient is at highest risk for iatrogenic injury to which of the following nerves?
Explanation
Question 66
A hand surgeon is repairing a Zone II flexor tendon laceration. To optimize tensile strength for an early active motion protocol while minimizing tendon gliding resistance (work of flexion), what is the optimal suture construct?
Explanation
Question 67
A 22-year-old male presents with recurrent anterior shoulder instability. A pre-operative 3D CT scan demonstrates 28% anterior glenoid bone loss. Which of the following procedures provides the most reliable long-term stability?
Explanation
Question 68
A patient with severe, longstanding carpal tunnel syndrome undergoes a carpal tunnel release. Due to profound thenar atrophy, an opponensplasty using the flexor digitorum superficialis (FDS) of the ring finger is performed. To optimize the vector for thumb opposition, the transfer should be routed around which structure?
Explanation
Question 69
A 20-year-old collegiate baseball pitcher is diagnosed with a full-thickness tear of the ulnar collateral ligament (UCL) of the elbow. Reconstruction is planned to restore valgus stability. Which specific ligamentous band must be reconstructed?
Explanation
Question 70
A 28-year-old female presents with persistent ulnar-sided wrist pain after a fall on an outstretched hand. MRI confirms a Palmer Class 1B tear of the triangular fibrocartilage complex (TFCC). After failing conservative management, what is the best surgical intervention?
Explanation
Question 71
During arthroscopic repair of a posterior SLAP tear, the surgeon must be cautious when placing suture anchors or drilling into the posterior glenoid neck. Penetrating the posterior glenoid neck medially by more than what distance puts the suprascapular nerve at significant risk?
Explanation
Question 72
A 60-year-old man undergoes limited fasciectomy for severe Dupuytren's contracture involving the ring finger. During the dissection, the surgeon carefully traces the neurovascular bundle. Which specific cord is primarily responsible for contracture of the proximal interphalangeal (PIP) joint and typically displaces the digital nerve centrally and superficially?
Explanation
Question 73
A 26-year-old man falls from a roof and presents with severe wrist pain. Lateral radiographs show a 'spilled teacup' sign, indicative of a volar lunate dislocation. According to the Mayfield classification of progressive perilunate instability, what is the correct sequence of ligamentous failure?
Explanation
Question 74
A 50-year-old female presents with severe ulnar neuropathy at the elbow. Intraoperative examination reveals that the ulnar nerve actively subluxates over the medial epicondyle during elbow flexion. What is the most appropriate surgical management?
Explanation
Question 75
A 74-year-old woman presents with severe right shoulder pain and an inability to raise her arm above shoulder level. Radiographs reveal superior migration of the humeral head with an acromiohumeral distance of 4 mm. MRI confirms a massive, retracted rotator cuff tear involving the supraspinatus and infraspinatus with advanced fatty infiltration. What is the most appropriate surgical treatment?
Explanation
Question 76
A 70-year-old woman presents with severe right shoulder pain and an inability to raise her arm above the horizontal level for the past 6 months. Examination demonstrates active forward elevation to 70 degrees, but passive forward elevation to 150 degrees. Radiographs reveal advanced glenohumeral osteoarthritis with superior migration of the humeral head articulating with the acromion. What is the most appropriate surgical management?
Explanation
Question 77
A 45-year-old man falls on his outstretched hand and sustains a 'terrible triad' injury of the elbow. He undergoes operative management for a posterolateral elbow dislocation, radial head fracture, and a type II coronoid fracture. Which of the following represents the most appropriate sequence of surgical reconstruction for this injury pattern?
Explanation
Question 78
A 38-year-old man presents with chronic wrist pain. Radiographs demonstrate a scaphoid nonunion with advanced collapse (SNAC). Imaging shows arthritic changes involving both the radioscaphoid and capitolunate joints, while the radiolunate joint is entirely spared. Which of the following is the most appropriate surgical intervention?
Explanation
Question 79
During a flexor tendon repair in Zone II of the hand, maintaining the integrity of the flexor tendon sheath is critical. Which of the following pulley combinations is considered most essential to prevent bowstringing of the flexor tendons?
Explanation
Question 80
A 22-year-old rugby player presents with recurrent anterior shoulder instability. A CT scan of the shoulder reveals 25% anterior glenoid bone loss. The surgeon plans a Latarjet procedure. This procedure provides dynamic anterior stability through a 'sling effect' primarily involving the interaction between the lower subscapularis and which of the following structures?
Explanation
Question 81
A 20-year-old collegiate baseball pitcher feels a pop in his medial elbow during a pitch. MRI confirms a complete distal avulsion of the ulnar collateral ligament (UCL). The primary restraint to valgus stress at the elbow during the late cocking and early acceleration phases of throwing is the:
Explanation
None
